


Kathleen Cézar de Mélo1; Aisla Graciele Galdino dos Santos1; José Roberto Amorim1; Tânia Rita Moreno de Oliveira Fernandes2; Carlos Dornels Freire de Souza1
Received on: 02/11/2019
Approved on: 16/12/2019
Financial support: None
Conflict of interests: None
Study conducted at the Department of Medicine, Universidade Federal de Alagoas, Arapiraca (AL), Brazil
INTRODUCTION: In Brazil, skin cancer is the most common type of cancer, and melanoma is the most lethal.
OBJECTIVES: To analyze the temporal trend of mortality due to melanoma in Brazil between 2000 and 2016.
METHODS: Ecological time-series study involving all deaths from melanoma in Brazil from 2000 to 2016. The crude death rate, adjusted for the Brazilian population and the world population, was analyzed. For the analysis, we used the regression model by inflection point with 5% significance.
RESULTS: In the period, 22,963 deaths from melanoma were recorded in Brazil, with an increasing trend in the crude death rate (2.6%), and in the adjusted rates for the Brazilian (0.6%) and the world population (0.5%). In the Southeast, we observed a steady trend in the crude death rate and the adjusted rate for the Brazilian population, as well as a decreasing trend in the world population rate. The crude death rate (77.77%; n=21); the Brazilian population (59.25%; n=16), and the world population adjusted rates (55.55%; n=15) presented an increasing trend. Only São Paulo and Rio de Janeiro showed a decreasing trend in the death rate adjusted for the Brazilian and the world population.
CONCLUSIONS: The study showed an increase in mortality from melanoma in Brazil. Policies should be implemented to favor early diagnosis and timely treatment.
Keywords: Melanoma; Time series studies; Epidemiology
Melanoma is a malignant tumor that originates from melanocytes, skin cells responsible for the production of melanin,1 that protects against damage caused by ultraviolet radiation (UV).2 The development of melanoma is a consequence of the loss of the genetic mechanisms of cell control, caused mainly by UVA and UVB radiation.1 It usually has a primary cutaneous location, but can appear on mucosal surfaces (oral, conjunctival, vaginal), and within the uveal tract of the eye and in leptomeninges.2,3,4
Among the risk factors for the development of melanoma skin cancer, we can highlight genetics, skin phenotype, numbers of nevi, family, and environmental history.1,3 Excessive exposure to the sun, with sunburn, especially in the first 20 years of life, is the most significant environmental factor as well as artificial tanning, especially in people with fair skin and eyes.1,4
These tumors are characterized by significant morbidity due to the great potential for metastasis.3,4 Thus, the development of campaigns and investments to prevent skin cancer are justified to diagnose it early, as it increases the possibility of curing melanoma in situ.1
In 2018, 287,723 new cases of melanoma were estimated in the world, representing an incidence rate of 3.8 cases for every 100 thousand inhabitants. Of these, 150,698 cases (3.9/100 thousand) occurred in men and 137,025 in women (3.6/100 thousand). That same year, 60,712 deaths were recorded worldwide (0.8/100 thousand). Among men, the number of deaths from melanoma skin cancer was 34,831 (0.9/100 thousand) and among women, 25,881 (0.68/100 thousand).5,6,7
In Brazil, skin cancer is the neoplasia with the highest incidence, and the estimate of non-melanoma skin cancer (basal and squamous cell carcinoma) for the year 2018 was 165,580 cases (85,170 new cases among men and 80,410 among women) for each year of the 2018-2018 biennium. Regarding melanoma, despite its high lethality, its incidence is low, with 6,260 cases (2,920 new cases in men and 3,340 in women), although an expressive growth is observed in populations of white skin color.8,9
Most of the theoretical framework on melanoma comes from studies conducted in countries with different sociodemographic and geographic characteristics, showing a lack of information in Brazil. Based on the above, this study aims to analyze the temporal trend in melanoma mortality in Brazil between 2000 and 2016.
Ecological, time-series study involving all deaths due to skin melanoma recorded in Brazil from 2000 to 2016.
The study conducted in all Brazilian regions, that is, North, Northeast, Midwest, Southeast, and South, including the 26 Brazilian states and the Federal District. According to the demographic census of the Instituto Brasileiro de Geografia e Estatística (IBGE), in 2010, the Brazilian population was 190,755,799 people, and the region with the largest number of inhabitants was the Southeast.10 Regarding the world classification of the Human Development Index (HDI), Brazil occupies the 75th position, with an HDI of 0.755, being classified as high human development.11,12
The following indicators were analyzed: crude mortality rate from malignant skin melanoma, mortality rate adjusted by the Brazilian population, and the mortality rate adjusted by the world population. Data were collected from the Online Mortality Atlas of the National Cancer Institute José Alencar Gomes da Silva (INCA). The filters used in the research were: both sexes, location, malignant skin melanoma (ICD-10 C43), from 2000 to 2016. It should be noted that the rates were obtained already calculated by the INCA platform.
For the temporal analysis, the regression model by inflection points (Joinpoint regression model) was used. The model tests whether a line with multiple segments is statistically more adequate to describe the temporal evolution of a set when compared to a straight line or to a line with fewer segments.13 The trends were classified as increasing, decreasing, or stationary, according to the slope of the regression line. The percentage of annual variation (APC, Annual Percent Charge) was calculated considering a 95% confidence interval (95% CI) and 5% significance. The analysis was performed using Joinpoint regression software (version 4.5.0.1, National Center Institute, Betheseba, MD, USA).
The study did not require approval from the ethics committee, as it used secondary public domain data, and there was no individual identification of any patient.
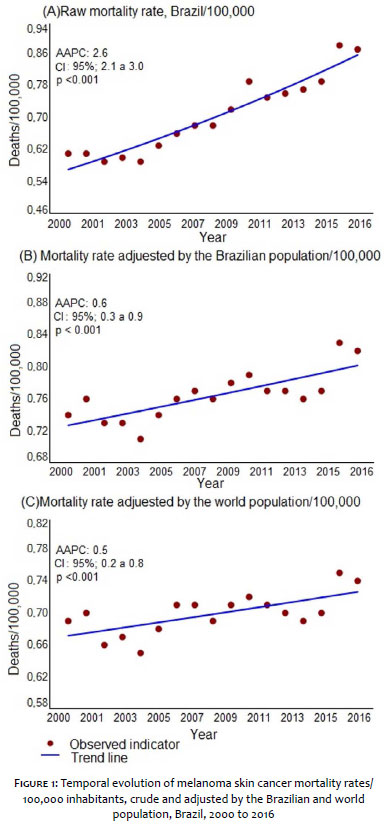
In the period studied, 22,963 deaths from melanoma were recorded in Brazil. The analysis of time series in Brazil showed an increasing trend in the crude mortality rate (APC: 2.6; 95% CI: 2.1 to 3.0; p<0.001), rising from 0.61 to 0.87/ 100,000. The rate adjusted by the Brazilian population (APC: 0.6; 95% CI: 0.3 to 0.9; p<0.001) and the rate adjusted by the world population (APC: 0.5; 95% CI: 0.2 to 0.8; p<0.001) showed the same increasing trend (Figure 1).
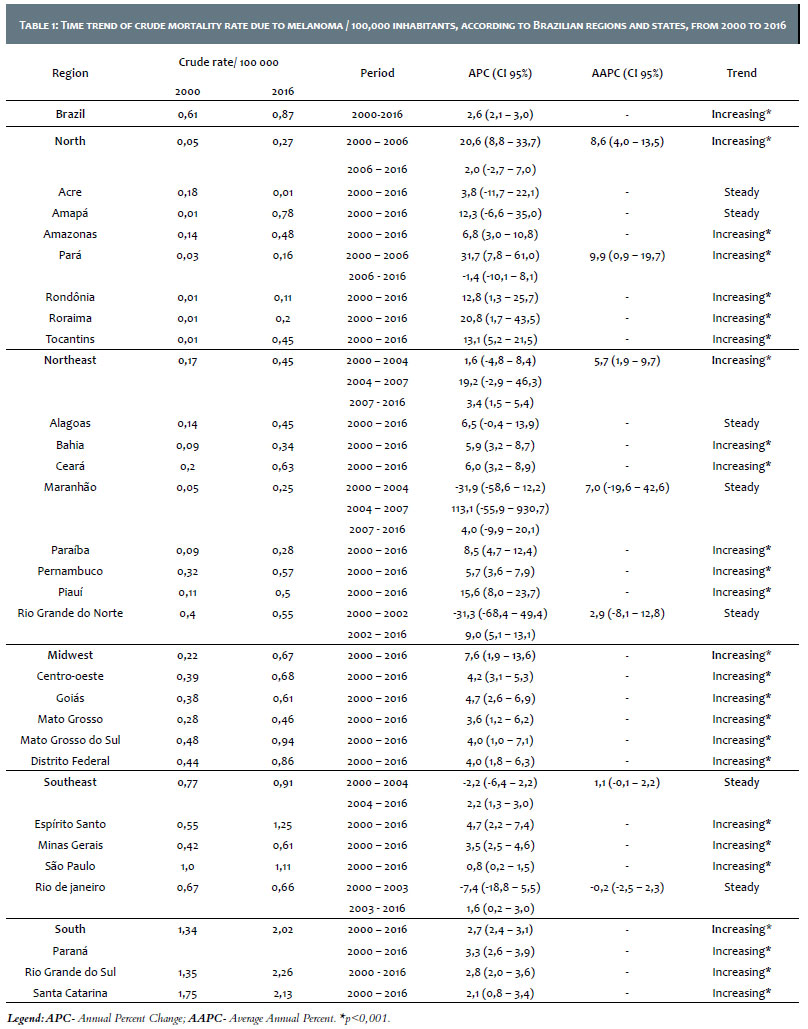
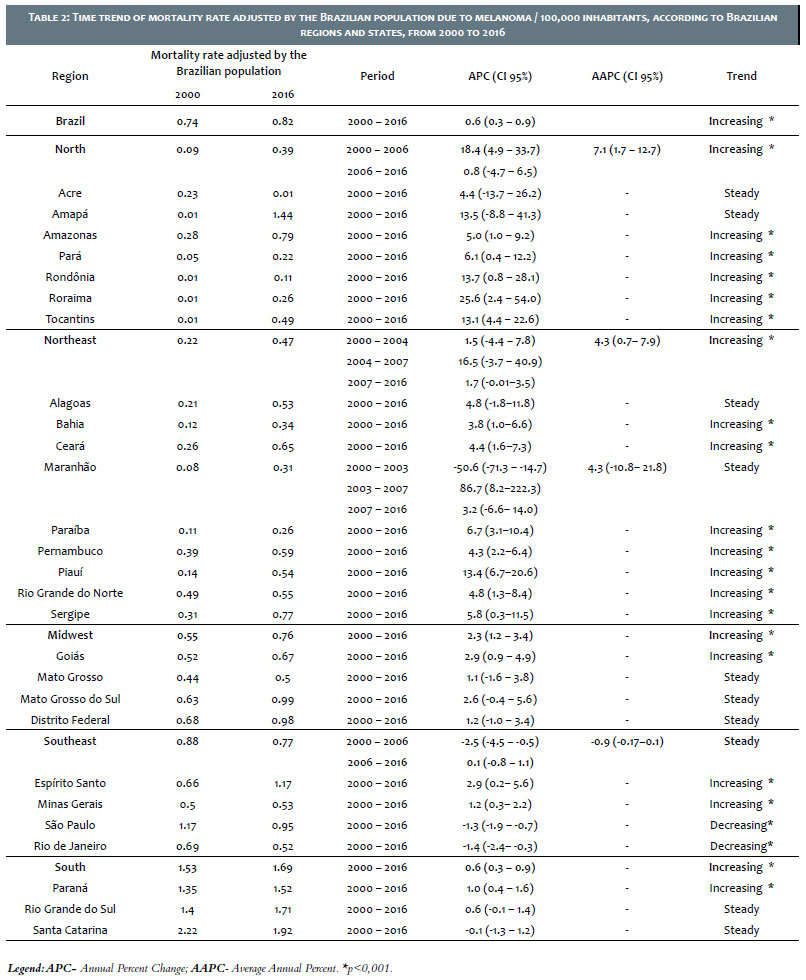
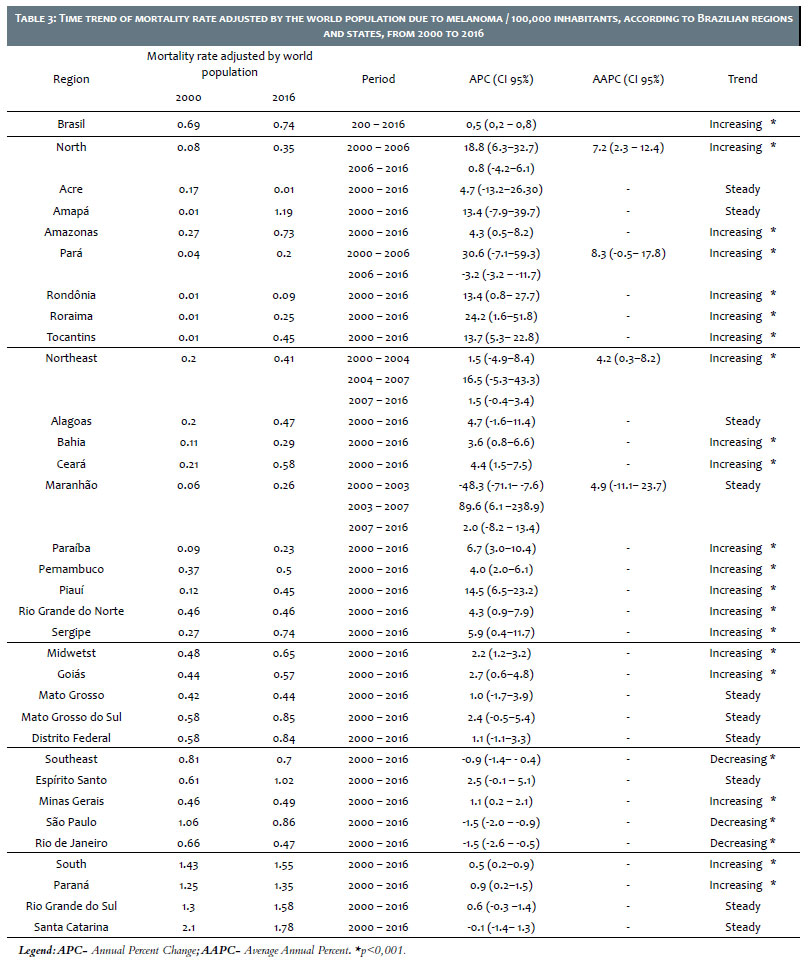
In the analysis according to regions, four of them (North, Northeast, Midwest, and South) showed a growth trend, and the North stood out with the highest percentage of mean variation in the crude rate (AAPC: 8.6; CI 95 %: 4.0 to 13.5; p<0.001), increasing from 0.05 to 0.27/100,000 at the rate adjusted by the Brazilian population (AAPC: 7.1; 95% CI: 1.7 to 12.7; p<0.001) and in the rate adjusted by the world population (AAPC: 7.2; 95% CI: 2.3 to 12.4; p<0.001). In contrast, the Southeast region showed a steady temporal behavior in the crude rate and in the rate adjusted by the Brazilian population, and a downward trend in the rate adjusted by the world population (APC: -0.9; 95% CI: -1.4 to -0.4; p<0.001) (Tables 1, 2 and 3).
In the analysis according to the states, 77.77% (n = 21) of them showed a tendency to increase the crude mortality rate, 59.25% (n=16) in the mortality rate adjusted by the Brazilian population, and 55.55% (n=15) in the mortality rate adjusted by the world population. In parallel, no state showed a decreasing trend in the crude rate. In contrast, only São Paulo and Rio de Janeiro showed a decreasing trend both in the mortality rate adjusted by the Brazilian population (AAPC: -1.3 and -1.4, respectively), and in the rate adjusted by the world population (AAPC: -1.5 and -1.5, respectively) (Tables 1, 2 and 3).
The incidence of melanoma in the world has increased in recent decades and, despite corresponding to less than 5% of skin cancers, it causes about 95% of deaths.14 Publications in Brazil and/or Latin America are limited to descriptive studies or in small case series,14 which justifies conducting investigations on the theme.
This paper assessed the mortality trend of melanoma skin cancer in Brazil, whose rates showed a growth trend in the period from 2000 to 2016. The discussion must be carried out from two perspectives: the first refers to changes in the pattern of sun exposure observed in the last decades, and the second, the highest number of diagnoses and notifications of the disease.
Intentional sun exposure is the main factor associated with an increased rate of melanoma incidence worldwide.15 The change in the aesthetic and socioeconomic standards on tanned skin began in the industrial revolution. With the emergence of factories, exposure to the sun has ceased to be occupational to be recreational, becoming a symbol of a higher economic condition.1,15,16 Thus, changes in the habits of the population throughout history, characterized by greater sun exposure, associated with the aesthetic appreciation of skin tanning, natural and/or artificial, and the increase in UV radiation, contributed to the expansion of the disease, making it a public health problem.17
In a tropical country like Brazil, these cultural changes, especially from the 1920s onwards, favored outdoor recreational activities even more, inducing an excessive exposure to ultraviolet solar radiation, especially among young people.1,15,16 At the same time, labor activities with exposure to the sun are still observed in the national territory, such as, for example, rural workers and informal commerce in the streets of urban centers.1,18,19,20,21,22 Research conducted in Pernambuco,23 involving fishers, showed a high prevalence of photo-exposure lesions.
International studies indicate an association between exposure to UV radiation and the occurrence of melanoma. In an investigation conducted in France, 83% of the 10,340 cases of melanoma recorded in 2015 were attributed to UV exposure.24 Similar results were also observed in the United Kingdom (86%) 25 and in Australia (95%).26 UV rays are recognized as carcinogenic, acting in the initiator and promoter regions of the genes, causing imbalance in the cell cycle.1,24
Since 1999, the Brazilian Society of Dermatology (SBD) started the National Campaign for the Prevention of Skin Cancer (Campanha Nacional de Prevenção do Câncer de Pele - CNPCP) in the main cities of the country, resulting in 566,873 visits since its implementation until 2016.17,27,28 This secondary prevention mechanism, based on early detection with massive attendance by the population, resulted in a detection rate of approximately 10%.29 In the long term, this early detection implies a reduction in mortality, as observed in the Southeast region and the states of São Paulo and Rio de Janeiro. A national survey conducted from 1980 to 2009 showed a decreasing trend in melanoma mortality, with emphasis on the Southeast region.30
It is essential to highlight that the inequality in conducting these campaigns may justify the heterogeneity of regional rates. The lower number of detection campaigns in the North region may justifies the higher mortality rate in that location, as observed in this study. From 2001 to 2005, for example, only one campaign was conducted in the state of Tocantins and two in Acre.17
In developed countries, studies have shown beneficial effects of these campaigns on early diagnosis and treatment in the early stages,31 resulting in an impact on patient survival. Research conducted in the United States showed an increase in the five-years survival after the diagnosis of melanoma, from 50% in 1950 to 90% in 1990.32 In a Brazilian study in the city of Jaú/SP, the survival rate varied from 100% in stage I to 0% in stage IV.31,33
The time between the onset of the disease and the diagnosis is a determining factor for the outcome. According to the staging of the American Joint Committee on Cancer (AJCC), the thickness of the tumor, ulceration, and mitotic rate are determining factors for the unfavorable outcome. Among the evaluation mechanisms, the Breslow Index stands out, which evaluates the tumor thickness, in millimeters, by histopathological examination and is an important prognostic factor to assess survival, the risk of local recurrence, as well as regional and distant metastases34,35: Breslow indicators <1mm are considered low risk and have an excellent prognosis for survival, which can lead to zero mortality. Diagnosis during this phase decreases mortality by 48% and, consequently, indicates an estimated 151% increase in survival.35
Even considering the methodological care, it is necessary to highlight some limitations. The first refers to the use of secondary data, influenced by the under-registration of deaths since the Mortality Information System (Sistema de Informações sobre Mortalidade - SIM) presents a wide variation in the coverage between the country regions. The second limitation concerns the lack of standardization in data collection and centralization, making it difficult to carry out investigations and comparisons between regions. And the third refers to the lack of epidemiological studies, which makes it challenging to discuss the topic.
Melanoma skin cancer can be considered an important public health problem in Brazil, because, despite its low incidence, it has high mortality rates. The analysis of Brazil's time series showed an increasing trend in the crude mortality rate, as well as in the rates adjusted by the Brazilian and by the world population between 2000 and 2016. Among the states, 21 of them showed a growth trend in the crude mortality rate, 16 in the mortality adjusted by the Brazilian population, and 15 in the mortality rate adjusted by the world population. Only São Paulo and Rio de Janeiro showed a decreasing trend in the mortality rate adjusted by the Brazilian and the world population.
The results of this study can contribute to the elaboration of intervention strategies and public policies to provide early diagnosis and timely treatment. New studies must be conducted to consolidate Brazilian statistics.
Kathleen Cézar de Mélo | 0000-0002-1183-0000
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Aisla Graciele Galdino dos Santos | 0000-0003-2837-0214
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
José Roberto Amorim | 0035-0057-0399-8987
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical revision of the manuscript.
Tânia Rita Moreno de Oliveira Fernandes | 0035-0002-7061-2825
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical revision of the manuscript.
Carlos Dornels Freire de Souza | 0000-0003-0837-8254
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Souza RJSP, Mattedi AP, Rezende ML, Corrêa MP, Duarte EM. An estimate of the cost of treating melanoma disease in the state of Sao Paulo – Brazil. An Bras Dermatol. 2009;84(3):237-43.
2. Bolognia JL, Jorizzo JL, Rapini RP. Dermatologia. 3rd ed. Elsevier: Rio de Janeiro; 2015.
3. Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. 6th ed. Guanabara Koogan: Rio de Janeiro; 2015.
4. Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. 7th ed. Guanabara Koogan: Rio de Janeiro; 2017.
5. World Health Organization. Global Cancer Observatory. France: Internacional Agency for Reaserch of Cancer [ acesso em 26 de junho de 2019]. Disponível em:http://gco.iarc.fr/.
6. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68(6):394-424.
7. Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019; 144(8):1941-53.
8. Castilho IG, Sousa MAA, Leite RMS. Photoexposure and risk factors for skin cancer: an evaluation of behaviors and knowledge among university students. An Bras Dermatol. 2010; 85(2):173-8.
9. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2018: Incidência de Câncer no Brasil. INCA: Rio de Janeiro; 2017.
10. Instituto Brasileiro de Geografia e Estatísticas. Censo Demográfico 2010: características da população e dos domicílios. Rio de Janeiro: IBGE, 2011[ acesso em: 26 de junho de 2019]. Disponível em: https:// censo2010. ibge.gov.br/ sinopse/ index. php?d ados =4&uf=00.
11. Organização das Nações Unidas. O trabalho como motor do desenvolvimento humano. Programa das Nações Unidas para o Desenvolvimento Humano, 2015 [ acesso em 26 de junho de 2019]. Disponível em: http:// hdr.undp.org/sites/ default/ files/ hdr15 _ove rvi ew _pt.pdf.
12. Organização das Nações Unidas. Atlas do desenvolvimento humano no Brasil 2013. Programa das Nações Unidas para o Desenvolvimento Humano, 2013 [acesso em 26 de junho de 2019]. Disponível em: http://www.atlasbrasil.org.br/2013/data/rawData/idhm-do-brasil.pdf.
13. Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000; 19(3):335-51.
14. Vazquez VL, Silva TB, Vieira MA, Oliveira AT, Lisboa MV, Andrade DA, et al. Melanoma characteristics in Brazil: demographics, treatment, and survival analysis. BMC research notes. 2015;8(1):4.
15. Garbe C, Keim U, Eigentler TK, Amaral T, Katalinic A, Holleczek B, et al. Time trends in incidence and mortality of cutaneous melanoma in Germany. J Eur Acad Dermatol Venereol. 2019;33(7):1272-80.
16. Souza SRP, Fischer FM, Souza JM. Bronzeamento e risco de melanoma cutâneo: revisão da literatura. Rev Saúde Pública. 2004; 38(4):588-98.
17. Sociedade Brasileira de Dermatologia. Data analysis of the Brazilian Society of Dermatology skin cancer prevention campaign, 1999 to 2005. An Bras Dermatol. 2006; 81(6):533-9.
18. Sena JS, Girão RJS, Carvalho SMF, Tavares RM, Fonseca FLA, Silva PBA, et al. Occupational skin cancer: Systematic review. Rev Assoc Med Bras. 2016;62(3):280-6.
19. Hammond V, Reeder AI, Gray AR, Bell ML. Are workers or their workplaces the key to occupational sun protection?.Health Promot J Austr. 2018;19(2):97-101.
20. Reeder AI, Gray A, McCool JP. Occupational sun protection: workplace culture, equipment provision and outdoor workers' characteristics. J Occup Health. 2013; 55(2);84-97.
21. Malak AT, Yildirim P, Yildiz Z, Bektas M. Effects of training about skin cancer on farmers' knowledge level and attitudes. Asian Pac J Cancer Prev. 2011;12(1):117-20.
22. Popim RC, Corrente JE, Marino JAG, Souza CA. Câncer de pele: uso de medidas preventivas e perfil demográfico de um grupo de risco na cidade de Botucatu. Ciênc saúde colet. 2008;13(4):1331-6.
23. Bezerra SMDFM, Sotto MN, Orii NM, Alves C, Duarte AJDS. Effects of long-term chronic exposure to sun radiation in immunological system of commercial fishermen in Recife, Brazil. An Bras Dermatol. 2011;86(2):222-33.
24. Arnold M, Kvaskoff M, Thuret A, Guénel P, Bray F, Soerjomataram I. Cutaneous melanoma in France in 2015 attributable to solar ultraviolet radiation and the use of sunbeds. J Eur Acad Dermatol Venereol. 2018;32(10):1681-86.
25. Parkin DM, Mesher D, Sasieni P. Cancers attributable to solar (ultraviolet) radiation exposure in the UK in 2010. Br J Cancer. 2011;105(Suppl 2):S66.
26. Olsen CM, Wilson LF, Green AC, Bain CJ, Fritschi L, Neale RE, et al. Cancers in Australia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39(5):471-6.
27. Vilanova CMA, Lages RB, Ribeiro SM, Almeida IP, Santos LG, Vieira SC. Epidemiological and histopathological profile of cutaneous melanoma at a center in northeastern Brazil from 2000 to 2010. An Bras Dermatol. 2013; 88(4):545-53.
28. Lages RB, Barbosa PB, Almeida IP, Lopes LRS, Lopes Filho LL. Detecção precoce do câncer de pele: experiência de campanha de prevenção no Piauí-Brasil. Rev Bras Promoç Saúde. 2012; 25(2):221-7.
29. Sociedade Brasileira de Dermatologia. Dezembro Laranja. [acesso em 14 de julho de 2019]. Disponível em: https://www.sbd.org.br/ dezembroLaranja/ sobre/default.aspx?a =anteriores.
30. Mendes GLQ. Melanoma no Brasil: Tendência Temporal de Mortalidade com Modelagem idade-período-coorte, e Análise de sobrevida em coorte hospitalar [tese]. Rio de Janeiro (RJ): Escola Nacional de Saúde Pública Sergio Arouca; 2014.
31. Salvio AG, Assumpção Júnior A, Segalla JGM, Panfilo BL, Nicolini H R, Didone R. One year experience of a model for melanoma continuous prevention in the city of Jaú (São Paulo), Brazil. An Bras Dermatol. 2011;86(4):669-74.
32. Schaffer JV, Rigel DS, Kopf AW, Bolognia JL. Cutaneous melanoma- past, present, and future. J Am Acad Dermatol. 2004;51(1):65-9.
33. Segalla JGM. Relatório Epidemiológico Registro Hospitalar de Câncer - Hospital Amaral Carvalho - Jaú - São Paulo: 1996-2004. São Paulo: Editora Joarte; 2005.
34. Santos ALOM, David EF, Gual F, Gonçalves FA, Lourenção LG, Cardeal ILS, et al. Melanoma cutâneo primário: estudo retrospectivo de 2000 a 2009 em um Hospital de Ensino no interior do Estado de São Paulo. Arq Ciênc Saúde. 2011;18(4):152-6.
35. Maia M, Totoli SSM. Prognóstico do Câncer de Pele. In: Neves RG, Lupi O, Talhari S. Câncer da Pele. Rio de Janeiro: Medsi; 2001.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}