


Bárbara Ávila Chagas da Silva1; Meire Soares Ataide1; Leticia Reis de Oliveira Mamere1; Gabriel Fernandes Dias2
Data de recebimento: 13/09/2019
Data de aprovação: 28/01/2020
Suporte Financeiro: Associação de Apoio à Residência Médica de Minas Gerais
Conflito de interesse: Nenhum
Trabalho realizado na Universidade Federal do Triângulo Mineiro, Uberaba (MG), Brasil
INTRODUCTION: Unaesthetic scars can trigger symptomatic, functional, aesthetic and emotional repercussions. Among the main treatments found today is microneedling.
OBJECTIVE: Prospective, quantitative study to evaluate the benefits of healing with a single microneedling session.
METHODS: A microneedling session was performed on scars of 28 patients. Before performing the procedure with cylinders containing 192 2.5 mm needles and 90 days later, scars are photographed in a standardized manner, having been applied on the Patient and Observer Scar Assessment Scale. Through the performed score, a quantitative evaluation by the analysis of the parameters, being vascularization, pigmentation, thickness, relief, malleability, surface area, pain, itching, color, stiffness, height and irregularity, in addition to the patient's total score and general opinion. and the observer.
RESULTS: All variables obtained improvement, except pain, emphasizing malleability and height. In addition, the overall opinion of the patient and the observer shows 51% improvement.
CONCLUSIONS: Microneedling is a safe, inexpensive, minimally invasive treatment that delivers experimental results in a single session.
Keywords: Cicatrix; Scales; Therapeutics
Healing is a dynamic process that requires biochemical and physiological synchrony to have adequate tissue restoration. This mechanism depends on several factors, such as anatomical location, skin type, underlying diseases, age, ethnicity, and the surgical technique used. When the healing involves the dermis completely or extends to the subcutaneous tissue, the lesion becomes noticeable.1,2
The most common unsightly scars are hypertrophic, keloid, and atrophic. They can trigger symptomatic, functional, aesthetic, and emotional repercussions. Thus, this condition can cause psychological damage and limit the patient in social and professional relationships. Therefore, the treatment of these lesions is a constant challenge for the physician.3-5 The patient's eagerness for improvement may be related to the desire to erase unpleasant memories, surprise the partner, or even request a promotion in their work.6
The repercussions associated with the emotional condition secondary to the scar include anxiety, social exclusion, depression, interruption of daily activities, sleep disorders, in addition to psychosocial deterioration, with difficulty in reintegrating into the environment in which they lived.7,8
Several techniques have been tested to correct post-traumatic skin sequelae. However, many of them are unsatisfactory. Needling methods, such as the subcision, described in 1995, have also been used for the treatment of scars.9 Currently, one of the proposed treatments is microneedling.
The technique has been improved and increasingly widespread since it is a minimally invasive, simple, inexpensive, safe, and effective procedure. The procedure consists of inducing a controlled lesion on the skin without causing any real damage to the epidermis. The objective is to originate micropunctures that reach the dermis and trigger, with the bleeding, an inflammatory stimulus. Thus, microneedling induces the release of growth factors, which stimulate the formation of new collagen and elastin in the papillary dermis, associating with the production of new capillaries. Then, the association of neovascularization and neocollagenesis after the treatment leads to scar reduction.10-12 The indications for this procedure are diverse and can be used in rejuvenation as an active vehicle - for example, retinol and vitamin C - or as an isolated stimulus. It also acts on sagging and attenuation of wrinkles. Finally, as already mentioned, it corrects distensible, wavy, and retractable depressed scars, in addition to recent and old stretch marks.13
One of the standardized instruments is the disposable cylinder equipped with stainless steel microneedles with length varying from 0.5mm to 3mm and diameter from 0.1mm to 0.25mm. It is essential to highlight the value of the diversity of needle lengths since the intensity of the reaction generated is proportional to this measure. For example, 1.5mm needles promote microchannels that reach the epidermis and dermis, destroying the scar collagen bundles.14,15 Among the benefits of this procedure, we highlight its good safety profile, which can be applied to all phototypes, including Fitzpatrick skin types IV andV, since it rarely leads to hyperpigmentation. Usually, patients present good tolerability and may have mild erythema and ede
ma, with a quick return to work activities, varying from seven to 10 days, according to some studies. In some cases, there is no need for work leave. Also, it has other advantages, such as collagen stimulation without removing the epidermis; shorter healing time; lower risk of adverse events when compared to ablative techniques; increased skin resistance and thickness; and the possibility of being conducted in sites where there is less concentration of skin annexes.16,17
When indicating the procedure, the physicians should pay attention to the contraindications, such as the presence of active acne, oral herpes or any other local infection, psychological disorders that may be exacerbated by the treatment, moderate to severe chronic skin disease (for example, psoriasis), blood dyscrasias, tendency to keloid, use of anticoagulants, treatment with chemotherapy or radiotherapy, and patients who can’t understand the technique. Adverse events are not common; however, they can occur. The most frequent are erythema and irritation, which usually disappear within a few hours. There are also reports of post-inflammatory hyperpigmentation, worsening of acne, reactivation of herpes, granulomatous allergic reactions, and local infections when using nonsterile materials.18,19 In general, most reports state significant improvement, some after just one session. Patients are satisfied with both aesthetic and mobility improvements. Also, they report good tolerability to the procedure, with no complications in most cases. Thus, the effectiveness and safety of this therapy are confirmed.17,20
To evaluate the clinical improvement after the treatment is a challenge since there is no single standardized scale for scar assessment. Some of the most used ones are the Vancouver Scale (VSS), Manchester Scar Scale (MSS), Patient and Observer Scar Rating Scale (POSAS), Visual Analogue Scale (VAS), and Stony Brook Scar Evaluation Scale (SBSES), based on subjective parameters, but used objectively. Among these, POSAS stands out, as it considers the assessment of both the physician and the patient, elucidating the characteristic of the lesion reliably.21,22
The present study aimed to quantify the clinical improvement of surgical scars, including post-traumatic scars and breast prosthesis, cesarean section, or skin biopsy, after a micro-needling session, assessing the results using POSAS.
This study was conducted at the Dermatology Outpatient Clinic of the Universidade Federal do Triângulo Mineiro (UFTM), after the approval by the institution's Research Ethics Committee.
Thirty patients were randomly selected, who had a link to the Outpatient Clinic of the Hospital de Clínicas da UFTM with unsightly and/or dysfunctional scars resulting from aesthetic procedures, such as breast prosthesis, car accident trauma, stab wounds, cesarean section, cholecystectomy, or skin biopsy. Exclusion criteria were: less than 18 years old; cognitive deficit; presence of any active lesion at the procedure site; moderate to severe chronic skin diseases, such as eczema or psoriasis; blood dyscrasias; tendency to keloid; use of anticoagulants; treatment with chemotherapy or radiation therapy.
After selection, the patient was instructed on the risks and benefits of the procedure. Then, the scar was photographed, and the Patient and Observer Scar Assessment Scale (POSAS) was applied. The procedure was performed in an exclusive operating room of the Dermatology Service of the UFTM Specialty Outpatient Clinic, having been performed by resident dermatologists assisted by the dermatologist responsible for the Service. After antisepsis with chlorhexidine 2%, anesthesia was performed with lidocaine solution 2% without vasoconstrictor, diluted 1:4 with 0.9% saline solution, and injected into the skin with a 31G needle. The intervention was followed using of a cylinder studded with stainless steel microneedles, totaling 192 units with 2.5 mm length (Dr. Roller®, Moohan Enterprise CO., Gyeonggido, South Korea), with back and forth movements guided by a uniform pattern of petechiae throughout the treated area, reaching a deep injury. According to some studies, 10 to 15 passes must be made in the same direction, and at least four crossing passes in the rolling areas. At the end of the procedure, a gauze dressing was applied over the lesion, and the patient was instructed to remove it after 24 hours with running water, and initiate then the use of a dexpanthenol-based skin regenerator for 10 days. Also, the importance of photoprotection was stressed. All patients received the same treatment protocol and guidelines. After 90 days of the procedure, the questionnaire was applied again, and the lesion was photographed. It is worth mentioning that the data and photos taken in the first evaluation were not made available to the observer and the patient.
The variables analyzed at POSAS by the observer were: vascularization, pigmentation, thickness, texture, malleability, surface area, and general opinion; and those of the patient were pain, itching, color, stiffness, height, irregularity, and general opinion. The score ranged from 1 to 10, with the minimum value being normal skin and 10 the worst scar imaginable. For assessment of the results, the Wilcoxon test 23 was applied to compare day 0 to day 90.
Thirty patients were selected and, since the sample proportion is unknown, the sample was calculated from a 90% confidence level and a maximum error of the estimate of 15%.24-25 However, two were lost to follow-up. All those who completed the study reported bearable pain during the procedure. Also, the return to work activities ranged from three to five days, according to the extent of the injury. Of the 28 patients assessed, four had no desire to repeat the procedure, due to complete improvement, and the others wished to perform it again. There were no complications, such as hypertrophic scarring or infections. The patients' skin phototypes varied from II to IV, according to the Fitzpatrick scale.
The comparative analysis between D0 and D90 of the vascularization, pigmentation, thickness, texture, malleability, surface area, pain, itching, color, stiffness, height, irregularity, general opinion of the patient and the observer was performed using the Wilcoxon test.23 Table 1 shows the results.
After the experiment and the hypothesis test, it is noted that the vast majority of parameters are changed when comparing the skin on the day of application and after 90 days of use (p-level <0.05). All parameters of the observer rejected the null hypothesis, that is, vascularization, pigmentation, thickness, tex-ture, malleability, and surface area, presenting differences when comparing the start and the end date. When assessing the patient's scale, the pain parameter does not reject the null hypothe-sis, that is, it did not change from one period to the next, while itching, color, stiffness, height, and irregularity varied.
We calculated the averages of each of the parameters for comparison. Except for pain, which had no difference between the averages in the two periods, we observed that the other parameters showed a reduction in the average scores. This represents an improvement, since the lower the value for the scale, the closer it is to the characteristics of normal skin. Tables 2 and 3 show the results. Malleability and height were the parameters that obtained the highest average reductions in percentages between the scores in the two periods, while vascularization and stiffness obtained the smallest reductions for the observer and patient scale, respectively. Even so, those with the smallest changes showed considerable average reductions (a minimum of 40%).
Considering the frequencies of the patient's scale parameters, the pain parameter was the only one that showed a different behavior from the rest. When analyzing the other parameters of the patient's scale, we can observe a similar behavior to that of the observer's score since they concentrated on the lower levels of the scale after 90 days.
Furthermore, to the assessment of the parameters, the general opinions of both the observer and the patient were studied. The hypothesis tests rejected the null hypothesis (p<0.05), indicating a change in the opinion of those involved from one period to the next. The changes in the general views of the observer and the patient were positive since the average grades of these parameters were reduced by 51%, representing greater proximity to normal skin after 90 days.
In terms of frequency distribution, we can visualize the opinion change of those involved in the study. The frequencies of the general views of the observer and the patient were analyzed. We can observe that, in both distributions, the concentration shifted from the right to the left side of the graph, showing the change in the grades from one period to the next. The patient's opinion, for example, had a higher incidence (39%) in grade 10 in the initial period. On day 90, the highest incidence (32%) was for grade 1.
This study selected 30 patients; however, two were lost to follow-up. Among the 28 subjects who completed the treatment, four patients revealed that they would not like to undergo the procedure again, as they were already satisfied with the result. However, the others wanted new sessions, despite the initial satisfactory result. According to a study conducted in 2017, despite the different results, all patients showed satisfaction and interest in following the treatment after microneedling.26
All patients reported good tolerability to the procedure, as expected by the authors. Also, there were no reports of adverse events or complications, proving to be a safe and minimally invasive technique. As already described, as the epidermis is maintained, microneedling has a low risk of infection and post-inflammatory hyperpigmentation. Another advantage of this treatment is the short recovery time. In the present study, patients returned to work activities in two to four days.27-29
Through the application of POSAS, we could quantitatively assess the following variables, according to the observer: vascularization, pigmentation, thickness, texture, malleability, surface area, and general opinion. The patient's variables were: pain, itching, color, stiffness, height, irregularity, and general opinion. The score ranged from 1 to 10, with the minimum value being normal skin and 10 the worst scar imaginable. The pain criterion did not vary between the first and the second questionnaire; however, all patients scored 1 in this regard, that is, equal to normal skin from the beginning.
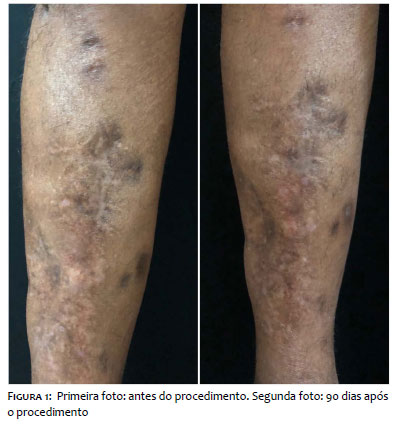
Among the evaluated criteria, except for pain, we noticed an improvement in all aspects, highlighting malleability and height (Figures 1 and 2). Published studies show that microneedling promotes the degradation of dense collagen in the misaligned fibers of the healing process, allowing the realignment of collagen fibers and promoting the minimization of irregularities, reduction of scar volume, increased sensitivity, and elastin synthesis. Consequently, there is an improvement in the scar distensibility, reducing hyperpigmentation and normalizing the keratinocyte-melanocyte relationship.29
In the present study, one of the patients had a scar on the face with mobility difficulties, requiring physiotherapy. After the procedure, the physical therapist noticed an improvement in the condition during the movements. Microneedling can improve flexibility and elasticity, as shown by other studies.30-32
In 2018, a study used POSAS to assess the improvement of scars after microneedling, and the results pointed to an increase in scar quality with a significant tendency to normal skin. The general opinion showed a 51% improvement for both the patient and the observer, corresponding to the values found in this study.33 Microneedling stimulates the synthesis of significant structural and skin reconstruction elements (collagen, elastin, proteoglycan), being used in the treatment of many skin defects, with high effectiveness in cases of scarring.34 Therefore, it was chosen as the only form of therapy in this study.
One of the objectives of this study was to assess clinical improvement with just one session. However, partial improvement implies the need to prolong treatment. A study conducted in 2014 on rats to investigate the effects of repetitive treatments showed the best results when the treatment was repeated four times with an interval of three weeks. Therefore, with the largest number of sessions, better results can be obtained.31 It is noteworthy that the patient's opinion, the prospects for improvement and the true degree of dissatisfaction are essential for conducting any procedure or deciding to prolong the therapy.6
Microneedling is a safe, low-cost, effective, and minimally invasive treatment. With just one session, satisfactory results can be obtained, but others may be necessary. The method includes the improvement of several relevant aspects in the analysis of scars, such as malleability and height. In addition to the aesthetic improvement, the functional enhancement of the affected site should be highlighted. Therefore, considering the good tolerability and the high degree of patient and observer satisfaction, this procedure is an excellent therapeutic option for scarring.
Therefore, knowing its technique and indications is essential for training young dermatologists.
I thank Sergio Antonio Zullo, master in Statistics from the Universidade Estadual de Campinas, and Vinícius Chagas Martins, master in Production Engineering from the Universidade Federal de Itajubá, for the assistance in the analysis of statistical data.
Bárbara Ávila Chagas da Silva | ORCID 0000-0002-6333-8311
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Meire Soares Ataide | ORCID 0000-0002-2102-3637
Active participation in research orientation.
Leticia Reis de Oliveira Mamere | ORCID 0000-0001-6114-7602
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Gabriel Fernandes Dias | ORCID 0000-0003-4295-9378
Data collection, analysis, and interpretation.
1. Oliveira Júnior FC, Florêncio PR, Fernandes RL . Como obter melhor cicatrização nas incisões das cirurgias estéticas corporais. RBM Dermatologia e Cosmiatria. 2009. v. 66, p. 27-31.
2. Mandelbaum SH, Di Santis EP, Mandelbaum MHS. Cicatrização: conceitos atuais e recursos auxiliares - Parte I. An. Bras. Dermatol. 2003;78(4):393-408.
3. Pereira JRC. Tratamento de cicatrizes patológicas com a associação de cepalin, heparina e alantoína. Rev Bras Med. 2003;78(8):603-608.
4. Crocco EI, Costa NM. Tratamento de cicatriz atrófica em paciente asiático com laser fracionado não ablativo Er: Glass 1550nm. Surg Cosmet Dermatol. 2012;4(4):354-356.
5. Kadunc BV, Almeida ART. Surgical treatment of facial acne scars based on morphologic classification: a Brazilian experience. Dermatol. Surg. 2003;28(12):1200-9.
6. Robinson JK, Hanke WC, Siegel DM, Fratila A. Surgery of the Skin. Philadelphia: Elsevier; 2010.
7. Pellard S. Epidemiology, aetiology and management of abnormal scarring: a review of the literature. J Wound Care. 2006;15(1):44-8.
8. Gangemi EN, Gregori D, Berchialla P, Zingarelli E, Cairo M, Bollero D, et al. Epidemiology and risk factors for pathologic scarring after burn wounds. Arch Facial Plast Surg. 2008;10(2):93-102.
9. Orentreich DS; Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543-9.
10. Singh A , Yaday S. Microneedling: Advances and widening horizons. Indian Dermatol Online J. 2016;7(4): 244-254.
11. Doddaballapur, S . Microneedling with Dermaroller . J Cutan Aesthet Surg. 2009;2(2):110-111.
12. Lima EVA, Lima MA , Takano D . Microneedling experimental study and classification of the resulting injury. Surg Cosmet Dermatol. 2013;5(2):1104.
13. Konicke K, Knabel M, Olasz E. Microneedling in Dermatology: a review. Plast Surg Nurs. 2017;37(3):112-115.
14. Bahuguna A. Micro needling-Facts and Fictions. Asian J Med Sci. 2013;4:1-4.8.
15. Anastassakis K. The Dermaroller Series. [Last accessed on 2018 Jun 22].http://www.mtoimportadora.com.br/site_novo/wp.content/uploads/2014/04/Dr.- Anastassakis-Kostas.pdf
16. Bonati LM, Epstein GK, Strugar TL. Microneedlingin All Skin Types: a review. J Drugs Dermatol. 2017;16(4):308-313. Review.
17. Lima EVA. Indução percutânea de colágeno com agulhas em cicatrizes após acidentes automobilísticos: correção cosmética e funcional . Surgical Cosmetic Dermatol. 2017;9(2):127-9.
18. Iriarte C, Awosika O, Rengifo-pardo M, Ehrlich A. Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol. 2017;10:289-298.
19. Nair PA, Arora TH. Microneedling using dermaroller: A means of collagen induction therapy. GMJ. 2014;69:24-7
20. Alster TS, Graham PM . Microneedling: A Review and Practical Guide. Dermatol Surg. 2018 Mar;44(3):397-404.
21. Fearmonti R, Bond J, Erdmann D, Levinson H. A review of scar scales and scar measuring devices. Eplasty. 2010;10:e43.
22. Linhares BC, Viaro MSS, Collares MVM. Traduçao para o português da Patient and Observer Scar Assessment Scale (POSAS) Rev Bras Cir Plast. 2016;31(1):95-100.
23. Siegel SE, Castellan JR, NJ. Estatística não paramétrica para ciências do comportamento. 2 ed. Porto Alegre: Artmed; 2006. p. 448.
24. Levin J. Estatística Aplicada a Ciências Humanas. 2 ed. Sao Paulo: Editora Harbra Ltda; 1987.
25. Triola MF. Introdução à Estatística. 7 ed. Rio de Janeiro: LTC; 1999.
26. Pinheiro LHZ, Chaves FNG, Veloso ST, Kastanópoulos HM, Soares AN, Dorigo IL, et al. Ambulatório de cicatrizes inestéticas: relato de experiência. Raízes e Rumos. 2017;5(1):85-92.
27. Hogan S, Velez MW, Ibrahim O. Microneedling: a new approach for treating textural abnormalities and scar. Semin Cutan Med Surg. 2017;36(4):155-163.
28. Alster TS, Graham PM. Microneedling: a Review and Practical Guide. Dermatol Surg. 2018;44(3):397-404.
29. Santos AN, Ferro GM, Negrão MMC. Microneedling approach in burn scars: literature review. Rev Bras Queimaduras. 2016;15(2):116-21.
30. 30. Aust MC, Knobloch K, Reimers K, Redeker J, Ipaktchi R, Altintas MA, et al. Percutaneous collagen induction therapy: an alternative treatment for burn scars. Burns. 2010;39:836-43.
31. Zeitter S, Sikora Z, Jahn S, Stahl F, Strauß S, Lazaridis A, et al. Microneedling: matching the results of medical needling and repetitive treatments to maximize potential for skin regeneration. Burns. 2014 Aug;40(5):966-73.
32. kubiak R , Lange B. Percutaneous collagen induction as an additive treatment for scar formation following thermal injuries: preliminary experience in 47 children. Burns. 2017;43(5):1097-1102.
33. Busch KH, Aliu A, Walezko N, Aust M. et al. Medical Needling: effect on skin erythema of hypertrophic burn scars. Cureus. 2018;10(9):e3260.
34. Zduńska K, Kołodziejczak A, Rotsztejn H. Is skin microneedling a good alternative method of various skin defects removal. Dermatol Ther. 2018;31(6):e12714.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}