


Érico Pampado Di Santis1; Patrícia Holderbaum1; Natália Machado Mildner1; Larissa Ethel Soriano Freire2; Denise Steiner2
Date received: 10/12/2019
Date approved: 02/01/2020
Financial Support: None
Conflict of interest: None
Research performed at the Dermatology Service, Universidade de Mogi das Cruzes, Mogi das Cruzes, (SP) Brazil
It is noteworthy the range of facial treatments, with aesthetic purpose, with which we can preserve the balance of the shape or beauty of our patients. Fillers, botulinum toxin, laser, and other technologies are widely used in dermatology. Eyelids can also be treated with these and other therapeutic resources. However, herniation of the fat pockets of the upper eyelids does not present significant results with these methods. The advancement of techniques known as minimally invasive and other technologies does not satisfy the treatment of this facial aesthetic unit. Thinking about the global rejuvenation of the face, it is unlikely that we will achieve a result of excellence without acting on the eyelids. Upper blepharoplasty remains irreplaceable, and it is the treatment of choice for skin redundancy and herniation of fat pockets. This surgery, with a long history in Dermatology, has a unique and fundamental role in facial rejuvenation. In this study, we tried to demonstrate the surgical technique of superior blepharoplasty educationally and to prove its efficacy and safety, with good aesthetic and functional results. With full knowledge of this anatomical region and technical precepts, we recognize that we can perform it safely.
Keywords: Blepharoplasty; Surgery, plastic; Eyelids; Esthetics; Dermatologic surgical procedures; Rejuvenation
Cosmetic Dermatology has witnessed rapid progress in recent years with the use of minimally invasive procedures such as facial fillers, application of botulinum toxin, laser, and other technologies, Dermatology has achieved satisfactory levels of facial rejuvenation. Meanwhile, the upper eyelid is an aesthetic unit that has not enjoyed significant results, even when considering this technical progress and the possibility of using various technologies. A surgical approach is thus required. When addressing the aging process in the periorbital region, one should take into account the eyelids skin quality and the effect from herniation of the fat pads.1-4
There is currently no procedure or technology that efficiently corrects these periorbital alterations with results as good or better than upper blepharoplasty. This shows the need for the dermatologists command of the blepharoplasty surgical techni-que in order to solve problems and provide satisfactory overall facial rejuvenation.
Review the knowledge of the anatomy involved in upper blepharoplasty, describe the surgical technique didactically, and prove its efficacy and safety, with good aesthetic and functional results.
Reports of surgeries to remove skin from the upper eyelids date back more than two thousand years. In the 19th century, such removal was for cosmetic purposes. Mackenzie and Dupuytren were among the first to describe the technique. After nearly 100 years, Miller optimized the technique and described it again.5 Graef was the first to use the term blepharoplasty in 1818 for treatment of a skin cancer of the eyelid, as a procedure commonly performed by dermatologists and an example of cosmetic surgery originating from oncological surgery. French dermatologist Susanne Noll was one of the pioneers in cosmetic blepharoplasty and facelift surgery, contributing major advancements to cosmetic dermatological surgery.5
Castanares, Fournier, and González have recently contributed to the techniques advancement.5
The key to surgery of the eyelids and the periorbital area is indepth knowledge of this complex regions anatomy. The dermatologist must know the anatomy in detail, since the area to be corrected by surgery is as important as those that may be affected by unintended manipulation of various structures in this surgical field.
The eyelids are mobile folds covered externally by thin skin and internally by the lids tunica conjunctiva. The upper and lower eyelids are reinforced by dense bands of connective tissue, the upper and lower tarsi, which form the eyelids’ “skeleton”.6
The eyelids skin and a thin layer of subcutaneous tissue lie on the orbicularis oculi muscle. The palpebral portion of the orbicularis oculi is divided into two portions: pretarsal and preseptal.
The pretarsal portion is situated on the tarsal plate of the orbicularis oculi and is attached firmly to it. It begins at the lateral canthus and is inserted into the medial canthus. The superficial portion forms the anterior part of the medial canthus tendon, and the deep portion is inserted into the bone of the lacrimal crest, forming the posterior tendon of the medial canthus. When contracting, the eyelid closes by approaching the lacrimal point of the lacrimal sac.7-8
The preseptal portion attaches loosely to the skin. It covers the orbital septum of the upper and lower eyelids, and its fibers join laterally to form the lateral palpebral raphe. The preseptal portion inserts into the lacrimal fascia on the lateral portion of the lacrimal sac, and on contraction, it allows tears to enter the lacrimal sac. When the muscles relax, the lacrimal fascia returns to its normal position, and the tears flow directly into the nasolacrimal duct. 8-9
Located at the junction of these two portions is the su-pratarsal crease, which is important to identify in eyelid surgery.
The levator palpebrae superioris muscle, the four rectus muscles (superior, inferior, lateral, and medial), and the two obli-que muscles (superior and inferior) are the principal extraocular muscles.10
Immediately below the orbicularis oculi muscle is the orbital septum, a fibrous membrane of connective tissue that separates the orbital fat pads and deep orbital structures from the eyelid itself, and that performs containment of the orbital fat tissue and other orbital structures. The fat pad compartments lie behind the septum. With aging, both the septum and the orbicularis muscle and the skin become more saggy and thinner, leading the orbital fat to prolapse, making it more prominent and ptotic.8
These fat pads are surrounded by a thin fibrous fascia, individualizing them in compartments.
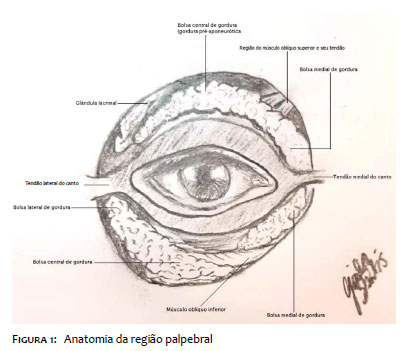
The upper eyelid has two compartments, central and nasal.11, 12 The central fat pad is situated anteriorly to the aponeurosis of the levator palpebrae, with a golden hue (Figure 1). The nasal fat pad is whitish-yellow in color and can be identified during blepharoplasty by exerting soft pressure on the eyeball and delicate divulsion of the nasal septum. Between the nasal and central fat pad lies a minimal but clear accumulation of adipose tissue that mimics separating the two pads and is associated loosely with the pre-aponeurotic pad; this structure is known as the adipose tissue transition. The trochlear and supraorbital branches of the superior ophthalmic vein are situated under it. Bleeding from this vein should be cauterized under direct visualization, because blind deep electrocauterization can injure the trochlea (or pulley of the superior oblique muscle) and cause diplopia.13-14
The lacrimal gland is arranged laterally. It can be confused with the fat pads, and care must be taken not to injure it inadvertently during surgery. The arterial supply to the eyelids and the venous drainage must also be observed and maintained intact during eyelid surgery.
The tarsi are structural elements of the eyelids consisting of dense fibrous tissue approximately 29mm wide and 10 to 12mm high at the midpoint, and 1mm thick. The inferior tarsus has the same width and thickness and is 5 to 6mm high. The tarsi begin medially at the lacrimal point and extend to the lateral commissures. Embedded vertically in the tarsal laminae and extending to their marginal aspects are the Meibomian sebaceous glands. There are 34 glands in the upper eyelids and 20 to 30 in the lower lids.12
Patient selection should involve the analysis of several factors, listed in Chart 1.
At least two consultations are necessary before the surgery. For dermatologists, in most cases several consultations and procedures have been performed prior to blepharoplasty. This prior interpersonal relationship with patients facilitates the preoperative preparation.
Preoperative preparation includes assessments of overall health status, history of medications, personal and family history of wound healing, and allergies, that is, a detailed patient work-up.
It is necessary to explain and furnish in writing the pre-, inter-, and postoperative care, probable recovery time, possibility of side effects such as dry eye, hematoma, and edema, among others, and possible surgical complications. In case of doubt as to the preexistence of dry eye, the Schirmer test should be performed. It should also be explained to the patient that a possible ptosis of tear glands will not be resolved by this surgery.
Prophylactic antibiotic therapy is performed with 2g of cephalexin 30 to 60 minutes before surgery. If the surgery is performed with local anesthesia, fasting is not necessary. The an-xiolytic lorazepam 1 to 2mg can be administered on the night prior to the procedure and after breakfast on the day of the surgery.
Photographic documentation is mandatory, as in all cosmetic procedures. The entire face should be documented, from the chin to the hairline, with the eyes open and closed, from the three angles (front, side, and oblique). Detailed photographs should also be taken of the orbital region, focusing on wrinkles, asymmetries, and scleral show.
The informed consent term, explaining possible complications of the surgery, should be signed to leave no doubts in the patient’s mind.
Preoperative tests include: complete blood count, TSH, free T4, blood glucose, liver enzymes, renal function, PT, and aP TT.
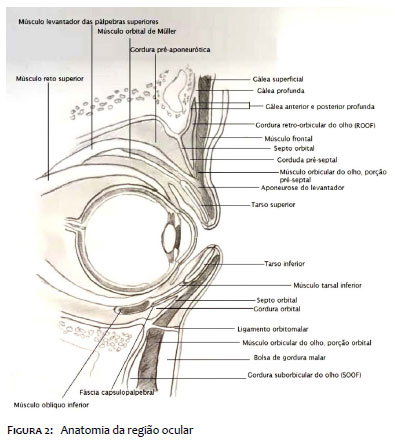
Anatomical nomenclature: (Figure 2)
- Skin: preseptal or supratarsal palpebral crease.
- Supratarsal crease.
- Orbicular muscle, preseptal portion is 3 or 4mm above the superior border of the tarsus.
- Fibrous orbital septum: courses from the orbital crease to the marginal arch (formed by the levator aponeurosis), which originates as a muscle, becomes fibrous, and inserts into the anterior base of the tarsus. The Müller muscle is located in its posterior portion.
- In Caucasians, the insertion is in the superior part of the tarsus; in Asians, the insertion is lower, and thus it does not form the supratarsal crease.
- Tarsus.
- Pre-aponeurotic medial or central fat pads.
- Nasal or medial pad — inferior to tendon of the superior oblique muscle — lighter in color and more fibrous and denser.
Incisions: defat the skin with chlorhexidine-alcohol for better fixation of the marking ink. Marking performed with the patient in sitting position.
First marking is on the supratarsal crease, well-defined in Caucasians and poorly defined or absent in Asians.
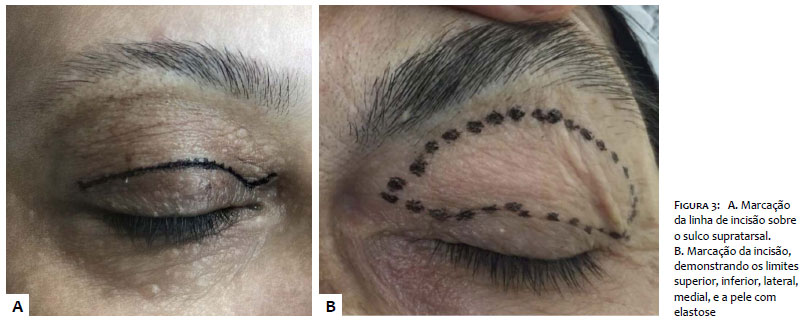
1st marking; demarcate the supratarsal crease (Figure 3a).
The distance between the supratarsal crease and the ciliary border varies from 6 to 8mm when measured at the mid-pupillary line.
As for the extremes of the incision, at the nasal canthus the scar should respect the palpebral aesthetic unit, not invading the lateral wall of the nose due to the risk of cicatricial bands and adhesions (fibrotic band of the medial canthus).
The aesthetic unit is more accommodating at the scar’s lateral canthus and can be extended, which improves the skin’s accommodation when necessary.
If not necessary, the scar can remain within the eyelids aesthetic unit. If it is necessary to prolong the incision, it should be kept within a natural crease or wrinkle of the skin. A lateral prolongation of the supratarsal crease is created.
The definition of the superior incision line is based on clinical assessment. This is where the state of the art comes into play in blepharoplasty. A combination of sensitivity and theory determine the site for this incision line.
The mid-pupillary line is marked.
One then identifies the highest point: the apex of the incision line will be located at this point (Figure 3b). Some characteristics dictate this point: the end of the palpebral elastosis when examining from inferior to superior. From the supratarsal crease onward, the skin is more damaged.
When the skin presents its natural characteristics again, the excision plane is finalized. Not all the cases will present this morphological difference which helps us in marking the upper limit of the area to excised, and in these cases, in which the limit between the elastotic skin and the healthy skin is not clear, the superior marking line should be made using the pinch test with an anatomical clamp or pachymeter, as shown in Figure 4a, joining the two extremities and thus preserving the palpebral rim, if that portion of the skin is needed for good closure of the palpebral rim.
Measurement of the distance between the supratarsal crease and the upper line of the surgical plane is essential for bilateral comparison, although 1mm or slightly more may exist as the difference between the two eyelids.
Tracing of the incision lines should always observe two factors: the natural closure of the palpebral rim, and that the incisions remain within the natural lines and thus be disguised when the eyes are open.
The pinch test of the entire region, from lateral to central, should be verified. Patients should open and close their eyes on command to perform this test.
The greatest risk and main cause of insecurity in one’s first surgeries of the upper eyelid is the removal of excessive skin,, leading to non-closure of the palpebral rim.
On the medial border, the risk involves formation of fibrous cicatricial bands.
On the lateral border, it is important to observe the distance between the superior ciliary border or the angle formed between the upper and lower lateral eyelids and the inferior incision line (supratarsal). A distance of less than 4mm can compromise the lymphatic drainage and cause chronic lymphedema of the upper eyelid.5 Figure 4c illustrates the minimum permissible limit between the lateral canthi and the incision line.
The lateral and medial extremities should allow access to the preseptal palpebral crease.
Another important factor for marking the superior incision line in the surgical plane is the relationship between the eyelid and eyebrow. Individuals with low eyebrows (the pattern seen in men) should not have a superior incision line very far from the supratarsal line. That is the distance between the mid-pupillary points and the supratarsal incision line and superior line should be sparing enough not to remove too much skin and lead to sunken eyes. The shadow formed by the eyebrow after removal of the skin will give the sensation of proximity between the eyebrow and ciliary border, producing a “sunken eye” appearance.
Patient in supine position.
Monitored (heart rate, arterial pressure, and oxygen saturation).
Surgeons’ preparation according to protocol, washing hands, drying, donning sterile gown and sterile gloves.
Antisepsis with aqueous chlorhexidine to avoid remo-ving previous marking of the surgical plane.
Placement of sterile surgical drapes.
Preparation of anesthetic and cooling solutions (Chart 2) and delicate surgical instruments (Chart 3).
It is essential to test the Kelly forceps’ grasping capacity with a folded gauze.
Anesthetize the lateral canthus and proceed to the medial canthus.
Use a 3ml syringe with a 30G needle. Pass the solution from the 10ml syringe (the 10ml syringe will always be used for the anesthetic solution and the 20ml syringe for the cooling solution). Use one needle for each side to always maintain an ideal thread in the first puncture. Prior organization of the surgical procedures clearly decreases the propensity to errors.
Conduct the punctures first along the supratarsal line to make a path for punctures, confirming the prior ink marking, return to the ipsilateral lateral canthus and trace the superior line of the plane. Hydrodissect the center of the surgical plane.
Mean volume used is 3ml per side.
After anesthesia, wait 15 minutes in order to obtain the proper vasoconstrictive effect.
Anesthetize the contralateral side in the same way. Incision: medial to lateral, bringing the incision towards yourself.
The canthi should end at sharp angles, less than 45 degrees.
Using toothed forceps, begin dissection of the skin. The removal should be delicate, because the skin is extremely thin (Figure 5a).
The excised skin should be kept in a kidney tray with saline solution (in case of need, serving as skin for grafting).
After removal of the skin, the orbicularis oculi muscle appears, especially its preseptal portion (Figure 5b).
Delicate pressure is exerted on the eyeball to assess the filling caused by the antero-superior shifting of the fat pads which are still contained by the fibrous septum and the orbicularis oculi muscle.
The curved scissor is used to remove linear portions of orbicularis oculi muscle in which there was turgidity caused by the pads.
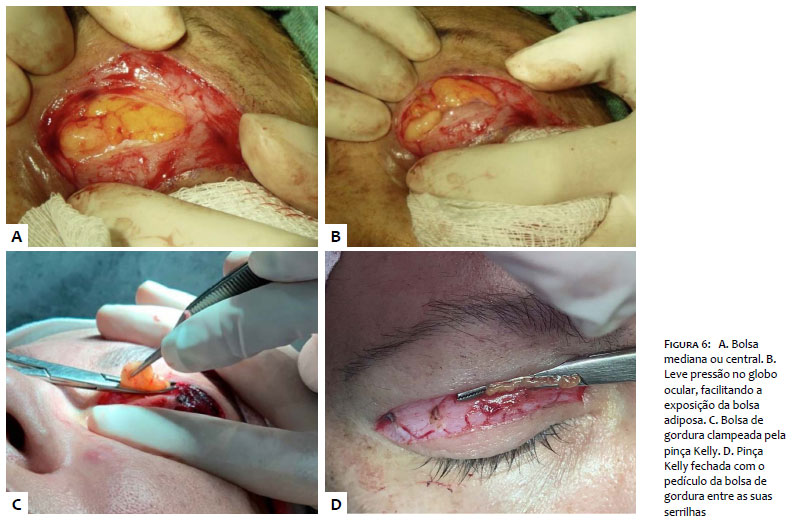
This begins in the projection of the central or medial pad, which is a pre-aponeurotic fat pad and is easily identified. It is goldish-yellow in color (Figure 6a).
The pad can be seen due to the transparency of the septum covering it. The septum is thin, and the pad has a soft appearance
Dissect the medial pad delicately with the help of a straight Kelly forceps with gauze wrapped around the tip, holding the pad with the toothed forceps. It is helpful to anesthetize the pad’s pedicle before grasping it. With the help of the toothed forceps, pull the pad and anesthetize its “pedicle” (actually the most proximal portion of the pad).
Soft pressure on the eyeball facilitates the pad’s exposure. Care and attention are necessary with bradycardia due to parasympathetic stimulus (Figure 6b).
After dissection of the pad, pressing the eyeball, the pad is clamped by its pedicle with the curved Kelly forceps, pretested for its grasping capacity as shown in Figure 6c.
Cut the pad with the curved scissors on the concave side of the Kelly forceps. The Kelly forceps is thus closed with the fat pads pedicle between its serrated jaws and the rest below it (Figure 6d).
Generous electrocoagulation is performed then with the electrocautery along the entire length of the jaws of the Kelly forceps, which are holding the remainder of the fat pad. Immediately after electrocoagulation, cooling is performed with the cooling solution.
This is the key moment in the surgery, in which the surgical assistant keeps constant gentle pressure on the eyeball and the Kelly forceps is opened. The surgeon verifies whether there is any bleeding in the fat pad, specifically prior to its grasp by the Kelly forceps. Electrocoagulation is performed on this portion, which is cooled again, and the assistant gently releases the pressure on the eyeball in order to allow retro-inferior retraction of the fat pad.
The same is done with the nasal pad. However, the nasal pad is deeper than the medial pad. The dissection should be performed very cautiously and gently. Again, pressure on the eyeball is required. Exteriorization of the nasal pad is more difficult, but more orderly, due to its greater consistency. The nasal pad is paler, denser, and more compact than the medial fat pad and is more protected by the fibrous septum.
Anatomical knowledge of the position of the tendon of the superior oblique muscle is important, located below the pad in order to avoid unintended trauma to this structure, which can cause strabismus and diplopia.15
During dissection of the nasal pad, the patient may feel some pain and discomfort, even with prior infiltration with the anesthetic solution.
Great care and attention are necessary in clamping the nasal pads “pedicle” with the curved Kelly forceps, in relation to the abovementioned tendon. Only the pad should be clamped.
Infiltration of anesthesia in the pad leaves it more tumescent and visible, and projects it more efficiently.
Again, the scissors rests against the concave side of the Kelly forceps and cuts the portion above the forceps.
Pressure is maintained to perform rigorous electrocoagulation and cooling, with immediate hemostasis. With pressure still on the eyeball, the jaws of the Kelly forceps are opened, with extreme attention to the presence of bleeding. Again, electrocoagulation is performed on the remaining portion of the fat pad, Cooling is performed, and the eyeball is decompressed to return the nasal pads pedicle to its superior and retrobulbar position.
Any bleeding from the pads’ “pedicles”, if left undetected and untreated, can lead to retrobulbar hematoma, an emergency situation with the risk of blindness and which requires immediate resolution, preferably by the ophthalmologist.
Some surgeons rigorously remove large extensions of the pads. Good results require removal of an excessive portion of the fat pads. Prior clinical assessment, and assessment at the moment of the decision on clamping, are essential for deciding how much of the pads should be removed.
A careful inspection is now made of the entire region. Direct visualization of the pads is not possible, since they have returned to their original position.
Electrocoagulation is performed on any bleeding points, which can be done from medial to central along the orbicularis oculi muscle to produce its retraction, on the line where the final scar will be located.
With the help of the Gilles hook and finetipped scissors, release the skin from the borders of the surgical plane to facilitate and optimize healing.
Edge-to-edge suture is performed with nylon 6.0 and simple or running intradermal sutures. The results are similar.
Having concluded the suturing, a cold compress is placed on the area. A practical approach is to tie two surgical gloves together by their wrists, filled with water, and freezing th em in advance. The gloves are positioned over the eyelids with the fingers pointing outwards, as shown in Figure 7, providing both cooling and gentle compression from the gloves’ weight. The eyelids should be protected with cotton gauze.
The longer tips of the sutures should be properly positioned in relation to the eyebrow to keep the thin, stiff tips from bothering the patient.
Raise the head of the gurney and then the patient’s bed and keep the compress cold.
Offer a light diet after 40 minutes, check vital and phy-siological signs, and if the patient is oriented in time and space, discharge is allowed.
The patient should continue to rest and follow the insinstructions provided during the preoperative visit.
Stitches may be removed on approximately day 5.
In the cases described here, the stitches were removed after five days, with no postop complications.
There was expected edema and ecchymosis, but no pain Two months after the surgery, good results were observed, with maintenance of correct positioning of the eyelids and absence of irritative symptoms in the eyeball (Figures 8, 9, and 10).
Blepharoplasty provides relief of the tired-looking face, signs of aging, and midface ptosis.
With aging, the eyelids’ skin tends to sag and the eyes’ supporting musculature loses its tone, tending to form fat pads under the eyelids. The sagging musculature, excess skin, and her-niation of the fat pads produce a tired, aged appearance.
Blepharoplasty is a surgical technique that produces great benefits and patient satisfaction by attenuating the flaccidness and palpebral ptosis, when used alone or in combination with other currently available treatments.
Since blepharoplasty can be performed under local anesthesia, without sedation, it may be considered a simple surgery, without complications and with low morbidity, as long as properly indicated and performed correctly with all the necessary care.
Blepharoplasty not only gives the patient a younger appearance, but also meets a functional need by lending a less tired expression and improving the field of vision.
The dermatological surgeon who is accustomed to removing carcinomas from the eyelids and performing concomitant reconstruction has already done reconstructive blepharoplasties, although perhaps without realizing it. Reconstructive surgery of eyelids after removal of a cancer is certainly more complex than when performed for aesthetic reasons and with prior markings and planning.
Proper preoperative assessment, detailing the surgery’s benefits and limitations, avoids problems and false expectations. This has shown that blepharoplasty is a safe and effective option with good functional and aesthetic results, low complication rates, and good acceptance by patients.
Érico Pampado Di Santis | 0000-0001-5782-9205
Conception, planning, data analysis, writing of the article or critical intellectual revision, and responsibility for the final approval for publication.
Patrícia Holderbaum | ORCID 0000-0003-0116-2602
Conception, planning, data analysis, writing of the article or critical intellectual revision, and responsibility for the final approval for publication.
Natália Machado Mildner | ORCID 0000-0001-9220-8092
Data analysis, writing of the article, and responsibility for the final approval for public
Larissa Ethel Soriano Freire | ORCID 0000-0003-2915-3660
Data analysis, writing of the article, and responsibility for the final approval for public
Denise Steiner | ORCID 0000-0001-6450-9234
Data analysis, writing of the article, and responsibility for the final approval for public
1. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119(7):2219-27.
2. Rohrich RJ, Arbique GM, Wong C, Brown S, Pessa JE. The anatomy of suborbicularis fat: implications for periorbital rejuvenation. Plast Reconstr Surg. 2009;124(3):946-51.
3. Lambros V. Observations on periorbital and midface aging. Plast Reconstr Surg. 2007;120(5):1367-76.
4. Ghavami A, Pessa JE, Janis J, Khosla R, Reece EM, Rohrich RJ. The orbicularis retaining ligament of the medial orbit: closing the circle. Plast Reconstr Surg. 2008;121(3):994-1001.
5. Coleman WP, Thomas WH, Asken S. Cirurgia cosmética-princípios e técnicas. 2nd ed. Rio de Janeiro: Revinter; 1997.
6. Moore KL, Dalley AF, Anatomia orientada para a clínica. 4th ed. Rio de Janeiro: Guanabara Koogan; 2001.
7. Pitangy I, Sbrissa RA. Atlas de cirurgia palpebral. Rio de Janeiro: Revinter; 1994.
8. Palermo EC. Anatomy of the periorbital region. Surg Cosmet Dermatol. 2013;5(3):245-56.
9. Kaminer MS, Dover JS, Arndt KA. Atlas of Cosmetic Surgery. Saunders. 2002;351-384.
10. Palermo EC. Rejuvenescimento da região palpebral. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 455-87.
11. Robinson JK, Hanke CW. Cirurgia da pele: procedimentos em dermatologia. 3rd ed. Rio de Janeiro: Elsevier; 2016.
12. Salasche SJ, Bernstein G, Senkarik M. Surgical anatomy of the skin. Estados Unidos: Appleton & Lange; 1988.
13. Gadelha AR, Costa IM. Cirurgia dermatológica em consultório. 2nd ed. Rio de Janeiro: Atheneu; 2009.
14. Codner MA, McCord CJ. Cirurgia palpebral e periorbitária. 2nd ed. Rio de Janeiro: Dilivros; 2016.
15. Oestreicher J, Mehta S. Complications of Blepharoplasty: Prevention and Management. Plast Surg Int. 2012;2012:252368.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}