


Sandra Tagliolatto; Patricia F. França; Kennya Macedo Pereira dos Santos
Received on: 10/03/2020
Approved on: 12/05/2020
Financial support: Dr. Patricia Felipe França is Pharmaceutical Consulting Manager at Fórmula & Cia, the pharmacy responsible for the samples handled and used in this protocol. Dr. Kennya Macedo Pereira dos Santos is a technical-commercial consultant at Gemini Indústria de Insumos Farmacêuticos Ltda, responsible for the samples of the probiotic bacterium Lactobacillus plantarum GMNL06.
Conflict of interest: None
Study conducted at the Dermoclínica, Dermatologia e Laser, Private Clinic, Rua Luzitana, 740 4A, Campinas (SP), Brazil
INTRODUCTION: Acne vulgaris, considered a chronic inflammatory and multifactorial disease, presents several therapeutic options. The use of probiotics is a good adjunctive treatment option due to its anti-inflammatory effect.
OBJECTIVE: Based on the promising character of these studies, which derive mostly from oral probiotic therapy, we decided to investigate what results could come from the topical use of a probiotic bacterium that has undergone the tyndallization process.
METHODS: In this study, we demonstrated the topical use of Lactobacillus plantarum GMNL06, alone, for three months.
RESULTS: We obtained a therapeutic response considered good or very good in 90% of mild or moderate acne cases.
CONCLUSIONS:Vulgar acne, considered a chronic inflammatory and multifactorial disease, presents several therapeutic options. The use of probiotics has become an adjunct treatment due to its anti-inflammatory effect. In this study, we demonstrated that the use of topical probiotics, in monotherapy, for three months obtained therapeutic response considered good or very good in 90% of mild or moderate acne cases.
Keywords: Probiotics; Bacteria; Acne; Treatment
Acne is an inflammatory dermatosis of the pilosebaceous follicle. It has the following fundamental characteristics: the hyperproduction of glandular sebum, quantitative and qualitative changes in sebum, Cutibacterium acnes increased colonization, follicular hyperkeratinization, and release of inflammation mediators in the follicle and dermis adjacent. It is a frequent disease that has a chronic course, affecting adolescents and adults, mostly men, but it usually persists in adulthood in about 50% of individuals.1,2
The psychological and social impact of acne can lead to depression and anxiety, and its treatment is critical.2,3
Different etiopathogenic factors are involved, such as follicular hyperkeratinization, sebaceous hypersecretion, skin microbiome changes, immunological factors, inflammatory process, in addition to other conditions that can influence the skin condition, such as diet and changes in the intestinal microbiome.4
Currently, it is considered that the inflammatory process is present in all phases of the pathophysiology of acne, since before the comedone formation.1
Cutibacterium acnes is a Gram-positive, anaerobic bacterium of the genus Corynebacterium and is part of the skin’s healthy resident microbiota. The proliferation of this bacterium occurs when the gland overproduces sebum, favoring the appearance of acne. In acne patients, C. acnes can reach 120.00 specimens/cm on the skin surface.2
The combination of seborrhea and follicular hyperkeratinization produces a favorable environment for C. acnes development, which is found in the skin microbiota and is not pathogenic under normal circumstances.5
Microbiome is the microbial community that occupies a habitat, composed of billions of bacteria, fungi, and viruses.
The human microbiota is established after birth, dominated by bifidobacteria, and stabilizes between the second and third years of life.
Commensal bacteria have greater importance and are involved in the synthesis of specific vitamins, the development and activation of the immune system, and the inhibition of colonization of certain pathogens.
In short, the intestinal microbiota plays a fundamental role in various metabolic, nutritional, physiological, and immunological processes. On the other hand, microbial communities in the organism can influence the pathogenesis of multiple diseases.6
Many conditions related to the microbiome's changes have already been identified, such as obesity, autism, inflammatory bowel disease, atopic dermatitis, and several other diseases, as well as changes in the intestinal microbiota of patients with acne vulgaris. It is assumed that the patient with acne is even more at risk of gastrointestinal discomfort.7
Studies of the intestinal microbiome on the organism and its role in the acne's inflammatory process led to the development of a principle called “gut - brain – skin axis”. Based on this mechanism, it was postulated that the intestinal microbiome’s improvement is shown as a new strategy in the treatment of acne.
However, the microbiome is not limited to the intestine. A review published in 2019, assessing the role of the microbiome in acne, addressed the skin's function as the first line of defense against external agents. It also approaches how, in addition to the skin’s physical barrier, there is also a need to protect the skin's microbiome to keep it balanced and capable of combating possible pathogens such as C. acnes. The review deepens, including addressing specifically the skin microbiome, considering it as an essential part of human health, as dysbiosis could cause or aggravate skin problems. It is believed that probiotics can modify the pathophysiological factors that contribute to acne.8
The World Health Organization (WHO) has been considering probiotics as a more attractive alternative therapy than antibiotics since they do not induce resistance. Probiotics are defined as living microorganisms that, when administered in adequate amounts, can benefit the host’s health.
Currently, probiotics are commercialized as nutraceuticals, nutricosmetics, and functional foods, even though Brazil does not recognize this terminology and consider them food supplements. These nomenclatures, however, are widely used both nationally and internationally.2,7
Probiotics can balance the intestinal microbiota, restoring normal intestinal permeability. Recently, research has shown that probiotics' use not only offers localized effects in the intestine, such as altering the local pH to create an environment unfavorable to pathogens and favorable to their proliferation but also exerts systemic effects.2,9
Studies show the action of probiotics in reducing plasma markers of inflammation and oxidative stress, as well as their action in improving the intestinal barrier's immune function and decreasing the production of pro-inflammatory cytokines (IL) 1,2,6,8 and TNF and stimulation of Toll-like receptors (TLRs).
Regarding its clinical action, effects have been reported in reducing blood pressure, decreasing cholesterol levels, better absorbing certain nutrients, acting, for example, in improving the use of lactose, also acting in relieving the symptoms of intolerance. They also control intestinal infections, as well as stimulate intestinal motility, leading to the consequent relief of constipation and presenting even an anticarcinogenic effect.2
There are also reports of improvement in the immune system by stimulating the production of antibodies, increased secretion of gamma-interferon (IFN ) in patients with atopic dermatitis and allergy to cow's milk, in addition to the competitive exclusion of the antimicrobial compounds’ production.2
Although the different actions of probiotics are recognized, their mechanisms of action have not yet been fully elucidated. Various processes are suggested that can act independently or associated, such as competition for adhesion sites, which ends up forming a physical barrier against pathogenic bacteria, competition with pathogens for nutrients, stimulation of the immune system, production of bacteriocins against pathogens, aid in digestion, absorption and production of nutrients, action on cellular metabolism, reducing the concentration of ammonia in the body, and release of enzymes such as lactase.2
Regarding its safety profile, the probiotic to be marketed needs to present a low risk of systemic infection and production of harmful toxins, not offering an excessive stimulus to the immune response and not allowing the transfer of genes between microorganisms.
As they are living cells, they must be used in adequate quantities; the bacterium must also have internationally known identification; exercise clinically proven benefits to the user demonstrated in vivo and in vitro; survive the attacks of gastric acid and bile salts, ensuring they are alive and active when they reach the site of action; besides having the guarantee of maintaining viability until the moment of consumption in the form of capsule, powder, or when added to dairy products.2
We should also highlight that, to guarantee their continuous effect, probiotics must be ingested daily. The required dose varies according to the strain and product and can promote benefits in very low or very high doses, with clinical studies always showing the health benefits.2
The National Health Surveillance Agency (ANVISA) determines that the minimum viable quantity for probiotics is between 108 and 10¿UFC (Colony Forming Units) in the daily recommendation of the product.2
Since 1930 theories on the benefits of probiotics and their action on the gastrointestinal system infer that psychological factors could influence the skin.10
Nowadays, it is known that emotional states lead to gastrointestinal dysfunction and changes in bacterial flora, causing local and systemic inflammation. 10
Studies relate emotional stress to the delay in the average time of intestinal transit, the consequent excessive growth of bacteria and the reduction of species of lactobacilli and bifidobacteria.11
Alteration of the intestinal microbiome (dysbiosis) leads to hypochlorhydria and excess bacterial growth, and competition for nutrients leads to the production of toxic metabolites.10
Dysbiosis is also involved in the release of inflammatory and neuromodulatory cytokines (such as substance P).
Substance P acts on the organ itself and at a distance, increasing pro-inflammatory mediators (IL-1, IL-6, TN- F- (PPAR –g).
Substance P promotes both proliferation and differentiation of sebaceous glands, leading to the worsening of acne. No less important fact is that substance P can be released under stress, corroborating the theory of the gut-brain-skin axis.
Also, regarding the immune mechanism, we must emphasize that the increase in IGF-1 is also involved in worsening acne conditions.12, 13,14
Recent studies demonstrate that prebiotics and probiotics can reduce markers of inflammation and oxidative stress.9 Studies have been published demonstrating the effectiveness of using oral probiotics in the clinical improvement of acne.
In addition to improving adherence and tolerability, adverse events are reduced when associated with the use of systemic antibiotics. 15,16
Of the probiotics, Lactobacillus acidophilus is the most studied species in the treatment of acne.17
The first study with lactobacilli to treat acne was published in 1961, in which 300 patients used probiotic strains for 30 days. There was an improvement in 80% of the cases, which showed some degree of clinical improvement (with a higher result in the most inflammatory cases).
This research has its relevance, as it was one of the first published studies to infer a possible link between the cutaneous manifestations of acne vulgaris and metabolic processes in the intestinal tract.2,15,18
Nowadays, several studies have already shown that the presence of circulating endotoxins derived from intestinal bacteria and changes in intestinal permeability may be common in acne.19,20 A study conducted with 40 patients undergoing conventional acne treatment divided them into two groups: 50% of the participants used antibiotics alone, and the other half used antibiotics associated with the probiotic. The assessment showed that the supplement group obtained better results and better tolerance to medications than volunteers who used the antibiotic alone18,21 proving the benefit of the association of probiotics with standard treatment in patients with acne.2
An interesting clinical study demonstrated that the consumption of industrialized dairy drinks fermented with Lactobacillus improved the clinical aspects of acne after 12 weeks.2
A possible mechanism of action of probiotics in acne is based on the fact that the loss of bifidobacteria due to bad eating habits (excessive consumption of fat and sugar) leads to an increased intestinal permeability and endotoxins efflux in the circulation (which consequently lead to inflammation, oxidative stress, and insulin resistance). Thus, the administration of probiotics could then decrease systemic access to endotoxins and reduce reactivity to them.22,23
A regulatory pathway is linked to the modulation of essential cytokines in developing the disease, such as IL 1-alpha (fundamental for follicular hyperkeratosis - obstruction of the glandular ostium).24
We can say that probiotics can regulate the release of inflammatory cytokines in the skin, just as antibiotics can alter the microbiota in places far from the gastrointestinal system.24,25
Another factor to consider is that, in acne, the load of lipid peroxidation is high, generating significant demand for antioxidants (qualitative alteration of sebum production), and the ability of oral probiotics to limit systemic oxidative stress could also be considered a therapeutic path (antioxidant effect).26
A possible relationship between high glycemic index diets and acne exacerbation has also been investigated. It is evident the relationship of some components of the diet (carbohydrates and high glycemic index) and acne.2,18
Systemic probiotics can improve insulin levels, reducing the release of IGF -1, leading to clinical improvement of acne.2,12,18,27
In short, we can point out the action of probiotics in acne treatment due to the reduction of local and systemic inflammation, decreased oxidative stress, maintenance of permeability of the intestinal barrier, and reduced release of substance P, regulation of glycemic control, and improved nutrient absorption.
In 1912, the first report of the use of probiotics directly on the skin (topical use of Lactobacillus bulgaricus) was published, which proved to be useful in the treatment of acne and seborrhea.
A study, conducted for only seven days, used probiotic in the form of cream to demonstrate that lactic acid-producing bacteria could increase the production of ceramides, which are recognized for having anti-microbial activity against C. acnes, in addition to anti-inflammatory activity. In another clinical study, the application of ceramide promoted a significant reduction of papules and pustules after two months of treatment.2
Studies have shown the value of topical therapy with probiotics Bifidobacterium longum and Lactobacillus paracasei to attenuate the inflammation mediated by substance P in the skin (remembering that substance P is a primary mediator, induced by stress, leading to inflammation and sebum production in acne).2
The application of selected probiotic bacteria to the skin can offer a protective effect, similar to a physical barrier, through the competitive inhibition of binding sites to prevent colonization by other pathogenic bacterial strains.2
It is known that living microorganisms are sensitive to heat and the presence of water and can become a challenge for pharmaceutical forms such as creams. Due to this characteristic, our study sought to use tyndallized bacteria.
Tyndallized bacteria can be defined as microorganisms or non-viable microbial cells, obtained from probiotics. The tyndallization process consists of a fractional sterilization method in which temperatures between 80 °C and 100 °C are applied to the microorganism. Heat-treated probiotics can confer immunomodulatory effects and assist in the inflammatory response. Thus, they and have been used in respiratory and dermatological pathologies.28
This is a clinical, experimental, prospective, randomized.
The study recruited 28 volunteers. The inclusion criteria were: participants of any age group, ethnicity, or gender, presenting with mild or moderate acne (grades I, II, III).
The exclusion criteria were severe acne (grade IV) and/or patient using other medications to treat acne during the study (three months).
The volunteers' evaluation was photographic and clinical, performed by two examiners.
In the first evaluation, anamnesis and clinical dermatological examination were performed. The acne was classified as grade I - prevalence of comedones; grade II - presence of papules and pustules; or grade III - presence of cystic lesions. On the same day, the photographic record was performed, and the informed consent form and the complete treatment were provided. The treatment was formulated and handled in a compounding pharmacy (Fórmula e Cia, Manipulação Pharmacy, Campinas, São Paulo, Brazil), including cream containing 30 g, with Lactobacillus plantarum GMNL06 in a concentration of 1 billion UFC/g, in a pump bottle, sanitizing lotion composed of saline (Needs®, LBS Laborasa, São Paulo, SP, Brazil) for facial hygiene, and SPF 30 sunscreen in aristoflex gel.
The patient was instructed to use the cream containing Lactobacillus plantarum GMNL06, twice a day, in the morning and at night, for 90 days. Patients were also instructed to return every 30 days for clinical evaluation and photographic record, in addition to receiving treatment for the next month.
Each return was recorded on a form if the patient showed correct adherence to treatment, and, in case he was not using the products in the protocoled manner, he was immediately excluded from the study group.
Upon return from the third month of treatment, patients were assessed and classified according to the scale below:
a) Acne worsening (increase in the number of lesions), zero result (when there was no clinical change in the initial condition with post-treatment);
b) Partial improvement (up to 50% decrease in the number of lesions);
c) Great improvement (more than 50% decrease in the number of lesions).
Two researchers clinically evaluated and classified the patients.
Of the 28 selected patients, seven were men, and 21 were women.
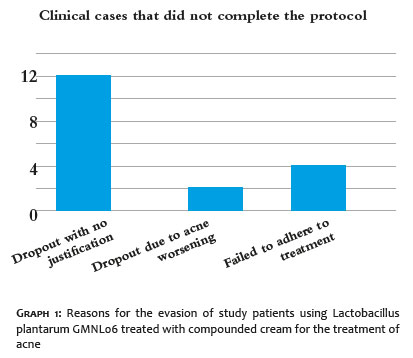
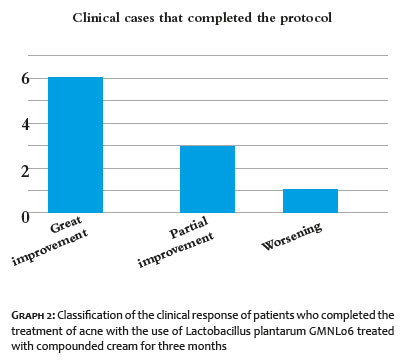
The age ranged from 13 to 46 years (average 29.5 years). Eighteen patients did not complete the study, and, most of these voluntary dropouts (12) gave up treatment without giving any reason and did not attend the returns or did not answer our calls. Two dropout volunteers reported worsening of the clinical condition and, therefore, discontinued its use. Four dropout volunteers stated that they were unable to adhere correctly to the treatment. Of these, one volunteer reported liking the result of using the probiotic and was classified as having much improvement since the first month of follow-up (Graph 1). Of the ten patients who completed the three months of protocol treatment, one presented acne worsening; none was classified as zero result; three partially improved; and six were classified as great improvement (Graph 2) (Figure 1).
Of these 10 patients, nine were classified, at the beginning of the protocol, as grade I acne and one as grade II acne.
There were no reports of adverse events such as scaling, itching, burning, or erythema.
Lactobacillus plantarum GMNL06 is a probiotic bacterium (sterilized), that is, heat-treated. During heat treatment, bacteriocins are released from cell membranes and perform the “antibiotic-like” action.28 Bacteriocins are proteins with antimicrobial activity that act by inhibiting the growth of Cutibacterium acnes.29,30,31
Few studies have been conducted with Lactobacillus plantarum for acne and with topical use, which denotes the relevance of the present study.
In the theoretical research conducted for the present study, the most relevant study was a clinical trial aimed at treating acne. It was conducted with another lineage of the same genus and species, Lactobacillus plantarum GG, also heat-treated, in the form of cream, with 29 women volunteers, aged between 25 and 55 years. The authors considered the effects promising in reducing the erythema caused by acne and in the intensity of the lesions.32
Based on our observations and the literature, we can cite as possible mechanisms of action of Lactobacillus plantarum GMNL06:
1) Epithelial action:33
- Improved barrier function in the epithelial layer;
- Pathogens’ competition for the receptor site in epithelial cells.
2) Immunomodulatory action:34
- Prevention of the immune-inflammatory response, by increasing the anti-inflammatory cytokines;
- Stimulation of the immune response;
- Differentiation of B cells, formation of IgA.
3) Increased resistance to pathogens:35
- Inhibition of pathogen adherence by competition;
- External membrane proteins with bactericidal effect.
The interest of this research in using Lactobacillus plantarum GMNL06 in the tyndallized form was the possibility of applying it in a compounded formulation for topical use, opening the range of options for professionals in the treatment of acne both as monotherapy and combined with other treatment strategies.
Studies corroborate the fact that tyndallized probiotic bacteria can modulate the growth of pathogenic microorganisms, favoring skin homeostasis.35 The use of probiotics for their anti-inflammatory action can be considered a therapeutic option in acne treatment.8 In our study, we chose to study the use of topical, probiotic bacterium, topical, in monotherapy, to treat mild or moderate acne.
This study's option to use Lactobacillus plantarum GMNL06, as monotherapy, apparently showed a slower improvement process in the skin condition, and we assume that this may have caused the abandonment of the protocol by some volunteers, after the first month of treatment. Another hypothesis for the protocol abandonment was that the protocol used establishes the use of the formulation twice a day. This hypothesis, in our analysis, may have contributed to the cases of non-adherence to the proposed protocol. Despite this, we must emphasize that, even within the group of volunteers who gave up treatment because they were not able to follow the protocol correctly, there was a case of clinical improvement considered as a great improvement in the first month of using Lactobacillus plantarum GMNL06.
An important fact to be highlighted is that, among the volunteers who managed to follow the protocol by the end of the third month, the majority (60% of the cases) showed improvement classified within the scale established for study as great improvement.
If we combine this result with partial improvement cases, it is possible to state that we obtained a 90% satisfactory result within the proposed protocol. That in the framework of acne for the portion of volunteers that fully adhered to the protocol for the use in monotherapy of Lactobacillus plantarum GMNL06, compounded cream, dispensed in a pump bottle, twice daily
In clinical practice, acne is treated with specific sanitizers for oily/acneic skin, association of topical keratolytic and/or bactericidal products and, in cases of more pustular acne, with the introduction of systemic medications. There are also complementary procedures, such as the removal of comedones, chemical peels, microdermabrasions, phototherapy, and others, for three months or more. We emphasize that none of these strategies were used during the proposed protocol so that there was no interference in the results obtained and data collected.
In our evaluation, there are many advantages in the use of probiotic bacteria tyndallized in a topical cream for acne. It did not induce bacterial resistance and did not cause discomfort or skin irritation, according to what we could observe in our study. This feature enables associating it with other products for acne treatment, which may enhance the speed of results. Because Lactobacillus plantarum GMNL06 does not produce photosensitization, this strategy used in our protocol presents as an interesting and effective therapeutic option for patients who are overexposed to sunlight or who have sensitive skin to conventional treatments.
Based on our data analysis and the results collected in our protocol, we could conclude that the topical use of Lactobacillus plantarum GMNL06 in compounded cream proved to be a safe and effective procedure in the treatment of mild and moderate acne, even as monotherapy. It didn't present skin irri
Sandra Tagliolatto | 0000-0003-22-03-0692
Data collection, analysis, and interpretation; active participation in research orientation; preparation and writing of the manuscript.
Patricia F. França | 0000-0002-2047-4161
Active participation in research orientation; preparation and writing of the.
Kennya Macedo Pereira dos Santos | 0000-0003-4756-9344
Study design and planning; critical revision of the manuscript.
1. Casari A, Pellacani G, Seidenari S, Cesinaro AM, Beretti F, Pepe P, et al. Pigmented nodular basal cell carcinomas in differential diagnosis with nodular melanomas: confocal microscopy as a reliable tool for in vivo histologic diagnosis. J Skin Cancer. 2011. Epub 2010 Oct 14.
2. Altamura D, Menzies SW, Argenziano G, Zalaudek I, Soyer HP, Sera F, et al. Dermatoscopy of basal cell carcinoma: morphologic variability of global and local features and accuracy of diagnosis. J Am Acad Dermatol. 2010;62(1):67-75.
3. Charles CA, Marghoob AA, Busam KJ, Clark-Loeser L, Halpern AC. Melanoma or pigmented basal cell carcinoma: a clinical-pathologic correlation with dermoscopy, in vivo confocal scanning laser microscopy, and routine histology. Skin Res Technol. 2002;8(4):282-287.
4. Menzies SW, Westerhoff K, Rabinovitz H, Kopf AW, McCarthy WH, Katz B. Surface microscopy of pigmented basal cell carcinoma. Arch Dermatol. 2000;136(8):1012-1016.
5. Argenziano G, Longo C, Cameron A, Cavicchini S, Gourhant JY, Lallas A, et al. Blue-black rule: a simple dermoscopic clue to recognize pigmented nodular melanoma. Br J Dermatol. 2011;165(6):1251-5.
6. Menzies SW, Crotty KA, McCarthy WH. The morphologic criteria of the pseudopod in surface microscopy. Arch Dermatol. 1995;131(4):436-40.
7. Longo C, Farnetani F, Moscarella E, Pace B, Ciardo S, Ponti G, et al. Can noninvasive imaging tools potentially predict the risk of ulceration in invasive melanomas showing blue and black colors? Melanoma Res. 2013;23(2):125-31
8. Peccerillo F, Mandel VD, Di Tullio F, Ciardo S, Chester J, Kaleci S, et. al. Lesions mimicking melanoma at dermoscopy confirmed basal cell carcinoma: evaluation with reflectance confocal microscopy. Dermatology 2019;235(1):35-44.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}