


Lívia Arroyo Trídico1; Carlos Roberto Antonio2
Received on: 26/06/2019
Approved on: 20/11/2019
Financial support: None
Conflict of interests: None
Study conducted at the Medical Schooll of São José do Rio Preto, São José do Rio Preto (SP), Brazil.
Q-switched lasers are widely used in dermatology to treat one of the most common complaints of dermatological routine: the pigmented lesions. The several pigments, targets of laser treatment on the skin, have different characteristics as color, size, tissue location, and origin. Q-switched lasers can interact with the pigments in various ways. Since the emergence of Q-switched technology, different and new ways of use have emerged. Understanding the mechanisms of action involved and their main clinical applicabilities is essential to optimize the therapeutic outcomes.
Keywords: Lasers; Tattooing; Melanosis; Skin pigmentation
Quality-switched, or Q-switched, lasers gained evidence in the 1990s, a period in which several studies have demonstrated their effectiveness in targeting pigments located in the dermis, such as tattoo ink and benign pigmented skin lesions. Before the appearance of Q-switched lasers, it was believed that lasers were limited to treating lesions restricted to the surface of the skin. Thus, Q-switched lasers surprised by their ability to target dermal pigments selectively. The name Q-switched is related to the mechanism used to control the light output, since it concentrates all the energy in intense bursts or series of pulses, modulating the intracavitary losses, the so-called Q factor of the laser resonator.1
Three types of Q-switched lasers are on the order of nanoseconds but vary in wavelengths. They are Q-switched Ruby (694nm and 20ns), Q-switched Alexandrite (775nm and 50ns), and Q-switched Nd:YAG (1064nm and 5 to 15ns).2 Longer wavelengths are better for treating lesions in the dermis due to higher penetration capacity and less epidermal absorption. Pigmented lesions of the epidermis respond better to shorter wavelengths. Thus, the indications for treatment with Q-switched lasers are diverse: ephelides, café-au-lait spots, lentigo, nevus of Ota, melasma, tattoos, among others.3
The treatment of pigmented targets with laser involves the selective destruction of a given structure. Thus, according to the theory of selective photodermolysis, two conditions are necessary: the laser must have a wavelength that is highly absorbed by the target regarding the surrounding healthy tissue, and the pulse duration used must be shorter than the time it takes for heat to escape through conduction. Thus, Q-switched lasers are classified as pulsed lasers with short pulses in nanoseconds. Pulsed lasers seek to destroy a specific structure, differing from continuous-wave lasers in which the objective of the treatment is to reach the entire surface tissue, providing a constant flow of light measured in watts. Also, other types of pulsed lasers act on pigmented targets: the pulsed dye laser acts on hemoglobin and long pulse lasers (Nd:YAG, alexandrite, and diode) act on hair removal.1, 3
The various target pigments for laser treatment on the skin have different characteristics in terms of color, size, location in the tissue, and origin. Thus, Q-switched lasers have several ways to interact with pigments. This study seeks to clarify and differentiate the several ways of using Q-switched lasers.
The theory of selective photodermolysis is the primary principle for destroying pigments with minimal damage to the underlying tissue. It is based on delivering enough energy to the target, but with pulse duration shorter than the thermal relaxation time of the target tissue, that is, the time it takes for the heated chromophore to dissipate half the heat absorbed into the underlying tissue. That way it is possible to reach the target, preserving the structures around it.4
The pulse duration of Q-switched lasers is so short that extremely small pigments from 10 to 100 nm are heated until they fragment, but before their heat is dissipated to the surrounding skin, preventing tissue heating, which could lead to burns or scars. The main mechanisms of pigment destruction with the Q-switched laser are by shock waves and/or cavitation damage, which are photomechanical physical effects produced by thermal expansion and/or extreme temperature gradients created within melanosomes or tattoo pigments.4
After the fragmentation of the pigment particles, phagocytosis performed by macrophages is the primary method of elimination. Tissue macrophages direct the broken fragments to the lymph channels or regional lymph nodes. Some fragments can be taken off transepidermically as the post-treatment scab is removed.5
Different pigments require different wavelengths; for example, green tattoo pigments are absorbed by alexandrite and ruby lasers, while 532nm lasers act only in the treatment of pigmented lesions located on the epidermis. The laser must penetrate the skin deep enough to reach the target and must be highly absorbed by the pigment. More superficial pigments are better treated with a shorter wavelength, while longer wavelengths act more deeply. 4
In addition to the wavelength variation, Q-switched lasers vary in pulse duration and fluency, characteristics that are fundamental in understanding their clinical applicability.
As initially reported, all Q-switched lasers have a pulse-width of the order of nanosecond, that is, they are short-pulse. However, there is a variation in the duration of short nanosecond pulses. This variation brings with it different therapeutic results and clinical indications. They are:
Short pulse Q-switched laser
Extremely short pulse Q-switched laser
The differentiation of the extremely short-pulse Q-switched concerning the short-pulse Q-switched emerged recently after the development of new devices capable of generating extremely high peaks that vary in megawatts but have pulses even smaller than the first devices of Q-switched laser.3,6 Few laser systems are capable of generating unique pulses too high. Many devices require two or more pulses to reach pulses as high as the extremely short pulse Q-switched laser.6,7
Extremely short Q-switched devices escape the phenomenon of optical shielding, which induces the formation of a plasma in the skin when the laser reaches the pigment, making multiple pulses of energy unable to effectively treat the deeper layers of pigment. Thus, a single shorter and higher pulse can achieve greater pigment extension, enhancing the effect of the session. Cencic et al., 2010, compared a single extremely short pulse Q-switched laser with multiple short-pulse Q-switched laser and concluded that the extremely short-pulse Q-switched laser is capable of increasing energy delivery, generating an even greater photoacoustic effect that breaks more pigment and to a greater extent compared to shorter, multiple pulses that cannot reach all of the pigment due to the optical shielding phenomenon.3,7,8
In extremely short pulses, there is greater homogeneity of the laser beam. They are mainly used to treat tattoos to minimize epidermal damage, as well as reduce bleeding and changes in skin texture.6 They can also be used for other pigmented lesions, such as ephelides and nevi of Ota, acting on pigments located in the dermis and epidermis. The maximum fluency achieved is 15J/cm2 at 1064nm, and generally, the number of sessions required for therapeutic effectiveness is better with the use of the extremely short pulse Q-switched laser.3
The mechanism of action of the Q-switched Nd:YAG laser (short pulse, nanoseconds) is different from the Nd:YAG long pulse (milliseconds). However, we know that, in the case of the long pulse, the laser energy dissipates as it heats the areas around the applied beam, and this heat can stimulate collagen impacting in the treatment of rhytids and photodamage.9 In contrast, in the case of Q-switched laser (nanoseconds), the energy does not have time to be dissipated to the adjacent tissue and concentrates on the target (pigment).
Q-switched pulses with energy above 5J/cm2 cause a thermolytic effect when the target pigment explodes, which brings shock waves to the surrounding tissues. Thus, the skin suffers physical and not thermal damage. This physical damage can lead to the expression of collagen III and consequent skin rejuvenation. Currently, it is known that when the Q-switched Nd:YAG laser is performed with energy below 5mJ/cm2, that is, below the thermolytic effect, therapeutic effects can also occur on aged skin since pigments still absorb the laser without the ability to cause shock waves of the thermolytic effect, thus characterizing the subthermolytic Q-switched laser.10,11
In general, the effects seen in thermolytic treatments are similar to traditional ablative lasers (Er:YAG and CO2) with fewer adverse events. Using subthermolytic fluencies, the effects of collagen stimulation are less pronounced; however, there is a total absence of downtime (present in ablative and thermolytic modalities).11 Therefore, the subthermolytic Q-switched Nd:YAG laser could act at a "subcellular" level, since it breaks only pigments and not cells, being called "subcellular selective thermolysis".12,13 The mechanism of action of subcellular selective thermolysis is also believed to involve biostimulation. 12,13
Lukac et al., 2010, and Liu et al., 2008, have shown that low fluency (subthermolytic) Q-switched laser therapy is safe and effective in melasma.14,15 A bleaching of 50% in epidermal melasma and of 30% to 50% in dermal or mixed melasma can be expected with the use of low fluence Q-switched laser.12 Jeong et al., 2010, reported that, with the use of subthermolytic Q-switched laser (1.6J/ cm2 fluence, 7mm tip, eight sessions with weekly intervals) associated with the daily triple formula, there was a more significant improvement in melasma in patients treated with laser than with the formula alone. 16
Subthermolytic Q-switched laser therapy is also used safely and effectively to rejuvenate photoaged skin, although the results are not as evident as the results obtained with ablative lasers. A study that treated patients with four or more sessions and used fluencies ranging from 1.5 J/cm2 to 3.5 J/cm2 showed an improvement of 20% to 35% in pore reduction, skin tone, and skin texture.12 Kalil et al., 2016, assessed the results of four sessions of 1064nm Q-switched Nd:YAG laser in stimulating facial skin collagen of four patients who obtained improvement in wrinkles, pores, and skin firmness (7 mm tip; 5Hz frequency; energy used in the first session was 600 mJ, increasing to 900 mJ in the second session, and to 1200 mJ in the third and fourth sessions).17
We know that in the treatment with Q-switched laser to remove pigments, the pulse duration is less than the thermal relaxation time of the pigment. Therefore, what is called a "lock-in" effect occurs, that is, the structure is heated in such a short time that the temperature increases without dispersing the heat, "locking" it inside the pigment. When a particle is heated in an extremely short time, the stress generated within it does not have enough time to spread. Therefore, "locked-in stress" occurs and, if it is high enough, it causes the fragmentation of the pigment particle.18,19 It is believed that the time limit for that "locked-in stress" occurs is slightly less than 1 nanosecond.
Thus, according to Kasai, 2016, when a Q-switched laser is used, its main reaction is photodermolysis, with a slight photomechanical effect. However, when a picosecond laser is used, photoacoustic destruction of the particle occurs on a larger scale, characterizing the locked-in stress with less photothermal effect, which causes more destruction to the target particles.2 Thus, what happens with picosecond lasers is that the pigment particles are broken down in even smaller sizes than with nanosecond lasers, by merely by increasing the photomechanical effect and reducing the photothermal effect. 20
Given the reduction of pulses from nanoseconds to picoseconds, the emergence of picosecond lasers allowed the more efficient and effective destruction of pigment particles, also presenting fewer adverse events.2 However, given the recent emergence of this technology, some questions still need to be clarified.
Although it is theoretically known that picosecond lasers are more effective at breaking pigments than nanosecond lasers, it is not known exactly which pulse range is best for removing pigments. Another issue about picosecond lasers is color dependence: because they act more strongly on the photoacoustic effect, picosecond lasers were thought to act on the removal of pigments regardless of the particle color. However, in current practice, although they present less color dependency than nanosecond lasers, this dependency still exists.21 Moreover, the high cost associated with the picosecond laser is a limiting factor for the clinical practice.22
Choi et al., 2018, compared nanosecond and picosecond lasers in removing tattoo pigments in an animal model. Q-switched Nd:YAG and picoseconds Nd:YAG lasers were assessed, showing greater effectiveness of the picosecond laser, with fewer adverse events, in addition to the ability to remove some non-black pigments.22
Zhang et al., 2018, compared the picosecond Alexandrite laser to the nanosecond Nd:YAG laser for removing a bluish-black tattoo performed more than 10 years ago on the eyelids of 72 patients. One to four sessions were performed, and there was no significant difference in results between the two types of lasers.23
Vachiramon et al., 2018, compared nanoseconds Nd:YAG 532nm to picoseconds Nd:YAG 532nm to treat solar lentigo. Thirty lesions were randomized and treated with a single session. In the evaluation at six and 12 weeks after the beginning of the sessions, the two treatments cleared the lesions. However, the patients were more satisfied with the lesions treated with a picosecond laser. Adverse events were similar in both groups. The authors concluded that the two lasers are safe and effective in the treatment of solar lentigo. However, due to the benefit-cost ratio, the nanosecond laser remains the primary treatment, and the picosecond laser can be considered a therapeutic option.24
Therefore, more studies are needed to define the main therapeutic differences and better indications between the use of nanosecond and picosecond laser when addressing pigment treatment.
Ephelides, solar lentigines, and seborrheic keratoses can be treated effectively with Q-switched lasers. The healing time and adverse events profile between these lasers are similar. Still, the absence of purpura following treatment with Q-switched Ruby (694 nm) and Alexandrite (75 5nm) makes them slightly preferred, especially when it comes to facial lesions. One or two treatment sessions are usually sufficient to clear most lentigines, although longer treatments are occasionally required for resistant and more extensive lesions. The biggest concerns of treatment are the postoperative pigment changes, such as hypopigmentation and hyperpigmentation. Post-inflammatory hyperpigmentation is more frequent in individuals with Fitzpatrick skin phototype III and IV, as well as in individuals with tanned skin. The risk of hypopigmentation is higher with the Q-switched Ruby laser than with the Q-switched Alexandrite laser or the Q-switched Nd:YAG 1064nm laser. Regarding café-au-lait spots, whitening is achieved after repeated sessions of Q-switched laser, because, as the treatment progresses, the color uniformity is interrupted, and the stain starts to show a speckled pattern with small macules until it clears completely.25
Until the development of short pulse lasers, there was no effective treatment for dermal melanocytosis such as nevus of Ota, nevus of Ito, and Mongolian spot.
Q-switched laser therapy has become the treatment of choice for these types of pigmented lesions. Q-switched ruby, alexandrite, and Nd:YAG lasers can reach dendritic melanocytic cells in the dermis, producing significant or complete lesion whitening after an average of four to eight sessions. Becker's nevi show variable results with Q-switched lasers, since hypopigmentation, incomplete removal, and recurrence often occur. Although nevus pigment cells are disorganized after exposure to the Q-switched laser, a significant amount of pigment persists in the attached structures. The reasons for this inadequate response and high recurrence rate are probably related to the complex hamartomatous nature of Becker's nevi and their hormonal dependencies, demonstrated by the increased activity of their androgen receptors. Therefore, the best approach in treating these lesions is the combination of a Q-switched laser and a long pulse laser, specific to the pigment, to simultaneously remove the epidermal pigmentation and the hair of the lesion.25
In the case of melasma, low fluence Q-switched laser therapy (subthermolytic) brings effective results. In epidermal melasma, higher whitening rates are observed than in dermal or mixed melasma.12 The absence of complete clearing of melasma is probably related to the failure to control the basic pathophysiological mechanisms of hypermelanosis, such as genetic influence, exposure to the sun, and hormonal factors.
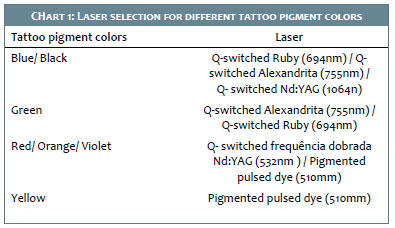
Laser tattoo treatment depends on the type and content of pigment. Amateur tattoos require fewer treatment sessions because they are usually made up of a single carbon-based pigment. Professional tattoos are more resistant to laser treatment because they are more densely pigmented and can contain multiple and less receptive pigments, mainly yellow and dark green. The ideal wavelength should be considered according to the colors present in the tattoos, since the affinity of the different pigments varies according to the wavelengths used, as shown in chart 1.5,25
Low fluence Q-switched lasers in multiple passes are used for facial rejuvenation to stimulate dermal fibroblasts to perform neocollagenesis providing improvement in skin tone and texture, pore reduction, sebaceous secretion, rhytids, and dyschromias.17 Goldberg conducted a pioneering pilot study describing the use of the Q-switched Nd:YAG 1064nm laser to treat facial rhytids, observing an improvement in texture, cutaneous elasticity, and rhytids after three monthly treatments. In a histological analysis in six patients treated with a Q-switched Nd:YAG laser, there was an improvement in solar elastosis, organization of collagen fibers, as well as an increase in the thickness of the papillary dermis.26,27
Q-switched lasers are widely used in dermatology to treat one of the most common complaints of the dermatological routine: pigmented lesions. Thus, since its emergence, discoveries and different forms of use are continually growing. To optimize the use of this technology, it is essential to understand the mechanisms of action involved and their main clinical applications.
Lívia Arroyo Trídico | 0000-0002-7743-4195
Study design and planning; preparation and writing of the manuscript; critical literature review.
Carlos Roberto Antonio | 0000-0001-9243-8293
Study design and planning; critical literature review; critical revision of the manuscript.
1. Kasai K. Tattoo. Introduction to Q switched laser treatment. Bunkodo. 2008;86-97.
2. Kasai K. Picosecond Laser Treatment for Tattoos and Benign Cutaneous Pigmented Lesions (Secondary publication). Laser Ther. 2017;26(4):274-81.
3. Goel A. Clinical applications of Q-switched NdYAG laser. Indian J Dermatol Venereol Leprol. 2008;74(6):682-6.
4. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220(4596):524-7.
5. Barua S. Laser-tissue interaction in tattoo removal by q-switched lasers. J Cutan Aesthet Surg. 2015;8(1):5-8.
6. Kozarev J. Fotona QX MAX: A versatile and powerful device for the treatment of pigment - Aesthetic Trends & Technologies, 2010.
7. Cencic B, Lukac M, Marincek M, Vizintin Z. High Fluence, High Beam Quality Q-Switched Nd:YAG Laser with Optoflex Delivery System for Treating Benign Pigmented Lesions and Tattoos. J Laser Health Academy. 2010;(1):9-18.
8. Aesthetic Buyers Guide: "RevLite EO Q-switched Nd:YAG Laser Features PhotoAcoustic Therapy Pulse";2007. p26.
9. Liu H, Dang Y, Wang Z, Chai X, Ren Q. Laser induced collagen remodeling: A comparative study in vivo on mouse model. Lasers Surg Med. 2008;40(1):13-9.
10. Chan NPY, Ho SGY, Shek SYN, Yeung CK, Chan HH. A case series of facial depigmentation associated with low fluence Q-switched 1,064-nm Nd:YAG laser for skin rejuvenation and melasma. Lasers Surg Med. 2010;42(8):712- 19.
11. Bevec T, Lukac M. Clinical Results in Thermolytic and Sub-Thermolytic Q-Switched Nd:YAG Skin Rejuvenation J Laser and Health Academy. 2011; (1).
12. Bevec T. Treating Melasma with Sub-Thermolytic Q-Switched Nd:YAG. J Laser and Health Academy. 2011; (1).
13. Polnikorn N. Treatment of refractory dermal melasma with the MedLite C6 Q-switched Nd:YAG laser: Two case reports. J Cosmet Laser Ther. 2008;10(3):167-73.
14. Liu H, Dang Y, Wang Z, Chai X, Ren Q. Laser induced collagen remodeling: A comparative study in vivo on mouse model. Lasers Surg Med. 2008;40(1):13-9.
15. Lukac M, Sult T, Zabkar J, Gorjan M, Vizintin Z. Parameters for the New FRAC3 Nd:YAG Laser Skin Treatment Modality. J Laser Health Academy. 2010;2010(1):47-55.
16. Jeong SY, Shin JB, Yeo UC, Kim WS, Kim IH. Low-fluence Q-switched neodymium-doped yttrium aluminum garnet laser for melasma with pre- or post-treatment triple combination cream. Dermatol Surg. 2010;36(6):909-18.
17. Kalil CL, Campos V, Reinehr CPH, Chaves CRP. Laser toning and drug delivery: a pilot study using laser Q-switched laser 1064nm. Surg Cosmet Dermatol. 2016;8(2):142-6.
18. Kasai K. Danger of low fluence Q switched Nd:YAG laser treatment for melasma-so called "laser toning". J Japan Soc Laser Surg Med. 2016;36(4):430-5.
19. Kasai K. Melasma. In: Kasai K, editors. Treatment of Pigmented Lesions. Hongo Bunkyo-ku: Bunkodo; 2015. p. 121-72.
20. Saedi N, Metelitsa A, Petrell K, Arndt KA, Dover JS. Treatment of Tattoos With a Picosecond Alexandrite Laser: A Prospective Trial. Arch Dermatol. 2012:148(12):1360-3.
21. Kasai K. Treatment strategy of melasma: The importance of conservative treatment taking into consideration of the essential qualities of melasma. Pepars. 2016;110:73-8.
22. Choi MS, Seo HS, Kim JG, Choe SJ, Park BC, Kim MH, et al. Effects of picosecond laser on the multi-colored tattoo removal using Hartley guinea pig: A preliminary study. PLoS One. 2018;13(9):E0203370.
23. Zhang M, Huang Y, Lin T, Wu Q. Comparison of treatment with an Alexandrite picosecond laser and Nd:YAG nanosecond laser for removing blue-black Chinese eyeliner tattoos. J Cosmet Laser Ther. 2018;20(7-8):415-8.
24. Vachiramon V, Iamsumang W, Triyangkulsri K. Q-switched double frequency Nd:YAG 532-nm nanosecond laser vs. double frequency Nd:YAG 532-nm picosecond laser for the treatment of solar lentigines in Asians. Lasers Med Sci. 2018;33(9):1941-7.
25. Antonio CR. Laser: Princípios básicos e avançados. Ipele: Livro Online, Set 2018;Cap 60
26. Goldberg DJ, Whitworth J. Laser skin resurfacing with the Q-switched Nd:YAG laser. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 1997;23(10):903-7
27. Goldberg DJ, Silapunt S. Histologic evaluation of a Q-switched Nd:YAG laser in the nonablative treatment of wrinkles. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2001;27(8):744-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}