


Caroline Baima de Melo1; Ana Lúcia França da Costa1; Guilherme de Carvalho Paulo Marcos1, In memoriam; Marília Medeiros de Sousa Santos2; Giovanna de Carvalho Paulo Marcos3
Received on: 25/03/2019
Approved on: 25/11/2019
Financial support: None
Conflict of interests: None
Study conducted in the Dermatology Outpatient Clinic, Hospital Universitário da Universidade Federal do Piauí (HU-UFPI), Teresina (PI), Brazil
INTRODUCTION: Cutaneous squamous cell carcinoma may originate from premalignant lesions, with actinic keratosis (AK) being the most frequent. The field cancerization is defined as an area of apparently healthy skin, but with important photodamage around the AK lesions. In this study, we compared imiquimod, an immunomodulator , to a medium-strength chemical peel, with Jessner’s solution combined with 35% trichloroacetic acid.
OBJECTIVE: To compare the efficacy/ acceptability of the two methods in treating the facial field cancerization.
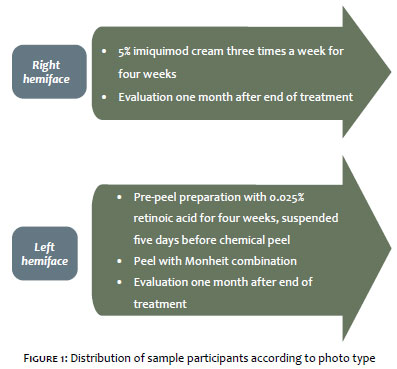
METHODS: Ten patients who underwent the two forms of treatment were selected: in one hemiface, they used 5% imiquimod cream three times a week for 4 weeks; in the other, they applied the medium-strength chemical peel, with Jessner’s solution combined with 35% trichloroacetic acid. Patients were evaluated 30 days after the end of the treatment by counting the AKs and recording the degree of patient satisfaction and the adverse effects with both treatment modalities.
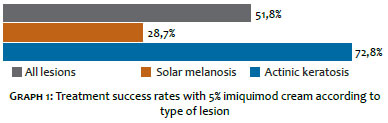
RESULTS: Treatment with imiquimod led to the resolution of 51.8% of the AKs and melanoses together and 72.8% when only the AKs were evaluated. Peeling treated 74.9% of AKs and melanoses and 79.1% of AKs. All patients felt satisfied at some level with both forms of treatment, with greater satisfaction with the chemical peel.
CONCLUSION: Both modalities were effective, but the chemical peel was more efficient and easier to apply, however, with more intense adverse effects
Keywords: Skin, cancer; Keratosis, actinic; Chemexfoliation
Actinic keratosis (AK) or solar keratosis is a highly frequent premalignant lesion that occurs mainly in light-skinned adults and elderly individuals, due to chronic exposure to ultraviolet radiation. Clinically, AK presents as a papular lesion covered with dry scales, with a rough surface and variable color, located predominantly on sun-exposed areas such as the face, neck, ears, neckline, forearms, and backs of hands, and the scalp of bald men1,2 These lesions not only serve as a sensitive and reliable marker of exposure to ultraviolet radiation, but are also precursors of potentially invasive squamous cell carcinomas. The potential for carcinogenesis of solar keratoses remains uncertain, but it is estimated that in patients with multiple lesions, it ranges from 6 to 10% in ten years.3 Malignant degeneration is more common in individuals with light skin, advanced age, excessive solar exposure, and immunosuppression.
Histological studies show that the majority of cutaneous squamous cell carcinomas are derived from actinic keratosis lesions. It is still not possible to predict exactly which AK lesions will progress to SCC, thus requiring their prompt treatment.4
The term "field cancerization" was coined by Slaughter in 1953 when studying the histological alterations in peritumoral tissues of squamous cell carcinoma, where he observed the emergence of new and multiple primary lesions.5 The concept is based on the fact that apparently normal skin around actinic keratosis lesions contains subclinical preneoplastic abnormalities – evidenced by histological tests and molecular analyses -, that allow the emergence of new lesions and local recurrence.6 Field cancerization can be diagnosed clinically via findings, upon dermatological examination, of multiple AK lesions and other conditions such as solar lentigo, pigmentation disorders, altered skin texture, wrinkles, xerosis, and solar elastosis.
Imiquimod is an immunomodulator derived from the imidazoquinoline family and whose mechanism of action is still largely unknown. The drug acts by inhibiting tumor proliferation through the toll-like receptor7, acting as a stimulator of immune response and inducer of tumor apoptosis.7,8 Its use is approved in humans for lesions resulting from papilloma virus infection and is also used, with variable response, in the treatment of actinic keratoses, basal cell carcinoma, Bowen's disease, squamous cell carcinoma, epitheliotropic lymphoma, and keratoacanthoma.
Chemical peels are the application of one or more caustic agents on the skin, so as to generate controlled destruction of the skin's layers. Chemical peels are classified as superficial (complete or partial destruction of the epidermis), medium (reaching the papillary dermis), and deep (lesion down to the mid-reticular dermis).9 The medium form of peel has been the most widely used in clinical practice, with the sequential combination of the application of Jessner's solution (association of resorcinol, salicylic acid, and lactic acid, with ethanol as the vehicle), followed by 35% trichloroacetic acid. It is safe, easy to apply, and has a wide range of applications, including actinic keratoses, photoaging, and dyschromia. The initial application of Jessner's solution allows more rapid absorption of the second chemical agent.10
The study's objective was to compare the efficacy and acceptability of the two treatment modalities for field cancerization of the face, as well as to objectively observe the number of AK lesions before and after the treatments and to verify the side effects of the medications used.
The study was approved by the Institutional Review Board of HU–UFPI under protocol 67283517.2.0000.8050. Study subjects signed a free and informed consent form. This was a prospective, longitudinal intervention study with a researchers' convenience sample of 10 patients diagnosed with field cancerization of the face at the Dermatology Outpatient Clinic of Hospital Universitário, Universidade Federal do Piauí (HU-UFPI), Brazil. The principal criterion for choice of patients was ease of access, with preference for patients residing in Teresina, the capital city of Piauí State, since there was a limited amount of the investigation drug available. The attempt was to minimize treatment dropout and loss of patient follow-up.
In order to be included in the study, participants needed to have at least ten lesions consistent with actinic keratosis of the face or at least five on each hemiface. The sample excluded patients already in treatment or over 80 years of age.
Participants were instructed to apply 5% imiquimod cream (Modik® Germed Pharma, Fortaleza CE, Brazil) on the right hemiface three times a week for four weeks. On the left hemiface, they were instructed to perform the pre-peel preparation with the daily application of 0.025% retinoic acid for four weeks. The topical medication was suspended five days before the Monheit chemical peel (Jessner's solution followed by 35% trichloroacetic acid). (Figure 1)
All the participants were submitted to both forms of treatment in order to make the comparator groups as equivalent as possible and to avoid selection bias. The sample was chosen at the authors' convenience and not randomly (a potential limitation to the study). All formulas for calculating sample size for clinical trials provide for random choice of participants, which is not the case in the current study.
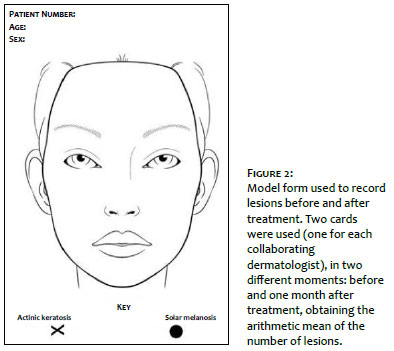
Lesions consistent with actinic keratosis were recorded before treatment and one month afterwards, on forms prepared specifically by the authors.
Evaluation of the presence of AKs was done by two collaborating dermatologists who were unaware of which treatment had been performed on each hemiface (single-blind study), 30 days after the end of the treatments. The number of lesions used to evaluate the results was the simple arithmetic mean of the sum obtained from the evaluation forms completed by the collaborators. (Figure 2)
The participants' degree of satisfaction with the treatments was analyzed with a questionnaire prepared by the project's authors, based on the previously published Treatment Satisfaction Questionnaire for Medication, version 1.4.
Data obtained on the treatments' efficacy and patient satisfaction with the treatments were compared and recorded on graphs and tables.
Ten patients were evaluated (eight females and two males). One female patient dropped out of follow-up after the end of treatment. The total sample thus consisted of nine patients.
As for age bracket, five participants (55.6%) were in their seventies, two (22.2%) were in their sixties, and two (22.2%) were in their fifties.
Patients had a mean of 98.5 lesions on the area treated with 5% imiquimod cream, considering actinic keratoses and solar melanoses, with resolution of 51 of these lesions (51.8%) and 47.5 remaining lesions (48.5%). Considering only actinic keratoses, resolution was 72.8% (with 14 remaining lesions out of a total of 51.5). (Graph 1)
Patients had a mean of 117.5 lesions, considering AKs and solar melanoses, on the area treated with the medium peel. Resolution was 74.9% (88 lesions, with 29.5 remaining lesions). When evaluated separately, actinic keratoses showed 79.1% treatment success (resolution of 55 of the lesions).
Patients were interviewed as to their degree of satisfaction with the two treatments. The majority of patients (88.9%) reported that they were satisfied with the results with 5% imiquimod cream, considering the long treatment time and ease of treatment (66.7%). As for the Monheit peel, the majority were satisfied (55.6%), while an important share (33.3%) were extremely satisfied with the results; 88.8% found the treatment acceptable or not too prolonged, and 55.5% found the treatment easy.
At the end of the interview, patients were asked which treatment they would choose for the entire face. Seven (77.8%) said they preferred the peel, while two (22.2%) preferred imiquimod.
All the patients reported side effects, regardless of the treatment modality. They all reported erythema and peeling, while two (22.2%) and five (55.6%) reported ulcerations and wounds on the application site for 5% imiquimod cream and the peel, respectively. Most of the patients found the side effects occasionally uncomfortable (77.8% in the case of the imiquimod cream) or very uncomfortable (44.4% with the chemical peel).
There were no reports of secondary infection, milium, or herpes simplex. (Figure 3)
Actinic keratoses were the fourth most frequent diagnosis in the Dermatology Outpatient Clinic in a case series conducted in Brazil in 2006, accounting for 5.1% of the conditions assessed.11 They are the most frequent lesions in the spectrum of squamous cell carcinoma, and in this context the natural history can evolve to three outcomes: involution, persistence, and differentiation into in situ or invasive SCC. The malignant conversion rate remains uncertain, with studies showing extremely variable rates, ranging from 0.1% to 20%. Prevalence in the population older than 40 years in the Northern Hemisphere ranges from 11% to 25%.12 Field cancerization of the skin can be defined as an area with important solar exposure, chronically damaged skin, with multiple solar keratosis lesions, in addition to other findings of damage from exposure to UV radiation. The most widely used drugs in topical treatment of AK are 5-fluorouracil, imiquimod cream (5% and 3,75%), and 3% sodium diclofenac gel.
5% imiquimod cream was initially used for treatment of genital and perianal warts. It was used off-label to treat various conditions, such as Bowen's disease, invasive SCC, malignant lentigo, molluscum contagiosum, keloid scars, and other diseases. It was later approved for treatment of actinic keratosis, including superficial AK.
Imiquimod is used in various ways to treat AKs. Three studies assessed treatment with the 5% formulation, three times a week for four weeks, where overall resolution of lesions ranged from 54% to 69%.13 In our study, the rate was 72.8%, thus higher than in previously published studies. When used according to the package insert instructions, the therapeutic success rates are higher (84%). No studies were found on the destructive potential of imiquimod in solar melanoses, caused by the final inflammatory effect on field cancerization. Local inflammation is known to be part of imiquimod's mechanism of action.14
Various adverse effects have been reported, but almost always restricted to the application sites, such as erythema, pruritis, burning sensation, erosions, and ulcerations.
All the patients reported some side effect from the use of imiquimod, and 22,2% reported important side effects such as ulcerations and wounds. This is consistent with the literature, since the studies report frequent skin reactivity, with 31% showing severe erythema, 30% crusts, and 19% ulcerations15 Most of the patients reported that the side effects were somewhat uncomfortable (77,8%), which is also corroborated by the literature, stating that the medication is well-tolerated.16
Stockfleth et al. reported that 84% of lesions treated with 5% imiquimod cream resolved with a 12-week cycle, but that local irritative reactions were common.17 However, this was not the treatment time used in our study, which may explain the lower therapeutic response.
Jessner's solution is a chemical peel formulation consisting of the association of salicylic acid, lactic acid, and resorcinol. This combination was initially used by Monheit and uses all three compounds' keratolytic capacities with resorcinol's depigmenting capacity to enhance the effects, even at lower concentrations.18 When used before trichloroacetic acid, the absorption is increased, promoting medium-depth destruction.
Caroline Baima de Melo | 0000-0003-1497-6568
Intellectual participation in the propaedeutic and/or therapeutic management of the study cases, critical revision of the manuscript.
Ana Lúcia França da Costa | 0000-0002-3451-5294
Approval of the final version of the manuscripts, conception and planning of the study, effective participation in orientation of the research.
Guilherme de Carvalho Paulo Marcos (In memoriam)
Data collection, analysis and interpretation.
Marília Medeiros de Sousa Santos | 0000-0003-4136-6984
Elaboration and writing of the manuscripts, critical review of the literature.
Giovanna de Carvalho Paulo Marcos | 0000-0001-5834-869x
Approval of the final version of the manuscripts, conception and planning of the study, effective participation in orientation of the research
1. Costa C, Scalvenzi M, Ayala F, Fabbrocini G, Monfrecola G. How to treat actinic keratosis? An update. J Dermatol Case Rep. 2015;9(2):29-35.
2. Berker D, McGregor JM, Hughes BR. Guidelines for the management of actinic keratoses Br J Dermatol. 2007;156(2):222-30.
3. Abdalla B, Rstom SA, Paschoal FM. Field cancerization: a review article. Surg Cosmetic Dermatol. 2014;6(4):310-8.
4. Martinez MAR, Francisco G, Cabral LS, Ruiz IRG, Neto CF. Molecular genetics of non- melanoma skin cancer. An Bras Dermatol. 2015;81(5):405-19.
5. Torezan LAR, Festa-Neto C. Cutaneous field cancerization: clinical, histopathological and therapeutic aspects. An Bras Dermatol. 2013;88(5):779-91.
6. Berman B, Cohen DE, Amini S. What is the role of field-directed therapy in the treatment of actinic keratosis? Part 1: overview and investigational topical agents. Cutis. 2012;89(5):241-50.
7. Smith K, Hamza S, Skelton H. Topical imidazoquinoline therapy of cutaneous squamous cell carcinoma polarizes lymphoid and monocyte/macrophage populations to a Th1 and M1 cytokine pattern. Clin Exp Dermatol. 2004;29(5):505-12.
8. GarcezI T, Gerardi D, Ferreira K, Cardoso C, Möschbacher P, Contesini E. Topical treatment of actinic keratosis with imiquimod 5% cream. Arq Bras Med Vet Zoo. 2012;64(6):1522-8.
9. Almeida ART, Camargos GPC. Procedimentos cosméticos pouco invasivos. In: Criado, PR et al. Tratado de Dermatologia. 2 ed. Vol. 2. São Paulo: Editora Atheneu, Capítulo 127. p. 2437-2452, 2014.
10. Lawrence N, Cox S, Cockerell C, Freeman R, Cruz Jr P. A Comparison of the Efficacy and Safety of Jessner's Solution and 35% Trichloroacetic Acid vs 5% Fluorouracil in the Treatment of Widespread Facial Actinic Keratoses. Arch Dermatol. 1995;131(2):176-81.
11. Sociedade Brasileira de Dermatologia. Perfil nosológico das consultas dermatológicas no Brasil. An Bras Dermatol. 2007;81(6):549-58.
12. Quaedvlieg PJF, Tirsi E, Thissen MRTM, Krekels GA. Actinic keratosis: how to differentiate the good from the bad ones? Eur J Dermatol. 2006;16(4):335-9.
13. Krawtchenko N, Roewert-Huber J, Ulrich M, Mann I, Sterry W, Stockfleth E. Arandomised study of topical 5% imiquimod vs. topical 5-fluorouracil vs. cryosurgery in immunocompetent patients with actinic keratoses: a comparison of clinical and histological outcomes including 1-year follow-up. Br J Dermatol. 2007;157( Suppl 2):34-40.
14. Gupta AK, Davey V, Mcphail H. Evaluation of the effectiveness of imiquimod and 5- fluorouracil for the treatment of actinic keratosis: Critical review and meta-analysis of efficacy studies. J Cutan Med Surg. 2005;9(5):209-14.
15. Szeimies RM, Gerritsen MJ, Gupta G, Ortonne JP, Serresi S, Bichel J, et al. Imiquimod 5% cream for the treatment of actinic keratosis: results from a phase III, randomized, double-blind, vehicle-controlled, clinical trial with histology. J Am Acad Dermatol. 2004;51(4):547-55.
16. Lebwohl M, Dinehart S, Whiting D, Lee PK, Tawfik N, Jorizzo J, et al. Imiquimod 5% cream for the treatment of actinic keratosis: results from two phase III, randomized, double- blind, parallel group, vehicle-controlled trials. J Am Acad Dermatol. 2004;50(5):714-21.
17. Stockfleth E, Ferrandiz C, Grob JJ, Leigh I, Pehamberger H, Kerl H, et al. Development of a treatment algorithm for actinic keratoses: a European consensus. Eur J Dermatol. 2008;18(6):651-9
18. Monheit GD. The Jessner's + TCA peel: a medium-depth chemical peel. J Dermatol Surg Oncol. 1989;15(9):940-50.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}