


Erlian Dimas Anggraini; Anis Irawan Anwar
Received on: 19/12/2019
Approved on: 17/02/2020
Financial support: None
Conflict of interests: None
Study conducted at the Dermatology and Venereology Department, Faculty of Medicine Hasanuddin University, Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia
Pincer nail deformity is characterized by excessive transverse over curvature of the nail. A 58-year-old woman came with a complaint of pincer nail accompanied by swelling and pain in the last 1 month due to frequent use of narrow shoes. We performed a surgical intervention indicated to treat pain, inflammation, interference with wearing shoes, and cosmetic embarrassment using an inverted T incision method with osteophyte removal. This case showed that the surgical approach did not require a long time to be conducted, presenting brief healing time, minimal pain, and excellent cosmetic outcome.
Keywords: Osteophyte; Ambulatory surgical procedures; Nails, malformed
Pincer nail deformity is a nail disorder of the hands and feet characterized by an excessive transverse over the curvature of the nail, which is caused by osteophyte formation in the distal phalanx.1 Cornelius and Shelley first described pincer nail deformity in 1968 as a transverse distal over the curvature of the nail.2 Based on its etiology, there are four distinct types of pincer nail: hereditary pincer nails, posttraumatic pincer nails, pincer nails in arthropathic disorders, and pincer nail affecting a single nail.3 Foot alterations because of narrow shoes or osteoarthritis are reported to cause pincer nails.4 A pincer nail compresses the nail bed leading to pain during walking or exercising as well as cosmetic problems.5 Pain may arise due to the embedding of the pincer nail in the lateral nail folds and nail bed, which becomes more pronounced distally.6 Several conservative and surgical treatment methods have been suggested to correct pincer nail deformities.7 However, there is still no established standard method for treating pincer nail deformity currently.7
Pincer nail is rarely found and reported in our region. Also, when a diagnosis is established, patients are often reluctant to undergo surgical correction. Here, we report the first case of pincer nail deformity surgical correction with osteophyte removal in our center.
A 58-year-old woman presented to the Outpatient Department of Dermatology Hasanuddin University Hospital, Makassar, South Sulawesi, Indonesia, with a complaint of pincer-shaped right toenail accompanied by swelling and pain since one month before admission. Initially, the patient reported she had noticed the nail deformity since two years ago; however, at that time, there were no complaints, so the patient did not seek treatment.
There was a history of trauma to the right toenail due to the frequent use of narrow shoes. The patient had diabetes and routinely consumed metformin twice a day in the last five years. Also, the patient had a history of uncontrolled hypertension. The patient denied having a history of similar complaints before or in her family.
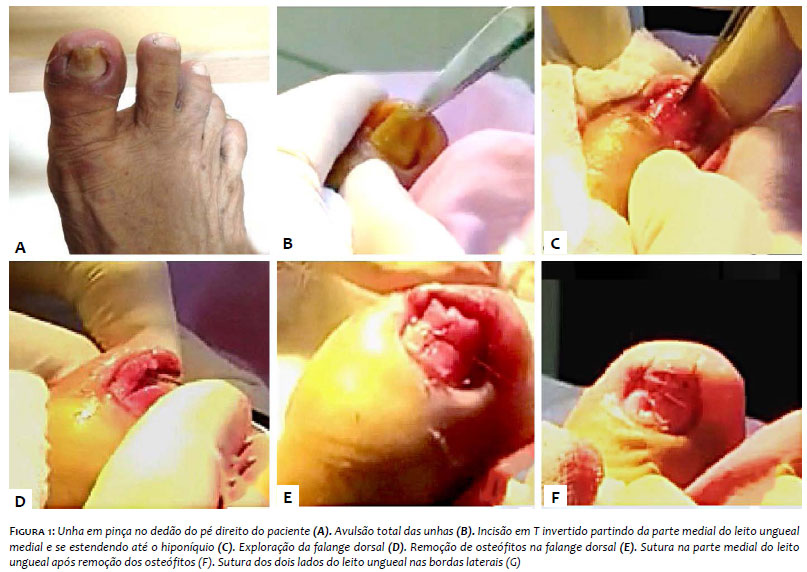
The patient was otherwise in good general condition. Dermatological examination showed nails clamping towards the medial and edema on the first finger of the right foot (Figure 1A). Considering the history and physical examination, we decided to perform corrective surgery using the inverted T incision method.
The surgery was conducted under local digital block anesthesia using 1% lidocaine after disinfection with povidone-iodine. A digital tourniquet application was applied to prevent bleeding during the procedure. The first step was to perform a total nail avulsion by using iris scissors and nail splitters to separate the nails from the nail bed (Figure 1B). Precaution was taken not to injure the nail bed. In the second step, an inverted T incision, starting from the medial nail bed extending to the hyponychium down to the bone, was made using a sharp knife (blade #11) to explore the distal phalanx and expose the osteophyte (Figure 1C). In the third step, after the nail bed was cut along the previously determined incision line, osteophytes were found on the surface of the distal phalanx (Figure 1D) and were subsequently removed (Figure 1E). In the fourth step, the nail bed was sutured, and the medial nail bed (which was widened by the incision) was sutured using polyglactin 4-0 (Figure 1F). Both sides of the nail bed were sutured separately to the lateral borders (Figure 1G). This suture was maintained for three weeks to keep the nail bed stretched over the bone. A significant improvement on the nails was observed after 6 months.
The over curvature of the nails is commonly called pincer nails, tubed nails, or trumpet nails.8 The risk of pincer nails is higher in the big toenails compared to the fingernails, and its incidence rate is two times higher in women than in men.4 Pincer nail deformity should be diagnosed and treated because it affects not only the appearance but also the function of the digit and the quality of life due to the pain it causes.9 Cosmetic results of pincer nail surgery have become more critical because of the increasing demand for nail preservation and excellent aesthetic outcome.10 Surgical methods include nail avulsion, total or partial excision of the nail bed, phenol matrixectomy of the lateral matrix horns, destruction of the matrices by electrocauterization, removal of osteophytes, skin or mucosal grafting of the nail bed, zigzag nail bed flap method, and others.11
As excessive osteophyte and narrow nail bed are the underlying factors of the pincer nail, removal of osteophyte and widening of the nail bed are expected to provide an ideal anatomic structure for the healthy growth of the future toenail.3 Inverted T incision is the method of choice that can be used in high-risk groups, including elderly patients over 70 years old and those with diabetes mellitus, chronic kidney disease, and/or peripheral vascular disease because this method is less invasive than the zigzag nail bed flap method.2
Correction of pincer nail deformity using the inverted T incision approach is a simple and effective procedure because of shorter operating time, reduced pain during surgery, excellent functional and aesthetic outcome.
Erlian Dimas Anggraini | ORCID 0000-0002-1889-6752
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Anis Irawan Anwar | ORCID 0000-0002-1830-5617
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript..
1. Altun S, Gürger M, Arpaci E, İnözü E. Correction of pincer nail deformity with dermal flap: a new technique in pincer nail deformity surgery. Acta Orthop Traumatol Turc. 2016;50(3):362-5.
2. Jung DJ, Kim JH, Lee HY, Kim DC, Lee SI, Kim TY. Anatomical characteristics and surgical treatments of pincer nail deformity. Arch Plast Surg. 2015;42(2):207-13.
3. Markeeva E, Hinterberger L, Vogt T, Rass K. Combined surgical treatment of a pincer nail with chemical matricectomy, median nail incision, and splinting. J Dtsch Dermatol Ges. 2015;13(3):256-9.
4. Noh SH, Na GH, Kim EJ, Park K. Significance of Surgery to Correct Anatomical Alterations in Pincer Nails. Ann Dermatol. 2019;31(1):59-65.
5. Shin WJ, Chang BK, Shim JW, Park JS, Kwon HJ, Kim GL. Nail plate and bed reconstruction for pincer nail deformity. Clin Orthop Surg. 2018;10(3):385-8.
6. de Berker DA, Richert B, Baran R. Acquired disorders of the nails and nail unit. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook's Textbook of Dermatology. New Jersey: Wiley-Blackwell; 2016. p.1-76.
7. Cho YJ, Lee JH, Shin DJ, Sim WY. Correction of pincer nail deformities using a modified double Z-plasty. Dermatol Surg. 2015;41(6):736-40.
8. Haneke E. Nail Disorders. In: Kang S, Amagai M, bruckner AL, enk AH, Margolis DJ, McMichael AJ, et al, editors. Fitpatricks Dermatology in General Medicine. New York: Mc Graw Hill Education; 2019. p. 1568.
9. Muslim MYBA, Chuah CK. Correction Of Pincer-Nail Deformity Using Autologous Full Thickness Skin Graft: A Case Report. Malaysia Jour Dermatology. 2017;39:79-81.
10. Aksoy B, Aksoy HM. Novel surgical method for pincer nail treatment: Partial matricectomy and triple flap technique. Dermatol Surg. 2017;43(11):1397-1399.
11. Chang P, Argueta G. Pincer nail. Our Dermatology Online. 2016;7(2):234-237.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}