


Francine Papaiordanou1; Guillermo Loda2; Marcela Benez2; Leonardo Pereira Quintella3
Received on: 03/07/2018
Approved on: 10/03/2020
Financial support: None
Conflict of interests: None
Study conducted at the Dermatology Institute Prof. Rubem David Azulay, Santa Casa da Misericórdia do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
Angiokeratomas are vascular malformations constituted by telangiectasia of preexisting vessels. They are not classified as angiomas. It is the rarest variant of angiokeratomas, with few cases in the literature. The mechanism of development of these lesions has not yet been fully elucidated. Small lesions can be treated with electrosurgery, curettage, or cryosurgery. Larger lesions require deep surgical excision, and depending on the size and depht of the lesion, direct closure, flap, or grafting. CO2 or argon laser are considered other treatment options. In this case report we describe a classic case of circumscribed angiokeratoma, with onset at birth, and progressive growth.
Keywords: Ambulatory surgical procedures; Dermatology; Vascular malformations
Angiokeratomas are relatively rare vascular malformations characterized by asymptomatic skin lesions. They are telangiectasias of pre-existing vessels and are not considered angiomas.1 The capillaries in the papillary dermis dilate, with secondary epidermal changes, with hyperkeratosis and acanthosis.2 Angiokeratoma circumscriptum is the rarest variant of angiokeratomas.3
Clinically, angiokeratomas appear as multiple hyperkeratotic dark red to black, papule, and plaques. Sometimes they are friable, with minimal trauma bleeding. They vary in size, depth, and location.4 Most commonly, they occur in the lower limbs, in segmental distribution.
In most cases, the lesion is already noticed at birth, but it rarely develops late in childhood or adolescence. There are no reports of spontaneous regression.4
Other clinical forms of angiokeratomas include 1. Angiokeratoma corporis diffusum (Fabry's angiokeratoma); 2. Mibelli's angiokeratoma (occurs on the back of the phalanges of hands and feet de); 3. Angiokeratoma of Fordyce's (scrotal region); 4. Solitary papular angiokeratoma (the most common form).1-5 There is also the circumscribed neviform angiokeratoma, which is an even rarer variant of the angiokeratoma circumscriptum.
The exact mechanism of development of these lesions has not yet been fully elucidated.5
A 25-year-old man reported lesions on the left lower limb since birth. Initially, they were dark red lesions, with little elevations, segmental, on the lateral aspect of the left leg. Over the years, the injury changed, becoming hyperkeratotic, elevated, and bleeding (Figure 1). The patient sought our Service due to the friability and pain in the elevated lesions, which bothered him when putting on his shoes and performing physical activities. He presented no known comorbidities.
On physical examination, the patient presented raised hyperkeratotic plaques, with a rough/warty and friable surface, painful to minimal trauma and pressure from clothes and shoes. The most elevated plaques varied in size, between 1cm and 4cm in their longest axis.
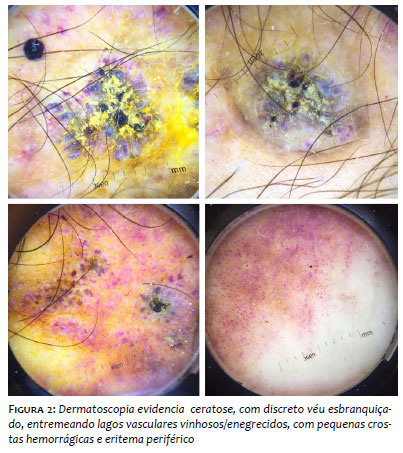
Around the most elevated lesions, there were small keratotic dark red plaques, with segmental distribution, extending from the lower third of the left leg to the instep and ipsilateral hallux. There was no difference in circumference between the two legs. Dermoscopy was necessary for the diagnostic elucidation, showing a lesion with an important keratotic component and a discreet whitish veil, interspersing dark red/ black venous lakes, with small hemorrhagic crusts and peripheral erythema (Figure 2).
The patient reported having performed a partial excision of the lesion ten years ago, but there was local recurrence.
Due to the history of recurrence, we opted for deep surgical excision (even muscular fascia), in two stages. Initially, the most extensive lesion was excised, with an angled allowing the primary closure, which resulted in a Y scar, and closure with moderate tension due to little skin mobility at the site (Figure 3).
We started performing central pulley sutures, for a better approximation of the edges, and then we used simple internal and external sutures, with nylon 3.0.
Primary closure allows faster recovery and less postoperative morbidity. Whenever possible, it should always be the first surgical option.
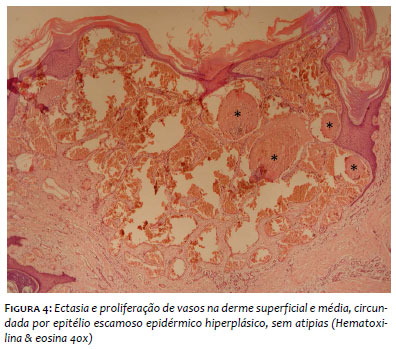
Histopathology showed ectasia and proliferation of vessels in the superficial and mid-dermis, surrounded by hyperplastic epidermal squamous epithelium, without atypias (Figure 4).
Corroborating clinical, dermoscopic and histopathological data, we concluded that it was angiokeratoma circumscriptum, the rarest variant among angiokeratomas.
The patient presented good healing of the surgical wound and returned for excision of the other minor lesions, near the major lesion.
Angiokeratomas are vascular lesions defined as one or more dilated vessels of the papillary dermis, accompanied by acanthosis/hyperkeratosis of the epidermis.4 The worldwide prevalence is 0.16%, affecting slightly more men.4 Angiokeratoma circumscriptum is considered the rarest variant. It most frequently affects the lower limbs, unilaterally, or asymmetrically distributed between the two members, 4 but it can also occur on the thighs, buttocks or other parts of the body.6 They are papular and/or nodular lesions that, over time, coalesce and become verrucous, hyperkeratotic plaques, in zosteriform distribution.1,3,4
In most cases, they are already present at birth, but they can develop in childhood or adolescence and even during adulthood.5,6
Our patient presented the classic picture of angiokeratoma circumscriptum: men, lower limb lesion present since birth, with progressive growth until adulthood, becoming symptomatic. The pathophysiological mechanism of the formation of these lesions is still unknown.4,5,6,7 Initially, there is vascular ectasia of the papillary dermis, and epidermal changes occur secondarily.
Some authors suggest that the development of hyperkeratosis may be associated with the expression of metalloproteinase-9 (mmp9) in the lesion.4,6 Changes in local hemodynamics, such as trauma to the capillaries in the papillary dermis, can cause the appearance of telangiectasias in the papillary dermis with hyperkeratosis and acanthosis in the epidermis. There are also reports of the expression of VEGF and its receptors (VEGFR-1 and 2) in the dilated capillary endothelial cells of these lesions. VEGF is an angiogenic growth factor. Of its receptors, VEGFR-1 is involved in cell migration and vascular maintenance; VEGFR-2 acts primarily in the regulation of mitosis and cell proliferation, but its exact role has not yet been precisely elucidated.6
Some authors consider, in addition to trauma, pregnancy, subcutaneous hematomas, and tissue hypoxia as other possible triggering factors.5
Angiokeratoma circumscriptums may coexist in association with Klippel-Trenaunay syndrome (port-wine stain, venous and lymphatic malformation, and soft tissue hypertrophy).4,5,7,8 It may also be associated with Cobb syndrome, nevus flammeus, cavernous hemangioma, and traumatic arteriovenous fistula.
Our patient presented no known risk factors or association with other types of lesions.
The diagnosis is primarily clinical and confirmed by histopathology, which shows hyperkeratosis, papillomatosis, and acanthosis, with the proliferation of vessels limited to the papillary dermis.7,8,9 The histopathological differential diagnosis is made with verrucous hemangioma, which consists of congenital and localized vascular malformation, but involving the reticular and subcutaneous dermis. Angiokeratoma circumscriptum consists of vascular dilation without vessel proliferation. On the other hand, verrucous hemangioma is considered a hyperplastic tumor, with mesenchymal cell proliferation tending to form capillaries.
Dermoscopy assists in the diagnosis, showing reddish lacunae and a whitish veil, covered by whitish scales and/or hematic crusts. However, dermoscopy does not allow todifferentiate a verrucous hemangioma from a circumscribed hemangioma due to the difficulty in estimating the depth of the lesion.
It is important to remember that, clinically, it can mimic a malignant melanoma.7,10 Cutaneous tuberculosis, deep mycoses, viral warts, and other lesions that show a linear growth pattern should also be considered as clinical differential diagnoses.7
Corroborating clinical, dermoscopic, and histopathological data, we closed the diagnosis of angiokeratoma circumscriptum, the rarest variant among angiokeratomas.
Angiokeratoma does not regress spontaneously. Small injuries can be treated with electrocautery, curettage, or cryosurgery. More extensive lesions require deep surgical excision and, depending on the size of the defect, direct closure, flap, or graft. Other options include CO2 or argon laser.4,5,7,10
The rarity of this entity in the world literature motivated the report of this case.
Our patient presented the classic clinical, dermoscopic, and histopathological features of the angiokeratoma circumscriptum.
We thank Dr. Patricia Bichara for her assistance with the patient's surgery.
Francine Papaiordanou | ORCID 0000-0003-0138-8361
Preparation and writing of the manuscript.
Guillermo Loda | ORCID 0000-0003-0289-5656
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marcela Benez | ORCID 0000-0003-0289-5656
Approval of the final version of the manuscript.
Leonardo Pereira Quintella | ORCID 0000-0002-2076-8776
Critical revision of the manuscript.
1. Jindal SR, Chalvade P, Jerajani HR. Late onset palmar angiokeratoma circumscriptum: An unusual presentation. Indian Dermatol Online J. 2014;5(3):320-2.
2. Bouaddi M, Colonna C, Cavalli R, Gelmetti CM. [A new location of angiokeratoma circumscriptum]. Ann Dermatol Venereol. 2012;139(11):732-5.
3. Ivy H, Julian CA. Angiokeratoma Circumscriptum.[Internet]. Bethesda MD: U.S. National Library of Medicine [cited 2020 Dec 5]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549769/
4. Sadana D, Sharma YK, Dash K, Chaudhari ND, Dharwadkar AA, Dogra BB. Angiokeratoma circumspriptum in a young male. Indian J Dermatol. 2014;59(1):85-7.
5. Das A, Mondal AK, Saha A, Chowdhury SN, Gharami RC. Angiokeratoma circumscriptum neviforme: An entity, few and far between. Indian Dermatol Online J. 2014;5(4):472-4.
6. Kang YH, Byun JH, Park BW. Angiokeratoma circumscriptum of the buccal mucosa: a case report and literature review. J Korean Assoc Oral Maxillofac Surg. 2014;40(5):240-5.
7. Agrawal SN, Deshmukh YR, Jane SD. Angiokeratoma circumscriptum: dilemma in diagnosis. Indian J Pathol Microbiol. 2014;57(2):350-1.
8. Wankhade V, Singh R, Sadhwani V, Kodate P, Disawal A. Angiokeratoma circumscriptum naeviforme with soft tissue hypertrophy and deep venous malformation: A variant of Klippel-Trenaunay syndrome? Indian Dermatol Online J. 2014;5(Suppl 2):S109-12.
9. Kwon NH, Kim SY, Kim GM. A case of post-injury angiokeratoma circumscriptum of the chest. Ann Dermatol. 2010;22(1):66-8.
10. Debbarman P, Roy S, Kumar P. Angiokeratoma circumscriptum neviforme. Indian Pediatr. 2012;49(1):80.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}