


Raíssa Rigo Garbin; Gerson Dellatorre; Roberto Gomes Tarlé; Guilherme Augusto Gadens; Alexandre Luiz Weber; Lismary de Forville Mesquita
Received on: 16/04/2020
Approved on: 29/05/2020
Financial support: None
Conflict of interest: None
Study conducted at the Dermatology Service of the Hospital da Santa Casa de Curitiba, Curitiba (PR), Brazil
To accurately interpret intraoperative findings in Mohs Micrographic Surgery, it is essential to know the normal tissue histology of different anatomical sites. The freezing sections evaluated by the technique are obtained horizontally, unlike the vertical sections of conventional anatomopathological analysis. According to the literature review, the frozen sections of interest in topographic histology were digitized and detailed from a training Dermatology service case collection.
Keywords: Histology; Mohs Surgery; Skin Neoplasms
Mohs micrographic surgery (MMS) requires the dermatological surgeon to have extensive knowledge of normal tissue histology and pathological anatomy. The accurate interpretation of the freezing sections usually performed horizontally (in contrast to the vertical sections of conventional anatomopathological analysis), and the knowledge of histological peculiarities of the different anatomical regions are essential for the differentiation between typical structures and intraoperative tumor findings.1 The case collection of an MMS training reference service was reviewed, and the freezing sections of interest in topographic histology were digitized using a Leica DM-1000 microscope and a Leica ICC-50 camera (Leica Microsystems, Wetzlar, Germany).
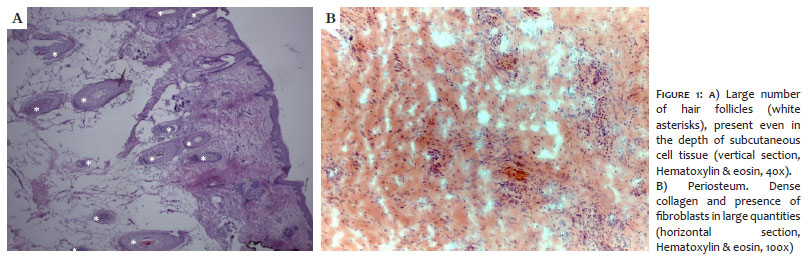
The scalp presents a high density of follicular units, with anagenic terminal follicles implanted deep in the subcutaneous tissue (Figure 1a).2 In horizontal sections, the hair follicle's cross-section results in rounded or oval basophilic structures, which may resemble basal cell carcinoma (BCC) nests. Knowing the characteristics of the different portions of the hair follicle helps in this differentiation.1 A series of layers from the bulb form the hair follicle, often showing a central hair shaft, and, unlike the BCC, it does not usually present a gap between its structure and the adjacent dermis. The outer epithelial layer is composed of monomorphic cells, with a moderate amount of eosinophilic cytoplasm surrounded by fibrous stroma. At the height of the reticular dermis, sebaceous glands are associated with the follicular unit, and its duct marks the division of the upper (infundibulum) and middle (isthmus) hair segment. The follicular unit's connection with the hair erector muscle delimits the division between the middle and lower hair segments (or bulb, which will contain the papilla) and is called a bulge. In the transition between the infundibulum and the isthmus, arciform epithelial cords protrude laterally in relation to the follicle and are called the mantle.2,3
In cases of deeper tumor involvement, it is possible to identify, below the subcutaneous and the galea aponeurotica), dense connective tissue, with collagen fibers and fibroblasts, representing the periosteum (Figure 1b).4
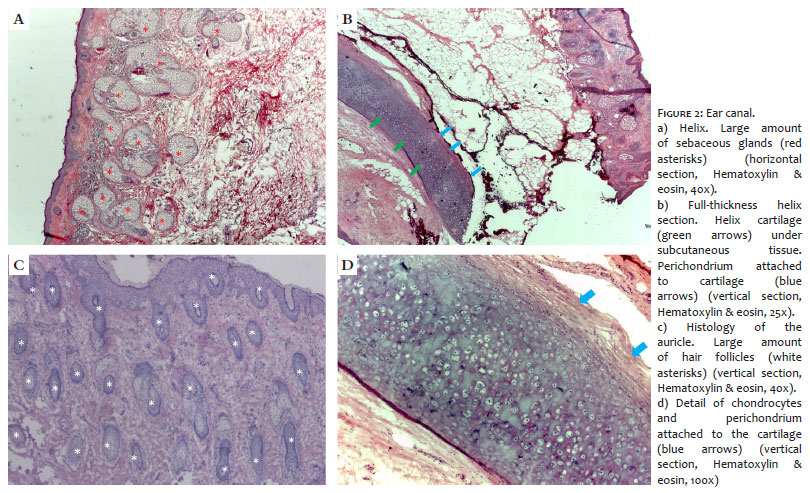
The auricle has its shape determined by the structure of elastic cartilage (Figures 2b and 2d). It is covered by thin skin, hair follicles, sebaceous glands, and eccrine sweat glands, the latter being replaced by cerumen glands at the level of the external acoustic meatus.5,6 The density of attachments is heterogeneous in the different portions of the canal, being more prominent in the area of the auricle (Figures 2a and 2c).
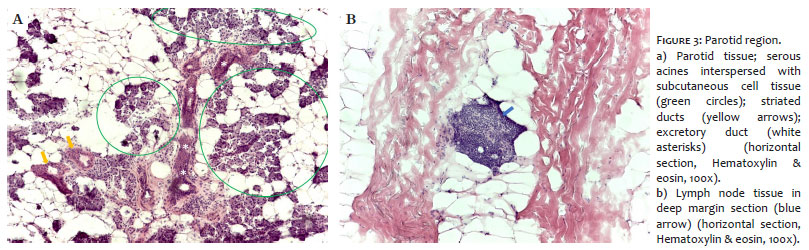
The skin over the parotid region is also a frequent site of tumors treated by MMS. In the case of tumor involvement in the deep margins, parotid and lymph node tissues can be identified in the freezing sections.
The parotid is the largest salivary gland in the body. It is considered a compound, tubule-acinar, merocrine and exocrine gland. In adults, serous acini form it entirely (Figure 3a). The superficial portion of the gland is closely related to the superficial musculoaponeurotic system (SMAS) of the face, which is formed from an aponeurotic extension of the platysma muscle. Some terminal branches of the great auricular nerve are also located there.7
The region is also a place of high lymph nodes concentration; small lymph node fragments can simulate basaloid tumor nests (Figure 3b) or peritumoral inflammatory infiltrate. This occurs mainly if the freezing sections are thick, causing overlapping cells, a common situation in specimens with high adipose tissue content.
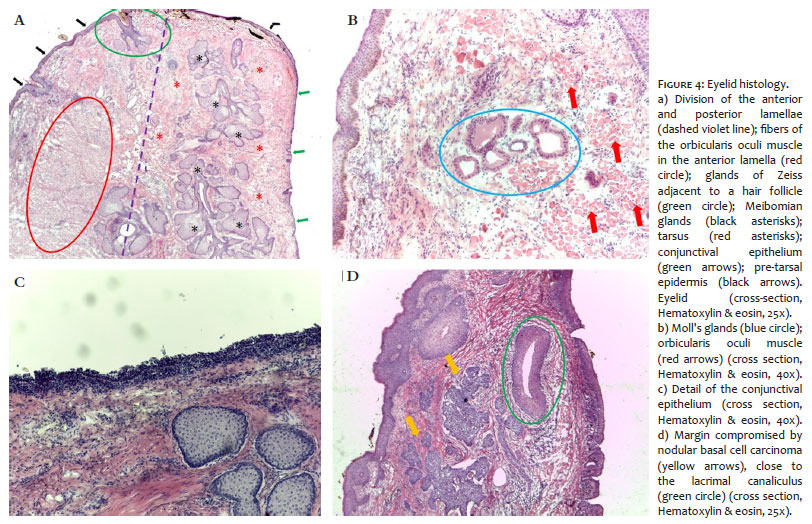
The eyelid is divided into anterior and posterior lamellae. The anterior lamella consists of skin (the thinnest of the body, 0.4 mm thick) and orbicularis muscle, while the tarsus and the conjunctiva form the posterior lamella (Figure 4a).8,9
The tarsus, a dense fibroelastic tissue, is responsible for providing structural support, which is essential to the eyelid's function. Inside, we find modified sebaceous glands, called Meibomian glands, which produce lipid secretion. Its content flows directly through eyelid openings to form the outer layer of the tear film. They are known as the most frequent site of sebaceous carcinoma.9
Zeiss's sebaceous glands present in the dermis, in turn, are associated with the hair follicles of the eyelashes on the eyelid edge. Also, in the dermis, there are Moll glands (apocrine sweat glands), which have openings for both hair follicles and directly on the anterior palpebral margin, being more numerous on the lower eyelid (Figure 4b).Unlike Moll's glands, the eccrine sweat glands are not confined to the eyelid margins and can be found throughout the eyelid region.9
The conjunctival epithelium is non-keratinized and has about five layers of cells in thickness (Figure 4c). Goblet cells, which produce mucus, can be found inside the epithelium, being more frequent in the fornix region.9
The upper and lower lacrimal canaliculi, often seen in MMS histological sections in tumors of the medial portion of the eyelids, are lined with stratified squamous epithelium (Figure 4d). In the region of common canaliculus, formed by the union of the two canaliculi, the epithelium becomes pseudo-stratified, non-ciliary, and columnar.10
The nasal surface is rich in glandular and follicular structures, and their density varies according to the subunit assessed (Figures 5a and 5d). Much of the nose's shape - especially the nasal wings, and thus the patency of the nasal vestibule - depends on cartilage support (Figure 5c). In full-thickness sections, the mucous lining with ciliated cylindrical pseudostratified epithelium can be identified as well as the nasal mucous glands (Figures 5d and 5e).
The differentiation between BCC and hair follicles is a constant in the routine of the micrographic surgeon. The multicentric growth of the basaloid epithelium adjacent to the hair follicle characterizes the folliculocentric basaloid proliferation (FBP). This benign histological finding can occur in this topography and can be confused with BCC (Figure 5f).
If not recognized, this entity can lead to unnecessary excision of additional stages by the Mohs surgeon. Criteria such as the folliculocentric and radial disposition, in addition to the presence of a prominent hyaline basal membrane and normal adjacent stroma in the FBP, help differentiate the two entities.11,12
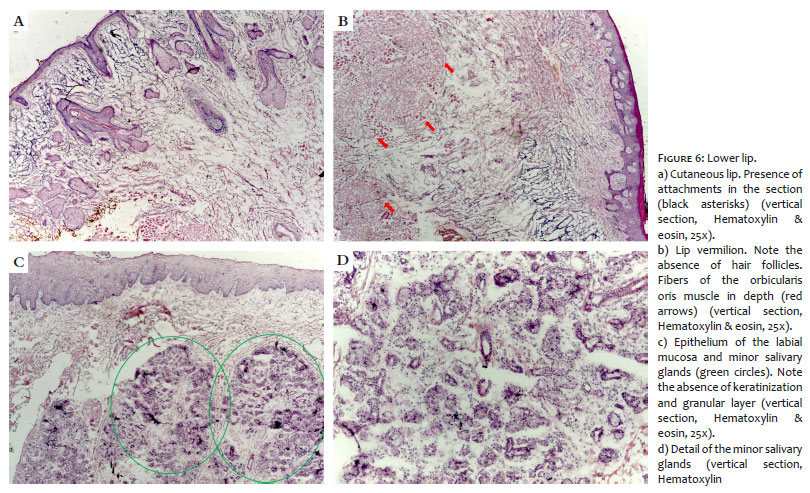
The lips consist of two movable musculomembranous folds, covered by mucosa, on the inner surface, and cutaneous integument, on the outside (Figure 6a). The area of the mucocutaneous union constitutes the vermilion (Figure 6b). Stratified keratinized squamous epithelium covers the cutaneous portion and preserves the cutaneous attachments. On the other hand, the mucous portion is not keratinized, and its pink color, absence of protection structures, and the presence of salivary glands differentiate it from the skin (Figures 6c and 6d). Even now, ectopic sebaceous glands can be identified, and are called Fordyce granules.6
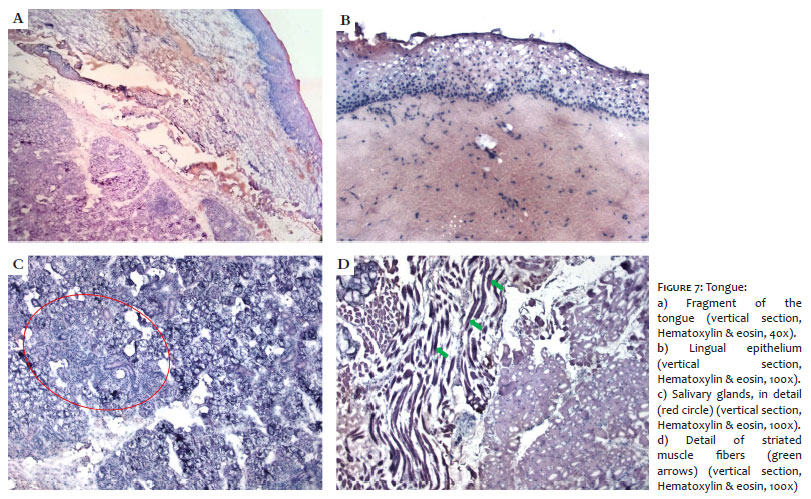
The tongue is predominantly composed of striated skeletal muscle fibers, in addition to adipose tissue, blood vessels, salivary glands, and mucous lining (Figure 7).
The mucosa that covers the back of the tongue has keratinized epithelium and, due to the taste buds' presence, makes the tongue a sensory and specialized structure. The lingual papillae (filiform, fungiform, and goblet) cover the anterior two-thirds of the tongue's back, and a smooth mucosa, rich in lymphoid aggregates (lingual tonsillar tissue), covers the tongue's base.6,13
In a longitudinal section of the nail apparatus, the proximal nail fold, nail plate, matrix, bed, and hyponychium are seen.14 When addressing tumors located in the distal phalanx, it is possible to identify one or more of these structures on the surgical margins.
The proximal nail fold has dorsal epithelium (with sweat glands and no pilosebaceous units) and ventral epithelium (without cutaneous attachments, cornified, and which will originate the cuticle). The matrix is composed of a thick germinal epithelium without a granular layer, with few melanocytes. As the matrix cells progress to the upper layers, their cytoplasm becomes more eosinophilic and the nucleus, pycnotic, until it forms the nail plate, consisting of cornified cells of lamellar arrangement (Figure 8).
Below the lamina is the nail bed, delimited distally by the hyponychium and proximally by the matrix. Its epithelium is thin, without granules, and attached to the underlying dermis by long and narrow epidermal cones. The hyponychium and the volar skin have a granular and thick and compact corneal layer. The dermis rests directly on the distal phalanx, without the interposition of subcutaneous tissue.15
Eventually, when dealing with cutaneous lesions in breast topography, it is possible to identify mammary gland tissue in the specimen's deep margins. The secretory portion of the mammary gland includes lobules and ducts, interspersed by the interlobular stroma (dense connective tissue, fat cells, and blood vessels) (Figure 9).
The lobes are circular structures made of acids (formed by an inner layer of epithelial cells and an outer layer of myoepithelial cells) and loose connective tissue - the intralobular stroma. In this, the presence of chronic inflammatory cells, mainly lymphocytes, is physiological and variable according to the menstrual cycle period.
A layer of epithelial cells and another layer of myoepithelial cells form the mammary ducts, and they drain the lobules.6
Depending on the section's incidence, such structures may form basophilic clusters that must be differentiated from tumor infiltration at the subcutaneous level.
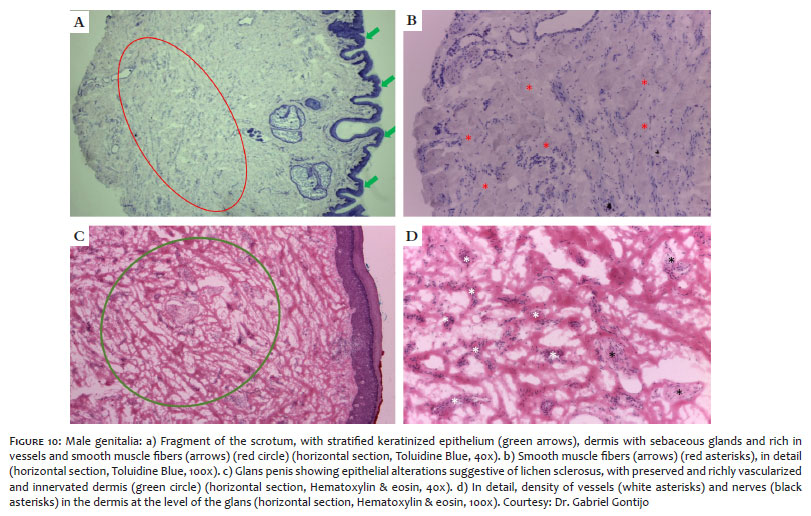
A thin epidermis, a dermis rich in sebaceous glands and blood vessels, forms the penis and scrotum's skin envelope. This dermis is closely related to the tunica darts, composed of smooth muscle fibers (Figure 10). At the glans level, there is a transition from keratinized epithelium to the mucous epithelium.5,13
Histological differentiation between benign and malignant entities is essential in CMM, aiming at precise removal of the tumor and preservation of healthy tissue. Dense inflammation, scar tissue, hair follicles, and other normal skin structures can resemble tumor aggregates. Knowing the histological particularities of the body's different areas through freezing sections contributes to the correct interpretation of the slides.
Raíssa Rigo Garbin | 0000-0002-9771-1209
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Gerson Dellatorre | 0000-0002-9657-0002
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Roberto Gomes Tarlé | 0000-0003-2831-6579
Approval of the final version of the manuscript; study design and planning; critical revision of the manuscript.
Guilherme Augusto Gadens | 0000-0002-8990-1715
Approval of the final version of the manuscript; study design and planning; critical revision of the manuscript.
Alexandre Luiz Weber | 0000-0002-4862-5777
Approval of the final version of the manuscript; study design and planning; critical revision of the manuscript.
Lismary de Forville Mesquita | 0000-0002-7148-4490
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical revision of the manuscript.
1. Gross K, Steinman HK. Mohs surgery and histopathology. New York: Cambridge University Press; 2009.
2. Aasi SZ, Leffell DJ, Lazova RZ. Atlas of practical Mohs histopathology. New York: Springer; 2013. p. 3-9.
3. Elder DE. Lever's histopathology of the skin. Philadelphia: Lippincott Williams & Wilkins; 2008.
4. Morgan BM, Hamill JR, Spencer JM, Thornhill R. Atlas of Mohs and frozen section cutaneous pathology. 2nd ed. New York: Springer; 2018. p. 17-43.
5. Junqueira LC, Carneiro J. Histologia Básica. 10th ed. Rio de Janeiro: Guanabara Koogan; 2004.
6. Gartner LP, Hiatt JL. Tratado de histologia em cores. 2nd ed. Rio de Janeiro: Guanabara Koogan; 2003.
7. Carlson E, Ord R. Textbook and color atlas of salivary gland pathology: diagnosis and management. New Jersey: Wiley-Blackwell; 2008.
8. McCord CD, Codner MA. Eyelid and periorbital surgery. St. Louis: Quality Medical Pub; 2008. p. 784.
9. Kanski JJ. Clinical ophthalmology: a systematic approach. 6th ed. New York: Butterworth-Heinemann/Elsevier; 2007. p. 931.
10. Guthoff RF, Katowitz JA. Oculoplastics and Orbit: Aesthetic and Functional Oculofacial Plastic Problem-Solving in the 21st Century: Springer; 2009.
11. Leshin B, White WL. Folliculocentric basaloid proliferation. The bulge (der Wulst) revisited. Arch Dermatol. 1990;126(7):900-6.
12. Patel NS, Johnston RB, Messina JL, Cherpelis BS. A unique basaloid proliferation encountered during Mohs surgery: potential pitfall for overdiagnosis of basal cell carcinoma. Dermatol Surg. 2011;37(8):1180-8.
13. Netter FH. Atlas de anatomia humana. 4th ed. Rio de Janeiro: Elsevier; 2008. p. 51-62.
14. Belda Junior N, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 2nd ed. São Paulo: Atheneu; 2014. p. 47-82.
15. Magalhães GM, Succi ICB, Sousa MAJ. Subsídios para o estudo histopatológico das lesões ungueais. An Bras Dermatol. 2003;78(1):49-61.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}