


Suthida Tantipunpipat1; Sinee Weschawalit2; Panlop Chakkavittumrong2
Received on: 31/10/2019
Approved on: 10/03/2020
Financial support: None
Conflict of interests: None
Study conducted at the Divisão de Dermatologia, Colégio Internacional de Medicina Chulabhorn, Thammasat University, Pathum Thani, Tailândia.
INTRODUCTION: The inflammation may play a critical role in the development of facial acne. Pro-inflammatory mediators, such as prostaglandins and leukotriene, have been implicated in the initiation of acne.
OBJECTIVE: This study aimed to evaluate the clinical efficacy and safety of 1% diclofenac gel compare with a placebo gel in the treatment of mild to moderate acne patients in 12 weeks. Methods: A 12 weeks, randomizing, double-blind, individual and split-face comparative trial was conducted in 24 volunteers. Patients with mild to moderate acne vulgaris, aged 18 to 30 years were enrolled. They received 2.5% benzoyl peroxide with 1% diclofenac gel and 2.5% benzoyl peroxide with placebo gel apply regularly at each side of the face.
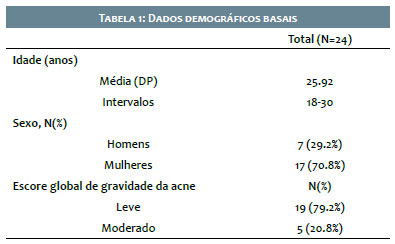
RESULTS: 24 participants with mean (SD) age of 25.92 years were enrolled in the study. Statistically significant decrease in mean of comedone lesions was observed in 1% diclofenac gel group by acne lesion count at week 12 (P <0.05) superior than placebo gel. Moreover, post inflammatory hyperpigmentation also had statistically significant decrease superior to placebo group at week 4.
CONCLUSIONS: The 1% diclofenac gel topical treatment has shown good clinical efficacy and safety in decreasing facial comedones at week 12 and post-inflammatory hyperpigmentation in 4 weeks.
Keywords: Acne vulgaris; Diclofenac; Inflammation; Hyperpigmentation
Acne vulgaris is a common chronic skin disorder of the pilosebaceous unit that is usually involved with adolescents.1 Acne vulgaris has several main factors including inflammation which is emerging recently because of the antibiotic overuse and resistant of bacteria.2 The course of acne may be self-limited, but it is a distress condition among young adult who is sensitive about their appearance and also may lead to permanent scarring.3,4
Inflammatory signaling in the pilosebaceous unit is a component of the initiation of acne lesions. The microcomedone, which arises from keratinocyte occlusion, is believed that inflammation may precede microcomedone formations and trigger follicular plugs. The study of acneprone patients and early acne lesions shows increasing in perifollicular and papillary dermal CD3+, CD4+ T cells, the proinflammatory cytokine IL- 1, and many proinflammatory signals in the uninvolved skin.5 P.acnes induces inflammation by stimulating via TLRs, and it activates the up-regulation of TLR2 and TLR4. TLR2 of macrophages are induced to release multiple proinflammatory cytokines and chemokines: interleukin- 8 ( IL- 8) , tumor necrosis factor- alpha ( TNFα) , interleukin- 1 alpha ( IL- 1α), interleukin- 12 ( IL-12), interleukin-1 beta ( IL-1β).6,7 Then, the pathogen will be attacked by PMNs or NKs cell and/ or antimicrobial peptides ( AMPs).8
Moreover, inflammation is induced via the cyclooxyge-nase metabolic pathway and the lipoxygenase pathway.9 The key mediator of inflammation in COX pathway is prostaglandins; it significantly aggravates inflammation and also stimulate sebaceous proliferation and sebum production via PPAR- mediated pathways.10,11 LTB4, LOX pathway, activates the local attraction of neutrophils and monocytes.11 Moreover, LTB4 stimulates DNA synthesis and keratinocyte proliferation which is the early acne lesion.12 Diclofenac, NSAID, is proven to have analgesic, anti-inflammatory, and antipyretic properties and show dual action on COX and LOX inhibitors.13,14 Inhibiting LOX and COX pathway may be another way to treat acne disorder.
Acne lesions prone to resolve with sequelae. Production and release of various keratinocyte-derived mediators, including prostaglandins, leukotrienes and many cytokines that affect melanocyte proliferation and melanin production are promoted by inflammation of the epidermis.15 Although PIH usually spontaneous resolves, but it can last from months to years.16 Since the hyperpigmentation is a consequence of the inflammation, it is important to control the inflammation effectively for preventing and reduce the severity of PIH.16
In this study, the authors aimed to evaluate the clinical efficacy and safety of facial acne vulgaris reduction, post inflammatory hyperpigmentation and quality of life with acne in male and female aged 18-30 years old using anti-inflammation effect of 1% diclofenac gel. The reduction of acne lesion counts and acne severity is the primary endpoint.
This study was designed as a single center, randomizing, double-blind, individual and split-face comparative trial. This study was conducted at the outpatient dermatology clinic of Benchakitti Park Hospital between October 2018 to April 2019. This study was approved by the Human Ethics Committee of Thammasat University
Seventeen women and seven men with a mean age of 25.92 years were enrolled (N=25). Eligible subjects had Fitzpatrick skin types II-V with mild to moderate facial acne vulgaris. The acne vulgaris is evaluated by acne lesion counts and global acne severity index. Subjects were asked to avoid any other moisturizer or cosmetic product that have acne reduction effect during the study.13 The exclusion criteria are subjects with severe acne disease, severe systemic disease, known allergy to NSAIDs, history of hirsutism, polycystic ovarian disease or significant menstrual irregularities, pregnancy and lactating. Subjects are using systemic antibiotics, topical corticosteroids, oral contraceptive pill, and systemic retinoid will be excluded. One patient not complete the trial due to personal issue that cannot come to follow up (N=1).
In this study, the treatment will be assigned to each patient randomly according to the intervention group. The inter-vention group will get 1% diclofenac gel to apply on one side of the face twice a day with 2.5% benzoyl peroxide applied to both sides of the face daily before bed. Along with prescribing broad spectrum anti-UVA and anti-UVB sunscreens to apply adequately every day. Other topical applications or cosmetic products that will affect the result will be prohibited throughout the study
The primary clinical efficacy endpoint is the change from baseline in facial acne vulgaris at week 12 by acne lesion count and global acne severity score. The secondary endpoint are drug local-tolerability and reduction of post inflammatory hyperpigmentation by Antera 3D® image (Miravex Ltd, Dublin 2, Ireland). Focus area of Antera 3D® image (Miravex Ltd, Dublin 2, Ireland) will be taken on the same point by using the intersection line between the imaginary line from lateral cantus to alar of nose. The photograph will be taken at the baseline and every visits by using digital camera (CANON60D) in the identical camera setting, lighting and fixed patient positioning. Moreover, the subjects were asked to answer dermatology life quality index and Cardiff acne disability index to evaluate mental impact of acne disorder.
The demographic data were analyzed using standard descriptive statistics. The change from baseline in facial acne vulgaris, post inflammatory hyperpigmentation and life quality index were presented as mean (95% confidence interval). P-value corresponds to Paired t test with < 0. 05 was considered statistically significant.
Among twenty-four participants with mild to moderate facial acne vulgaris were enrolled into the study. Baseline demo-graphic data was shown in (Table 1).
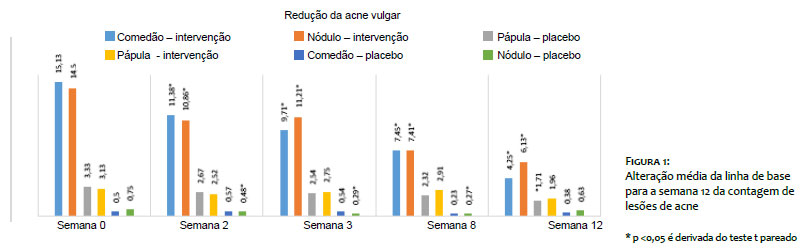
At baseline, the mean number of acne counts were not significantly different between treatment groups. Both groups have acne severity and acne count not significantly different. Among patients treated with 2.5% benzoyl peroxide/1% diclofenac gel, the mean (SD) baseline comedone lesion count was 15.13, decreasing to 4.25 after 12 weeks while the mean baseline comedone lesion count of 14.5 for placebo-treated patients decreased to 6.13. The number of comedone acne is reduced significantly in both group in week 2, week 4, week 8, and week 12. There is no different of comedone treatment efficacy between the intervention group and placebo group except in week 12 that the intervention group shows significantly superior than placebo group (P<0.001). (Figure 1)
Secondly, the mean (SD) baseline papule and pustule lesion count was 3.33, decreasing to 1.71 after 12 weeks while the mean baseline papule and pustule lesion count of 3.13 for placebo-treated patients decreased to 1.96. The reduction of papule and pustule acne is constantly improving in both groups. The intervention group has significantly reduced number of papule and pustule at week 12, but it does not show superior significant between the intervention group and placebo group.
Third, the mean (SD) baseline cystic and nodular acne lesion count was 0.5, decreasing to 0.38 after 12 weeks while the mean baseline cystic and nodular acne lesion count of 0.75 for placebo-treated patients decreased to 0.63. The reduction of cystic and nodular acne is constantly improving in both groups. The placebo group has significantly reduced number of cystic and nodular acne at week 2, week 4 and week 8, but it does not show superior significant between the intervention group and placebo group.
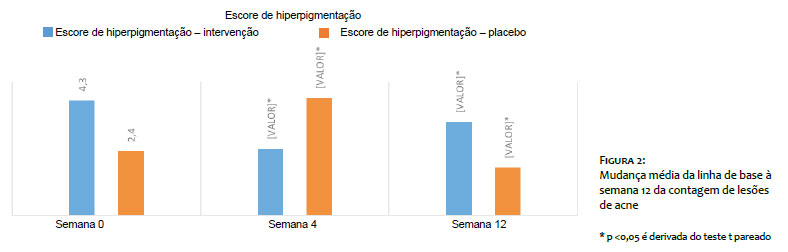
The Antera 3D assessments for melanin shows impro-vement of melanin color after 12 weeks in both intervention and placebo group. Among 2.5% benzoyl peroxide/1% diclo-fenac gel-treated patients, the mean (SD) baseline PIH lesion was 0.4, reduce to 0.36 after 12 weeks while the mean baseline PIH lesion of 2.5% benzoyl peroxide/ placebo gel group was 0.42 reduce to 0.38. There is no different at the baseline of both groups. At week 4, the 2.5% benzoyl peroxide/1% diclofenac gel group show the superior reduction of hyperpigmentation score superior over 2.5% benzoyl peroxide/ placebo gel group significantly. At the end of the study, the hyperpigmentation score does not show statistically significant difference between both groups. (Figure 2)
The side effect was scored by patient and physician using side effect questionnaire. Both physicianand patient evaluation about severity of scaling, erythema, burning, stinging, and it-ching scoring are quite similar. The side effect remained low for both groups, and severity scores range in 0 or 1 for 80 to 90 percent of patients at the end of study. The most common side effect is mild erythema and scaling. This mild side effect did not lead to discontinuation of treatment. The improvement score
The improvement score was recorded by patients and physician. For the patients perspective on intervention side, the mean (SD) baseline ofacne improvement is 1-25% improvement. After 12-week treatment, the mean (SD) of acne improvement is 26-50% improvement. For placebo side, the mean (SD) baseline of acne improvement is 1-25% improvement and 1-25% improvement at week 12. Both the intervention group and placebo group have significant improvement of acne at week 12, but it does not show superior significant between the intervention group and placebo group.
For doctor perspective on intervention side, the mean (SD) baseline of acne improvement is no improvement. After 12-week treatment, the mean (SD) of acne improvement is 1-25% improvement. For placebo side, the mean (SD) baseline of acne improvement is no improvement. After 12 weeks’ treatment the mean (SD) of acne improvement is 1-25% improvement. Both the intervention group and placebo group have significantly improvement of acne at week 8 and week 12, but it does not show superior significant between intervention group and placebo group. In addition, the overall treatment satisfaction is 7.63 out of 10 at 12 weeks.
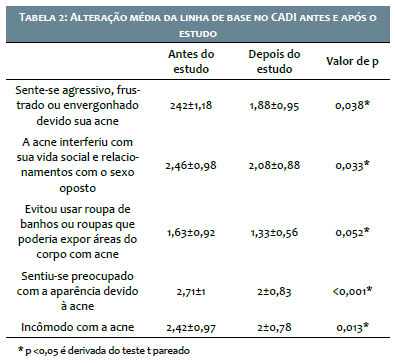
For acne induced quality of life impairment by CADI score, CADI 1-5 is mild impairment, CADI 6-10 is moderate impairment, CADI 11-15 is a severe impairment. At week 0, there was mild impairment (CADI = 1-5) for feeling aggressive, frustrated, or embarrassed on acne. There was significantly reduce in impairment of embarrassment, interfere with social life and relationship, the concern of appearance and acne disturbing. There was mild impairment of wearing swimming costumes. There was mild impairment of concerning the appearance. Patients acne severity considers mild impairment (CADI = 1-5). (Table 2)
To evaluate impact of acne on daily life is measure by DLQI, 0-1 = No effect on patients life, 2-5 = mild effect, 6-10 = moderate effect, 11-20 = very large effect, 21-30 = extremely large effect. The result shows only mild effect of acne to the patients quality of life.
Acne vulgaris is one of the most common skin disorder which commonly located on the face, chest, and back. It is predominantly among adolescents, at 15-18 years old.17 The goal of treatment is finding the cause of acne, reduce acne severity, prevent new acne formation, lessen psychological distress and scarring.18 Some of the acne patients find it is a stressful disorder that can lead to depression and lack of self-esteem.3 The DLQI study of 110 acne patients in Thailand, the mean total DLQI score was 8.95 (range 0-24). The most disturbing from acne is an embarrassment. This study only shows mild impairment. Similarly, the most disturbing is an embarrassment or self-consciousness. In addition, this study also evaluated CADI. The patients reported mild impairment from acne. After the treatment, the patients report lessen anxiety, lessen effect on their daily life, lessen interfering social life and lessen concern of appearance significantly.
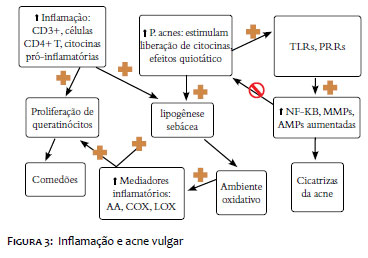
Inflammation has been recognized as one of the major factor initiated acne. The study of acneprone patients and early acne lesions shows increasing in perifollicular and papillary dermal CD3+, CD4+ T cells, the pro-inflammatory cytokine IL-1, and many proinflammatory signals in the uninvolved skin.5 The innate immune, when pathogen, Pacnes, slip through epidermis will be quickly recognized by TLRs and then attacked by cells (PMNs or NKs) and/or secreted substances like antimicrobial peptides (AMPs).9 TLR-2 and TLR-4 are responsible for acne pathogene-sis.6 Up-regulated AMP induces pro-inflammatory chemokines and cytokines and also stimulates keratinocyte production.5 Pacnes enhances sebaceous lipogenesis, which oxidized and induce production of inflammatory mediators in cultured keratinocytes.5 Other proinflammatory lipid by-products, AA, is metabolized into prostaglandins (PG), and leukotrienes (LT).8 LTB4 attract local neutrophils and monocytes.11 PGE2 stimulates the formation of histamine and bradykinin.19 This suggested that COX and LOX pathway induced inflammation in acne which opened new opportunities for acne treatment. (Figure 3)
The diclofenac, NSAIDs, is an anti-inflammatory drug that appears to have both effect on lipoxygenase pathway and cyclooxygenase pathway.20 The former study demonstrated that mice without LTB4 receptor have lower inflammation.20 The study of banoxaprofen show improvement of acne disorder.21 A study of tetracycline hydrochloride capsules with ibuprofen tablets (2,400 mg/day) for 2 months demonstrated an effective result. Another study combine minocycline capsules (150 mg/ day) and ibuprofen tablets (1,200 mg/day) also demonstrate very good result.22 Rofecoxib 50 mg daily prophylaxis premenstrual acne. 101 patients show significant decrease in inflammatory acne by zileuton.23 Explained this study that 1%diclofenac gel, COX and LOX pathway inhibitor, might help subside a small inflammation which there is an improvement of comedone statistically superior than placebo group. However, papule/pustule and cystic/nodule acne show promising result yet not statistically superior than placebo group. In addition, the results also show decreasing number of acne in both intervention and placebo group. This may due to 2.5% BPO, which is standard treatment of acne. A greater different in acne count may show if the study has larger group of patients.
The most common side effect in this study is mild scaling and erythema. Both intervention and placebogroup have no statistically different. These side effects are caused by both BPO and 1%diclofenac gel. The incidence of adverse events was 84.0% in the 2.5% BPO group of 450 Japanese volunteer in 52 weeks.24 Diclofenac treatment was well tolerated, patients reported ‘fair’ to ‘excellent’ tolerability. Some of patients experienced usually mild local reactions, for example, skin dryness, erythema, and pruritus.25 The higher the concentration of diclofenac leads to more side effect.26 In conclusion, 1% diclofenac gel to the limitations are that this is merely a small study with small sample size. The long-term follow up and larger number of patients are suggested to confirm the efficacy and safety.
Treat mild to moderate acne is safe with low adverse event.
The former study shows inflammatory factor has influence over melanocyte proliferation.27 Moreover, PGE2, and PGD2, is responsible for activation and /or proliferation of epidermal pigment cells.28 COX-2 knock-down in melanocytes resulted in decreased expression of tyrosinase, tyrosinaserelated protein 1(TRP-1) and melanogenesis Associated Transcription Factor (MITF), as well as reduced tyrosinase enzyme activity.29 This study shows significant improvement of hyperpigmentation score of intervention group superior to placebo group significantly at week 4. However, at the end of the study, the hyperpigmentation score does not show statistically significant difference between both groups. This might suggest that 1%diclofenac gel help reduce melanin faster than placebo gel.
Furthermore, despite inflammation factor, there are several factor that have impact to acne disorder.2 To achieve the goal of facial acne vulgaris treatment need several modality of treatment. 1%diclofenac gel is suggested to be one of the alter-native treatment of mild to moderate facial acne vulgaris. Better understanding of inflammation process would help create new possibility of acne treatment in the future
This randomized, split face, double-blind study demonstrated that 2.5% benzoyl peroxide/1% diclofenac gel is an effective and safe treatment option for patients with comedone. There was a statistically significant decrease in comedone lesions, and the medication causes little to no irritation. This study also suggests 2.5% benzoyl peroxide/1% diclofenac gel helps reduce post inflammatory hyperpigmentation after 4 weeks. Although the study of papule/pustule and nodule/cystic acne were not statistically significant. However, the result show little improvement to all lesions. The data consistently favoured 2.5% benzoyl peroxide/1% diclofenac gel over placebo to treat acne vulgaris and post inflammatory hyperpigmentation.
This study is the first to my knowledge to demonstrate the clinical efficacy and safety of primary and secondary out-comes of the change from baseline of acne vulgaris and PIH in 18-30 years’ women and men that have mild to moderate facial acne vulgaris by the assessment of acne lesion count, GAGs and Antera 3D® image. This study can be a valuable study that help research about inflammation and acne vulgaris in the future. However.
Suthida Tantipunpipat | ORCID 0000-0002-0130-7691
Coleta, análise e interpretação de dados; participação ativa na orientação de pesquisa; revisão crítica do manuscrito; preparação e redação do manuscrito; análise estatística.
Sinee Weschawalit | ORCID 0000-0003-1838-8464
Revisão crítica do manuscrito.
Panlop Chakkavittumrong | ORCID 0000-0003-4158-4789
Revisão crítica da literatura; coleta, análise e interpretação de dados; participação ativa na orientação de pesquisa; participação intelectual em conduta propedêutica e/ou terapêutica dos casos estudados; preparação e redação do manuscrito; análise estatística; concepção e planejamento do estudo.
1. Lynn DD, Umari T, Dunnick CA. Dellavalle RP. The epidemiology of acne vulgaris in late adolescence. Adolesc Health Med Ther. 2016;7:13-25.
2. Walsh TR, Efthimiou J, Dréno B. Systematic review of antibiotic resistance in acne: an increasing topical and oral threat. Lancet Infect Dis.16(3):e23-33.
3. Ritvo E, Del Rosso JQ, Stillman MA, La Riche C. Psychosocial judgements and perceptions of adolescents with acne vulgaris: A blinded, controlled comparison of adult and peer evaluations. Biopsychosoc Med. 2011;5(1):11.
4. Feldman S, Careccia RE, Barham KL, Hancox J. Diagnosis and Treatment of Acne. Am Fam Physician. 2004;69(9):2123-30.
5. Rico J. The Role of inflammation in acne vulgaris. Practical Dermatology. 2013:22-33.
6. Jugeau S, Tenaud I, Knol AC, Jarrousse V, Quereux G, Khammari A, et al. Induction of toll-like receptors by Propionibacterium acnes. Br J Dermatol. 2005;153(6):1105-13.
7. Tanghetti EA. The Role of Inflammation in the Pathology of Acne. J Clin Aesthet Dermatol. 2013;6(9):27-35.
8. Gollnick HP. From new findings in acne pathogenesis to new approaches in treatment. J Eur Acad Dermatol Venereol. 2015;29(Suppl 5):1-7.
9. Dreno B, Gollnick HP, Kang S, Thiboutot D, Bettoli V, Torres V, et al. Understanding innate immunity and inflammation in acne: implications for management. J Eur Acad Dermatol Venereol. 2015;29(Suppl 4):3-11.
10. Zouboulis CC, Jourdan E, Picardo M. Acne is an inflammatory disease and alterations of sebum composition initiate acne lesions. J Eur Acad Dermatol Venereol. 2014;28(5):527-32.
11. Tsai HH, Lee WR, Wang PH, Cheng KT, Chen YC, Shen SC. Propionibacterium acnes- induced iNOS and COX- 2 protein expression via ROSdependent NF- kappaB and AP- 1 activation in macrophages. J Dermatol Sci. 2013;69(2):122-31.
12. Alestas T, Ganceviciene R, Fimmel S, Müller-Decker K, Zouboulis CC. Enzymes involved in the biosynthesis of leukotriene B4 and prostaglandin E2 are active in sebaceous glands. J Mol Med (Berl). 2006;84(1):75-87.
13. Friedman ES, LaNatra N, Stiller MJ. NSAIDs in Dermatologic Therapy: Review and Preview. J Cutan Med Surg. 2002;6(5):449-59.
14. Aslan I, Özcan F, Karaarslan T, Kirac E, Aslan M. Decreased eicosapentaenoic acid levels in acne vulgaris reveals the presence of a proinflammatory state. Prostaglandins Other Lipid Mediat. 2017;128-129:1-7.
15. Morelli JG, Norris DA. Influence of Inflammatory Mediators and Cytokines on Human Melanocyte Function. J Invest Dermatol. 1993;100(2 Suppl):191S-195S.
16. Silpa-Archa N, Kohli I, Chaowattanapanit S, Lim HW, Hamzavi I. Postinflammatory hyperpigmentation: A comprehensive overview: Epidemiology, pathogenesis, clinical presentation, and noninvasive assessment technique. J Am Acad Dermatol. 2017;77(4):591-605.
17. Zouboulis CC, Piquero-Martin J. Update and future of systemic acne treatment. Dermatology. 2003;206(1):37-53.
18. Krakowski AC, Stendardo S, Eichenfield LF. Practical considerations in acne treatment and the clinical impact of topical combination therapy. Pediatr Dermatol. 2008;25(Suppl 1):1-14.
19. Tehrani R, Dharmalingam M. Management of premenstrual acne with Cox- 2 inhibitors: A placebo controlled study. Indian J Dermatol Venereol Leprol. 2004;70(6):345-8.
20. Fiorucci S, Meli R, Bucci M, Cirino G. Dual inhibitors of cyclooxygenase and 5- lipoxygenase. A new avenue in anti- inflammatory therapy? Biochem Pharmacol. 2001;62(11):433–8.
21. Allen B. Benoxaprofen and the skin. Br J Dermatol. 1983;109:361-4.
22. Kaminsky A. Less common methods to treat acne. Dermatology. 2003;206(1):68-73.
23. Zoubolis CC. Zileuton, a new efficient and safe systemic anti-acne drug. Dermatoendocrinology. 2009;1(3):188-92.
24. Kawashima M, Nagare T, Katsuramaki T. Open-label, randomized, multicenter, phase III study to evaluate the safety and efficacy of benzoyl peroxide gel in long-term
25. use in patients with acne vulgaris: A secondary publication. J Dermatol. 2017;44(6):635-643.
26. Taylor RS, Fotopoulos G, Maibach H. Safety profile of topical diclofenac: a meta- analysis of blinded, randomized, controlled trials in musculoskeletal conditions. Curr Med Res Opin. 2011;27(3):605-22.
27. Akarsu S, Aktan S, Atahan A, Koç P, Özkan S. Comparison of topical 3% diclofenac sodium gel and 5% imiquimod cream for the treatment of actinic keratoses. Clin Exp Dermatol. 2011;36(5):479-84.
28. Lévesque M, Feng Y, Jones RA, Martin P. Inflammation drives wound hyperpigmentation in zebrafish by recruiting pigment cells to sites of tissue damage. Dis Model Mech. 2013;6(2):508-15.
29. Nordlund JJ, Collins CE, Rheins LA. Prostaglandin E2 and D2 but Not MSH Stimulate the Proliferation of Pigment Cells in the Pinnal Epidermis of the DBA/ 2 Mouse. J Invest Dermatol.1986;86(4):433-7.
30. Kim JY, Shin JY, Kim MR, Hann SK, Oh SH. siRNA-mediated knock-down of COX- 2 in melanocytes suppresses melanogenesis. Exp Dermatol. 2012;21(6):420-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}