


Flávia Rodrigues Dias; Vitória Culau Merlo Milani; Hanna Raíssa Cardoso Guimarães; Ursula Metelmann
INTRODUCTION: The lips have a huge importance in facial aesthetics, and the use of fillers to improve the region is growing with a variety of different techniques described.
OBJECTIVE: To report the experience with the "lip tenting" lip filling technique.
METHODS: 20 female patients between 18 and 60 years of age obtained lip filling through vertically serial punctures from the lip vermilion border, depositing a small amount of product by retroinjection, in the superficial muscular plane.
RESULTS: All treated patients reported a high degree of aesthetic satisfaction with the result of the procedure, with edema and local ecchymosis transiently present in most patients.
CONCLUSIONS: This is an easy execution technique compared to other filling techniques, presenting very satisfactory aesthetic results.
Keywords: Anatomy; Lip; Rejuvenation
The lips play an essential role in the aesthetic perception of the face. Historically, bulky lips are associated with youth and beauty, especially in women. Aesthetic patterns vary between cultures and over time. Currently, there is a preference for thick, natural-looking lips, proportional to other facial features, with a well-defined red border and balance between the dimensions of the upper and lower lips.1,2,3 Filling materials are used to increase soft tissues, improve unsightly characteristics, and replace lost volume in the aging process.4 There is a growing demand for lip filling procedures, using different techniques and substances.
In the international literature, Eijik et al. described a lip filling technique called Lip Tenting, which consists of injecting the filler almost vertically into the lips from the outline (the white line that borders the top of the upper). This technique allows increasing the volume, elevation, and projection of lips contour, simultaneously, with each “stroke” of the injection.5 We report the experience with this technique.
This is a prospective, interventional study, in a series of cases, developed with selected participants at the Dermatology Clinic of the Hospital Padre Bento of Guarulhos. It was conducted respecting the ethical principles established by Resolution 466/12 of the National Health Council, including analysis by the Research Ethics Committee - CEP/ Hospital Padre Bento de Guarulhos (CHPBG) through the Brazil Platform, approved under number 3.039.220 on 09/18/2014. We requested authorization to patients through the free and informed consent term and authorization term for the use of images.
This was a self-financed research. The researchers funded all products used.
The inclusion criteria were: women; age between 18 and 60 years; with the desire to increase lip volume or correct unsightly asymmetries and disproportions. The exclusion criteria were: prior lip filling; participants with unrealistic expectations of treatment; psychiatric disorders; pregnant women; decompensated autoimmune or metabolic diseases; immunosuppression; and anticoagulants use.
Initially, an evaluation of each patient's individual characteristics was conducted to establish a treatment plan, aiming to improve the contour, volume, and asymmetries of each case. The patients were evaluated in an orthostatic position, with demarcation of the lips parallel to the line drawn between the pupils. As for the spatial location, the upper lip must be 18-20mm from the nose and the lower lip 36-40mm from the chin. The desired relationship in the lip-chin complex is the upper lip projecting approximately 2mm more than the lower lip in relation to the vertical facial plane. In women, the chin's most protruding point should be in a position slightly posterior to the lower lip. In men, on the contrary, in a slightly anterior projection. The lips need to maintain a natural profile. The nasolabial angle should be approximately 95° to 100° in women and 90° to 95° in men.6
Photographs were taken before, immediately after, and 30 days after the application of lip filling. Also, patients were interviewed before and 30 days after treatment, to establish the degree of satisfaction. The data were analyzed comparing the volumization improvement and the lips contour definition subjectively by the patient, based on the interviews, and by the injectors, through the photos taken throughout the study.
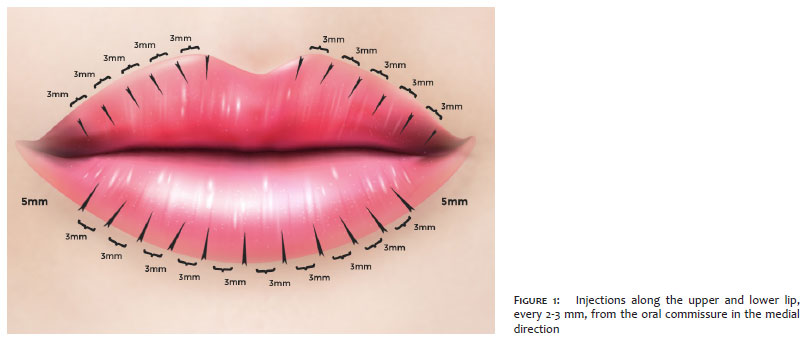
The procedure initiated by local asepsis with 2% aqueous chlorhexidine, followed by anesthetic nerve block with 2% lidocaine without vasoconstrictor, from the branches of the infraorbital nerve, right and left, and the branches of the right and left mental nerves. The hyaluronic acid filler without lidocaine (Restylane® | Galderma) was injected using a 29G needle (0.33x12 mm). The puncture started at the contour (the structure that insinuates between the labial vermilion and the skin junction), inserting the needle vertically towards the transition between dry and wet mucosa. The product was retro-injected, depositing 0.01 ml to 0.02 ml of volume per stroke, in the superficial muscular plane. The injections were repeated along the upper and lower lips, every 2-3 mm, from the oral commissure in the medial direction, except for the lip filter. (Figure 1). A total of 1 ml of hyaluronic acid was injected into each patient.
After the end of the procedure, local cleaning was performed with 0.9% saline. Participants were instructed not to manipulate the site, perform ice packs for five minutes, five times a day, for five days, and not to practice physical activity, as well as immersion bath, pool, or sea in the first 48 hours. Patients were photographed before the procedure and immediately after.
Twenty female patients, aged between 18 and 58 years, were treated. Of the sample, 60% reported mild discomfort/pain at the time of the maxillary nerve block, with comfort after the anesthetic effect started; 40% reported comfort to perform the entire procedure. Some degree of edema, erythema, and pain were observed in 100% of patients on the first and second days after the procedure, although tolerable. They all returned to their routine activities promptly.
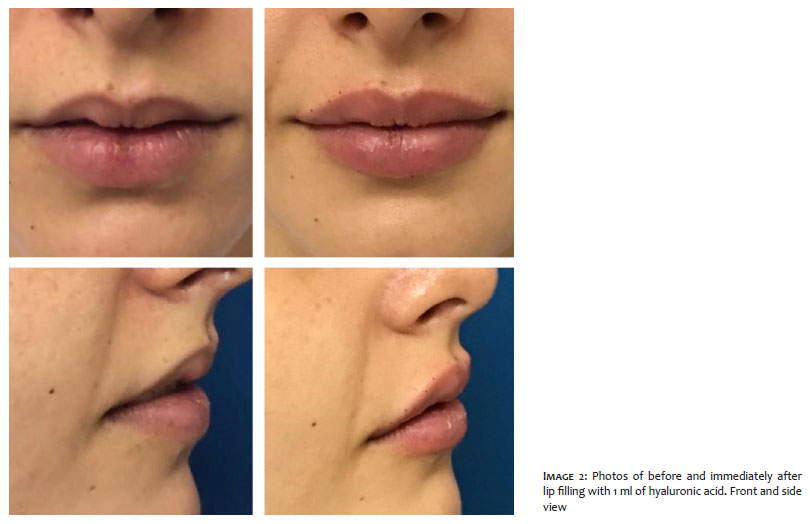
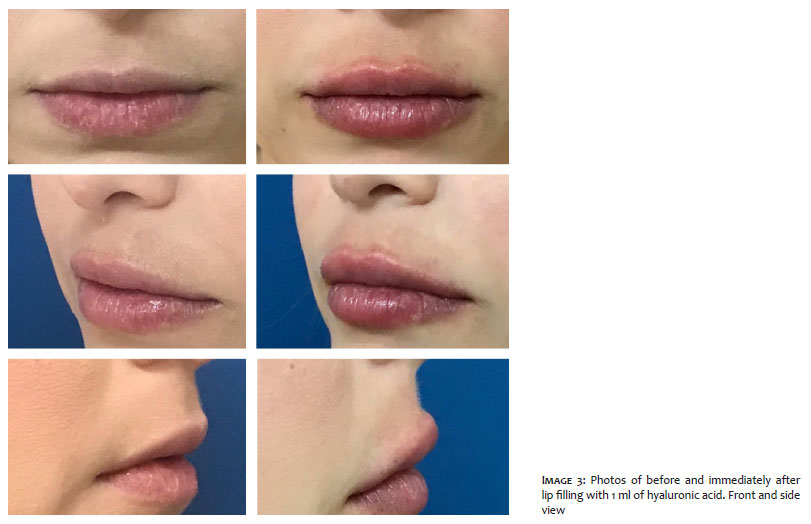
Eighty percent of patients presented ecchymosis in some puncture site, with complete resolution within seven days. There was no case of vascular occlusion or other adverse events. At the end of the study, 100% of the sample reported a high degree of satisfaction and stated that they would repeat the procedure when necessary. One hundred percent reported that they would indicate lip filling for a friend or relative (Images 1, 2, 3, 4: before and after [immediately after] of the procedures in four selected patients).
Lip filling is a procedure with increasing demand, aiming to improve unsightly characteristics and/or replace lost volume in the aging process. The reasons for dissatisfaction with each individual’s labial aspects vary from intrinsic causes, such as lips considered small, thin, asymmetrical, disproportionate, changes resulting from aging, even external influences, such as the aesthetic pattern of fashion, media, or celebrities. However, the result is often not satisfactory, leading to the discouragement of both professionals and patients to perform such a procedure. Thus, there are challenges for professionals to develop appropriate and safe techniques that adjust to the specific concerns, desires, and anatomy of each patient.
Hyaluronic acid is the substance of choice when used by qualified and adequately trained injectors. It stands out for being moldable, safe, producing immediate and lasting results, but not permanent, and being reversible with the use of hyaluronidase. The duration of the result depends on the product used, with several presentations available with different degrees of cohesiveness and viscosity. This guarantees great versatility in the application. It is biologically pure, with low protein loads, biocompatible, and biodegradable. The absence of animal proteins eliminates the need for skin tests.6,7 To obtain an aesthetically pleasing result in lip filling, it is essential to understand the proper architecture of the face in relation to the lips. Although there is no ideal technique for obtaining a “perfect” lip or a “standard” approach to lip augmentation, there are some basic concepts that lead to natural and aesthetically pleasing results.
From hundreds of years ago, basic artistic principles still apply today, and are based on the structure of Phi - the Divine Proportion - 1:1.618, which reveals the ideal balance and symmetry relationship.
Leonardo DaVinci in his anatomical studies used corpses to measure the proportions of the human body and found that nothing else obeys the divine proportion as much as the human body. According to DaVinci, in the perfect man, dimensions follow the golden ratio.8
Therefore, when studying and performing measures for ideal aesthetic procedures, these proportions are used.
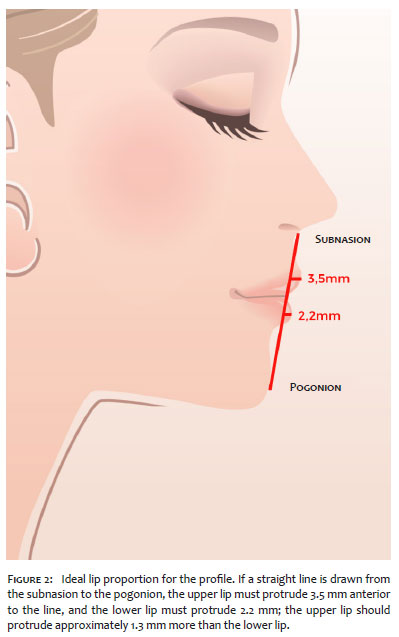
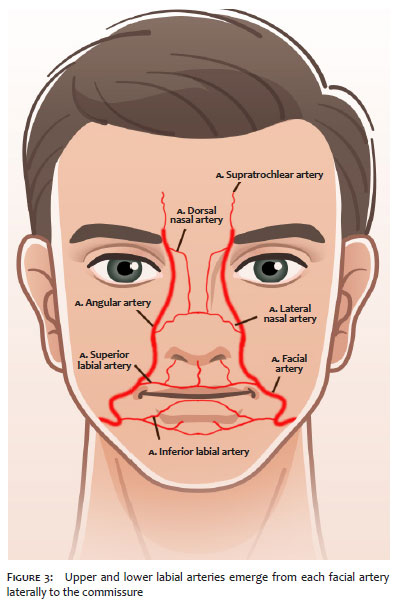
The face is divided horizontally into thirds: upper third, middle third, and lower third, all equal in vertical height. The lower third of the face is also horizontally divided into thirds: upper third corresponding to the upper lip and the lower two-thirds corresponding to the lower lip and chin. The ideal lip ratio in Caucasians in the frontal view is 1:1.6, which translates to about 40% of the volume in the upper lip and 60% of the lower lip volume. Also, the width of the mouth horizontally must be equal to one and a half times the nose's width.9 In the lateral view, if a straight line is drawn from the subnasion to the pogonion (the most anterior point of the chin), the upper lip should protrude 3.5mm anterior to the line, and the lower lip should protrude 2.2mm; the upper lip should protrude approximately 1.3mm more than the lower lip10 (Figure 2). An exaggeration of these proportions or the wrong proportion can lead to a "duck mouth" or "sausage lips" appearance. Arterial vascularization of the lips, originating in the external carotid system, is supplied by the upper and lower labial arteries that emerge from the facial artery, laterally to the commissure. The labial artery presents significant variations regarding the pattern of the dominant side, trajectory, and tortuosity, remaining, in most cases, in a posterior plane to the orbicularis oris muscle11 (Figure 3).
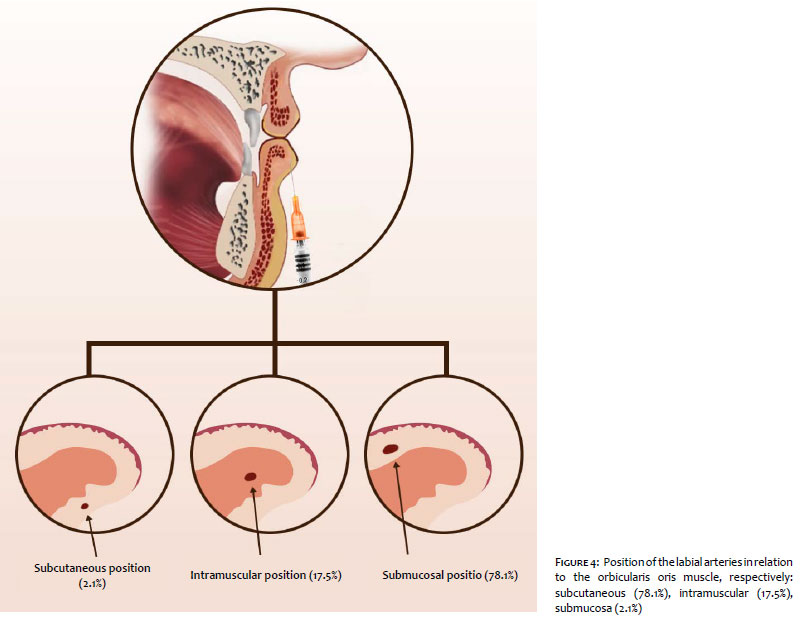
A large multicenter anatomical study was conducted to identify the position of the labial arteries in relation to the orbicularis oris muscle. Three distinct artery positions were identified: submucosa (between the oral mucosa and the orbicularis oris muscle in 78.1% of cases), intramuscular (between the superficial and deep layers of the orbicularis oris muscle in 17.5%), and subcutaneous (between the skin and the orbicularis oris muscle in 2.1%). The plane variability where the artery is located along the labial course was 29% for the upper lip and 32% for the lower lip. The midline was identified on the upper and lower lips as the most variable (Figure 4).12
Based on the results of this investigation, a safer location for the application of the volumizing material is the subcutaneous plane in the paramedian location. The artery can be identified more frequently in superficial positions on the midline, especially on the upper lip.11 Injection into the lips at a depth of less than 3mm at the cutaneous edge of the vermilion can be considered safe for the lips' projection.13
The lips are abundantly provided with sensitive nerve endings. The infraorbital nerve, a branch of the maxillary division of the trigeminal nerve, innervates the upper lip, and the mental nerve, a branch of the mandibular nerve, innervates the lower lip.14 The most commonly described technique for lip augmentation involves inserting a needle or cannula parallel to the horizontal axis of the lips. The instrument is inserted into the lateral mucosa of the lip and directed medially. This provides volume to the lip on the horizontal axis, using either an anterograde, bolus or retrograde injection. It is not uncommon to obtain unsightly results due to the deposit of a considerable amount of material horizontally across the upper and lower lip.5
The Lip Tenting technique reproduced in the reported patients allows good control over the filling’s shape and volume. It is possible to increase the volume, elevate, and edge eversion of the upper and lower lips, resulting in a more natural appearance than often obtained with other methods. Its main indications are patients who want to have increased lip volume, defined contour, correction of asymmetrical lips or anterior suboptimal filling.5
If any asymmetry is detected, you can reinsert the needle vertically at the point of asymmetry and inject a small amount of material to correct it. For example, if the patient wants a more prominent cupid’s bow, simply perform a retroinjection vertically on the upper lip’s vermilion at the top of the cupid’s bow towards the transition between the dry and wet border of the lip.5
The authors observed as a significant differential that the volumization of the lips does not occur horizontally only, but the “strokes” performed form structures similar to pillars that promote an increase in volume vertically together with the projection of the vermilion border, defining the contour and eversing the edges of the lips, which gives the lip an attractive shape, hence the name of the technique, “Lip tenting”. Another important aspect is that the lips, thus filled, show a significant improvement in the “gingival smile”, also justified by the increase in vertical volume.5
A great benefit was observed in restoring the lower third of the face's proportionality, as it is possible to restore the nasolabial angle and distance. When promoting the eversion and projection of the upper lip, there is a decrease in the distance between the nose’s base and the cutaneous-labial mucosa transition line and a reduction in the nasolabial angle. The increase in volume only inside the vermilion prevents the filling above or below the lips, under the perioral skin, promoting a more natural aspect. The result is a nasolabial facelift, non-surgical, with redness enhancement.
We highlight the importance of performing punctures starting at the vermilion border of the lip vertically, always towards the junction of the mucous/submucous, remaining on the superficial muscular plane. As the technique is based on multiple injections, the risks of large localized filler volumes, which give rise to palpable or even visible nodules, are minimal, as well as the risk of vascular occlusion. Thus, it is possible to reduce the risk of both visible artifacts (small nodules) and vascular involvement, whose anatomical topography is posterior to the injected plane (Figure 4). As a disadvantage, we agree with the authors of the technique that it is necessary to perform maxillary nerve block, as patients cannot tolerate multiple punctures with only topical anesthesia. We emphasize that if there are doubts since with the punctures, edema starts during the procedure, it is more appropriate to leave corrections of small asymmetries for the reevaluation after seven to 14 days.
As previously described by Eijik et al., Lip Tenting is a relatively easy technique to be taught and performed, especially for novice injectors who quickly gain the ability to provide the patient with symmetrical lip and with more satisfactory results when compared to other techniques. We agree with this statement; however, we emphasize that more than the manual skill, which is acquired with the learning curve, professionals need a critical aesthetic notion applied to each patient's demands, not only before but also during and after the execution of the procedure.
We emphasize that the technique covered in this publication is a good option for lip filling, but due to the great diversity of techniques, there is no consensus on which is the best of them. When choosing the filler’s application method, one must consider the skill of the physician combined with each patient's needs, always aiming at good aesthetic results and greater safety. Medical knowledge and technical training are essential for the management of possible complications. Further studies should be conducted to corroborate these findings.
Flávia Rodrigues Dias | 0000-0002-2758-147X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Vitória Culau Merlo Milani | 0000-0001-9523-7083
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Hanna Raíssa Cardoso Guimarães | 0000-0002-8063-3945
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Ursula Metelmann | 0000-0002-2446-6417
Active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Niamtu J. New lip and wrinkle fillers. Oral Maxillofac Surg Clin North Am. 2005;17(1):17-28.
2. Klein AW. In search of the perfect lip: 2005. Dermatol Surg 2005;(11 Pt 2):1599-603.
3. Bisson M, Grobbelaar A. The esthetic properties of lips: a comparison of models and nonmodels. Angle Orthod 2004;74(2):162-6.
4. Jorizzo JL, Schaffer JV. Soft tissue augmentation. In: Bolognia J, editor. Text book of dermatology. Philadelphia: Saunders Elsevier; 2012. p. 2547-60.
5. Braun M, Braun S, van Eijk T. Lip tenting: a simple technique for better lip enhancement. J Drugs Dermatol. 2010;9(5):559-60.
6. Trindade de Almeida AR, Sampaio GAA. Preenchimentos e técnicas para o terço superior da face. In: Kadunc B, Palermo E, Addor F, et al. editores. Tratado de cirurgia dermatológica, cosmiatria e Laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 355-60.
7. Carruthers J, Carruthers A. Hyaluronic acid gel in skin rejuvenation. J Drugs Dermatol. 2006;5(10):959-64.
8. Mandy S. Letter: art of the lip. Dermatol Surg. 2007;33(4):521-2.
9. Perkins SW, Sandel HD. Anatomic considerations, analysis, and the aging process of the perioral region. Facial Plast Surg Clin N Am. 2007;15(4):403-7.
10. Legan H, Burnstone C. Soft-tissue cephalometric analysis for orthognathic surgery. J Oral Surg. 1980;38(10):744-51.
11. Tansatit T, Apinuntrum P, Phetudom T. A typical pattern of the labial arteries with implication for lip augmentation with injectable fillers. Aesthetic Plast Surg. 2014;38(6):1083-9.
12. Cotofana S, Pretterklieber B, Lucius R, Frank K, Haas M, Schenck TL, et al. Distribution pattern of the superior and inferior labial arteries: impact for safe upper and lower lip augmentation procedures. Plast Reconstr Surg. 2017;139(5):1075-1082.
13. Scheuer JF, Sieber DA, Pezeshk RA, Campbell CF, Gassman AA, Rohrich RJ. Anatomy of the facial danger zones: maximizing safety during soft-tissue filler injections. Plast Reconstr Surg. 2017;139(1):50e-58e.
14. Rodriguez ED, Losee JE, Neligan PC. Cirurgia plástica: cirurgia craniofacial, cabeça e pescoço e cirurgia plástica pediátrica. - 3rd ed. - Rio de Janeiro: Elsevier; 2015.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}