


Bruna Paninson1; Caroline Brandão2; Marcia Ramos-E-Silva2
Received on: 11/07/2019
Approved on: 16/10/2019
Financial support: None
Conflict of interests: None
Study conducted at the Dermatology Service and Postgraduate course at Hospital Universitário Clementino Fraga Filho, Universidade Federal do Rio de Janeiro HUCFF/UFRJ , and Medical School of the Universidade Federal do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
The responsibility of the dermatologist continues after the end of a dermatologic surgery and must be shared with the patient. That is why the guidelines on postoperative care necessary with wounds are critical and need to be passed on clearly, at the patient's understanding level, and reinforced in writing. Good communication with patients helps the surgeon to avoid complications. The authors' concern to standardize the postoperative guidelines in dermatologic surgery originated the development of this article. A literature review, with the authors' main inquiries, was organized in questions and answers form, to assist dermatologists when performing surgical procedures.
Keywords: Postoperative care; Bandages; Postoperative complications
Dermatologic surgery is a standard procedure in the dermatologist's daily routine. It is considered safe and with low risk of complications; however, even experienced dermatologic surgeons are subject to complications during their professional practice. Therefore, prevention is always preferable to treatment. Proper planning, meticulous technique, and good communication with the patient are necessary.
The ideal scenario is to provide patients with written postoperative guidelines as well as to use the telephone for emergency communication. Postoperative calls to assess patient status are an easy way to detect complications early, increasing patient satisfaction. Facing these challenges, we created a set of questions whose answers can help standardize the conversation with the patient in the postoperative period. Most of the guidelines found in the literature are based on studies of other medical specialties, such as thoracic and cardiac surgery, as well as nursing studies. Thus, it is also necessary to compile the information according to the setting of dermatologic surgery.
This article is a narrative literature review, which aims to standardize the necessary guidelines for the patient after their dermatologic surgery. The recommendations are organized in the form of questions and answers. The authors asked 10 pertinent questions about the main guidelines that patients should receive after the end of dermatologic surgery, and the answers were elaborated through an analysis of the literature, books, printed and/or electronic articles.
After surgery and as soon as the wound is adequately covered, the patient or their caregiver is responsible for wound care at home. So, he/she should receive detailed information, preferably in writing, on how to take care of his/her surgical wound.
The health professional (doctor or nurse) performs the first simple compressive dressing that must remain intact for 24 to 48 hours, with a thin layer of ointment (petroleum jelly, petrolatum) and a non-adherent gauze, cut to cover the dimensions of the suture line. An absorbent layer of gauze should be placed, fixed by an external layer of surgical tape.1 The occlusive ointment must be reapplied and, depending on the location of the wound and the level of activity of the patient, it is advisable to place a light dressing or bandage, if necessary.1
At the end of the surgery procedure, a cover is placed over the wound, to prevent bacteria from entering the suture site, in addition to physically supporting the wound and absorbing exudates. This coverage is, in general, removed the next day,2 and a new one is performed. Because it aims to absorb exudates, among other actions, the dressing should be maintained as long as bleeding and/or drainage of secretion remains.2,3
The exact time that the surgical dressing should remain on the wound is still controversial both in the literature and in clinical practice. The dressing serves as a barrier for exogenous microorganisms, as long as its outer surface remains dry. When it becomes wet, it loses its protective capacity.2,3
During the first 24 hours, neutrophils appear at the edges of the surgical wound, targeting the formed fibrin clot. The edges become thick, and, in 24 to 48 hours, the epithelial cells of the edges migrate and grow along with the dermis and below the superficial crust, merging in the midline. Thus, we have physiological evidence that the wound is sealed from the external environment. The need for the dressing to remain beyond 12 to 24 hours has long been questioned. Today it is known that there is no increased risk of infection of the surgical site in this period, even if the surgical wound is exposed.2
The early removal of the dressing allows easy examination of the wound and early detection of complications, in addition to reducing the spending on dressing changes, also allowing patients to perform their daily hygiene practices. These guidelines are valid for surgical wounds considered clean and with closure by primary intention.2,3
The patient's desire must also be considered, as many of them feel safer when their surgical wounds remain occluded. Therefore, it is recommended to place gauze over the suture line and tape at the edges, leaving the center without occlusion. For many patients, this behavior improves their self-esteem.2
If the patient desires to keep the dressing, he/she should change it daily. In case the surgical wound remains with no exudation, there is no need to keep the dressing, but only to clean it with running water and mild soap foam during the bath.4
Facing a surgical site with serous and/or serosanguineous drainage, the patient must wash with it saline, as many times as necessary, until the drainage is interrupted, and keep the occlusive dressing. Dressing with sterile gauze and a minimum of adhesive tape is recommended to prevent fluid from staining bedding and patient clothing.2 Keep it minimally moist, with petrolatum or petroleum jelly, for better healing. This advice is also valid for patients who wish to maintain their surgical wounds without occlusion with dressings.1,3
If the patient remains with the dressing, he/she should repeat it two to three times a day, depending on the amount of transudate from the wound, until the suture removal. Bathe the dressing site can be useful to remove it in cases of adhesion or large edema in the area. The new dressing must be non-adherent, absorbent, protective, and safe.5
Patients should be instructed to remove the dressing in 24 to 48 hours and clean the wound with water and mild soap or with saline. There is no need to use other substances.1
Detergents, hydrogen peroxide, and concentrated povidone-iodine solutions should be avoided due to tissue damage and direct toxicity.6 Hydrogen peroxide can be used, but in moderation and to remove dried blood or scabs, as its excessive use can impair wound healing, by irritating the tissues.5
Chlorhexidine and alcohol 70% are indicated for cleaning intact skin. Still, they can cause hypersensitivity, cytotoxicity of fibroblasts and neutrophils with decreased chemotaxis, increased inflammation, damage to endothelial cells, delayed wound contraction and delayed healing if used on the surgical wound (open).5,6 The alcohol 70% can cause skin dryness, even on intact skin, if used repeatedly.7
Patients should be instructed on how to modify their routines, starting with the bath, usually 24 hours after surgery, avoiding wetting the dressing. Thus, they should avoid any activity in which the wound can be submerged (bathing, swimming), as immersion can increase the risk of infection and wound dehiscence.5 Some more recent waterproof occlusive dressings allow the patient to bathe in the first 24 hours, such as hydrogel and transparent polyurethane films.5
Physical activity should be avoided for at least 24 to 48 hours after surgery, as stress on the wound can cause dehiscence. Each case should be evaluated, according to the age and level of physical activity of each patient, as well as the characteristics of the surgical wound, such as extension, location, and depth, for greater restrictions.5
Everyone should be guided and encouraged to stop smoking, but if this is impossible, it should be minimized to less than 1 pack/day for one week before and for up to four weeks after surgery. Tobacco is a crucial inhibitor of wound healing and a significant cause of graft failure. Thus, it should be emphasized to the patient directly that smoking causes vasoconstriction, inhibits the wound epithelization, reduces the oxygen levels in the wound bed, and inhibits the deposition of collagen, affecting the healing phases.5
Social alcoholic patients should be instructed to discontinue alcohol consumption 48 hours before surgery, due to the interference of alcohol with the anesthetic and possible increase in local pain during surgery.5,8 In alcoholics, the abrupt suspension is not recommended due to the risk of severe symptoms after withdrawal.9
Strenuous activities, such as in particular weight lifting and vigorous exercise, as well as recreations, should be suspended for 24 to 48 hours.8 The peculiarities of each patient should be assessed, considering age, preoperative activity level, and extent, location, and depth of the wound.5
Although controversial, the early removal of the suture reduces the possibility of marks on the skin, improving the aesthetic result.
The sutures must remain on the scar as short as possible and must be maintained only long enough to allow complete epithelialization along the wound edges.1,8 In younger, healthy, and non-smoking patients, the sutures can be removed early, compared to older patients, smokers or diabetics, due to the slow wound healing.1
Before removing the sutures, the mechanical removal of the scabs, with the aid of hydrogen peroxide or saline, helps to visualize the stitches. The permanence of the stitches varies with the anatomical location according to the guidelines below:1,8,10
- Eyelids: two to four days;
- Face: up to seven days;
- Neck: two to seven days;
- Scalp: seven to 10 days;
- Trunk and extremities: 10 to 14 days;
- Over the joints: up to 10 days;
- Oral and genitoanal mucosa: three to five days.
After the removal, additional protection must be maintained, because healing is not yet complete at this time. Some authors suggest the use of micropore adhesive tapes to maintain the appropriate tension, keeping them from six weeks to six months, depending on the location, to reduce edema and minimize scarring.1
Aiming to modulate and even reduce post-surgical scarring, some studies indicate the injectable use of botulinum toxin type A (BTA) safely and effectively. In recent years, this practice has been described for hypertrophic scars and questioned for use in post-surgical scars. The main factor for the final appearance of the scar is the tension between the edges. The tension exacerbates the inflammatory reaction and leads to increased fibrosis by prolonging the wound erythema. The early BTA injection improves the aesthetic aspect of the surgical wound, as it acts by decreasing tension, directly inhibiting the activation of fibroblasts and TGF-beta1, suppressing the enlargement of the scar, reducing erythema, and effectively reducing the incision line.11
Preoperative assessment of patients, their history of clotting and diseases, as well as their medications in use are essential to prevent bleeding and bruising.9,12
The use of anticoagulants and systemic arterial hypertension increase the risk of bleeding, as well as alcoholism, as it inhibits the qualitative activity of platelets, leading to greater bleeding.12
Nonsteroidal anti-inflammatory drugs (NSAIDs) should be discontinued three to five days before surgery and reintroduced after three to seven days.13 Gingko biloba, vitamin E, garlic, ginger, glucosamine sulfate, and chondroitin may also increase the risk of intra- and postoperative bleeding and should, therefore, be stopped seven days before surgery.12,13 Capsaicin may decrease the concentration of factor VIII and, despite inconsistent information in the literature, discontinuation of medication two weeks before surgery with reintroduction after two weeks should be indicated.13
More recent studies emphasize that there are no statistical differences in the risk of postoperative bleeding in patients using ASA, warfarin, NSAIDs and the control group.14,15 It is not necessary to suspend anticoagulants and antiplatelet agents to perform dermatologic surgery. ASA does not increase the risk of major bleeding, unless the bleeding time is extended, which happens in only 25% of patients using this medication.16
For small procedures, the risk of bleeding is minimal.17 Bleeding time determination is necessary to assess risk in larger procedures.9 For patients using ASA for analgesic/ anti-inflammatory purposes or primary prevention, the advice is to discontinue the drug 10 to 14 days before the procedure. Patients using it for secondary prevention should continue to use it due to cardioembolic risk.13,17
Despite the increased risk of perioperative bleeding with vitamin K antagonists (warfarin), its suspension is not necessary, as bleeding can be controlled during surgery.12 The risk of thrombotic events with medication discontinuation is 1 in 278 to 1 in 11,500.12 Thus, the thromboembolic cardiovascular risk is higher than the benefit of drug withdrawal.13,18
Other medications, such as unfractionated heparin, thienopyridines (clopidogrel, ticlopidine, and prasugrel), thrombin inhibitors (lepirudin, argatroban, dabigatran), indirect factor Xa inhibitors (fondaparinux), phosphodiesterase inhibitors (dipyridamole), should not be suspended.13 Direct factor Xa inhibitors (rivaroxaban) need further studies to be evaluated. The orientation is to wait for the end of treatment to perform the dermatologic surgical procedure.13
Bleeding can cause several problems for both the patient and the surgeon. During the procedure, the bleeding covers the surgery site and, therefore, it is essential to keep the field dry for visualization and for later prevention of bruising. Hemostasis is a fundamental part of the surgery and should be performed with an electric scalpel. Attention should be paid throughout the wound, including the detached edges, searching for bleeding vessels.
There is the option of special dressings with hemostatic materials that can be used on open wounds to contain the bleeding. Examples of these products are absorbable gelatin or powder sponges, microfibrillar collagen, topical thrombin to accelerate coagulation, and oxidized cellulose. For major intraoperative bleeding, the Penrose drain placement is indicated to assist in hemostasis and decrease infection rates.16
In the postoperative period, a bandage composed of absorbent gauze in large quantities and resistant tape helps to compress the wound. Local ice application also reduces the bleeding. Patients should be advised to limit their activities by restricting the elevation of the operated site and avoid lifting weights higher than 4 kg to 7 kg.16
Patients should be informed and advised about the appearance of edema and post-surgical discomfort. During the first 48 hours, the first alteration is local discomfort, which should be treated with a common pain reliever (paracetamol and dipyrone, medications commonly used in Brazil). Ingestion of alcohol, ASA, and any substance containing aspirin, in addition to NSAIDs (including ibuprofen), should be avoided, as they increase the likelihood of accidental bleeding in the postoperative period. The doctor should reassess the patient if the discomfort remains.16
Postoperative pain compromises the patient's general condition. It is more intense in the first 24 to 36 hours, improving after 48 hours. We should not underestimate the patient's pain, as it is subjective and its threshold is immeasurable.19
Postoperative complications are considered uncommon, but must be explained to the patient at the time of signing the informed consent form.16
Guiding the patient is essential to avoid postoperative complications. The patient may present edema, ecchymosis, erythema, and increased skin sensitivity – they are all considered normal and expected changes.16
The four most frequent complications are bruising, infection, wound dehiscence, and necrosis.16
The bruising is a collection of blood at the surgery site that leads to edema and pain at the site with a progressive increase as it expands. The drainage of fluid collections is mandatory, since they interfere with wound healing, favor local infection, and can lead to necrosis.16
The use of antibiotics, when there are signs of infection, is indicated after drainage, and the class of antibiotic to be chosen depends on the location of the wound, with the first generation cephalosporin (cephalexin) considered the first line of treatment.16
Ecchymosis can be alarming for the patient, but it rarely implies a problem other than aesthetics. Ecchymosis masking a bruising should be ruled out through physical examination. It is prevalent around the eyes - even if the surgery has not been performed on the eyelids - in patients with coagulopathies, anticoagulant users, and elderly. All patients should be instructed on the possible appearance of ecchymosis and apply ice to the site during the immediate postoperative period to decrease their formation.16
The surgical wound dehiscence is the spontaneous opening of the sutures with the separation of all its layers. When there is detachment and/or loss of the superficial skin layer, the epidermis, around the surgical wound, it is called post-surgical epidermolysis. Both are consequences of other complications: hematoma, seroma, infection, necrosis, inadequate repair design and/or early suture removal, and situations such as old age, diabetes, neoplasms, poor nutritional conditions, drugs (corticosteroids and certain antibiotics), and smoking, among others. When dehiscence occurs, the option is healing by secondary intention If there are no signs of infection when detected in the first 24 hours, a new closure can be performed, with the wound edges friable.16
Necrosis occurs when vascular perfusion is compromised and is usually the result of another complication. Closing the lesion under tension can affect the superficial dermal plexus, impairing blood perfusion and causing pallor in the tissue. Another cause is the extensive detachment in an excessively superficial plane, interrupting the arterioles that make the local irrigation. The use of suitable materials, such as a hook instead of tweezers, to lift the tissue instead of crushing it, prevents tissue damage by crushing. The layered suture helps eliminate tension in the tissue. The suture knot must be secure and not tight, so as not to compromise the blood supply.16
Another complication that can occur is seroma, a collection of serous fluid accumulated in potential spaces after surgery, very common after large divisions. Layered closure eliminates this space. Seroma is identified as a soft mass below or adjacent to the suture line. It must be drained, as this fluid makes healing difficult, increases the possibility of infection and applies pressure to the healing epidermis.16
Patients should be advised about long-term complications, such as paresthesia, pain, motor impairment depending on the location, pruritus, erythema, and skin pigmentation alteration, which can occur at the surgical wound site for several months after the procedure.16
The rate of wound infection is very low (0.91% to 1.3%), if the surgical technique is clean.13,20
The risk of infection is reduced if the patient takes a bath before surgery, so he/she should be instructed to do so the night before surgery with an antiseptic agent. Shaving should be avoided 24 hours before, but if necessary, it is recommended to trim the hair with scissors or a hair clipper in the operating room.13,21 Haircut is a better alternative than razor shaving.18
Among the risk factors for surgical site infection are the location of the procedure below the knee, on the lips, ears, and groins, as well as smoking, immunosuppression (including diabetes), and colonization.13 Another interesting finding is a higher rate of infection in malignant than benign tumor lesions.20
Pre- and postoperative antibiotics increase the cost and bacterial resistance. They are indicated as prophylaxis in flaps or nose and ear grafts, closure under tension, inflammation or infection of the surgical site, procedures below the knees, surgery on the hands, uncontrolled diabetes mellitus, and immunodeficiency.13
Antibiotic prophylaxis should be performed 30 to 60 minutes before surgery. Sulphamethoxazole-trimethoprim 800/160 mg, ciprofloxacin 500 mg, levofloxacin 500 mg orally, or intravenous use of cephalothin 1g are recommended.13
Topical antibiotics do not prevent wound infection, so they should not be used for this purpose, in addition to increasing the risk of bacterial resistance and contact dermatitis.13
Some recent studies have found that bacterial decolonization with topical mupirocin is useful for patients with nasal Staphylococcus aureus, reducing the rates of surgical site infections.13
Each patient must be evaluated individually and monitored according to the type, extent, and location of the surgical wound. If there is a complication, the follow-up time can be extended until the complete resolution of the complication. Each professional must evaluate the time required for each patient.
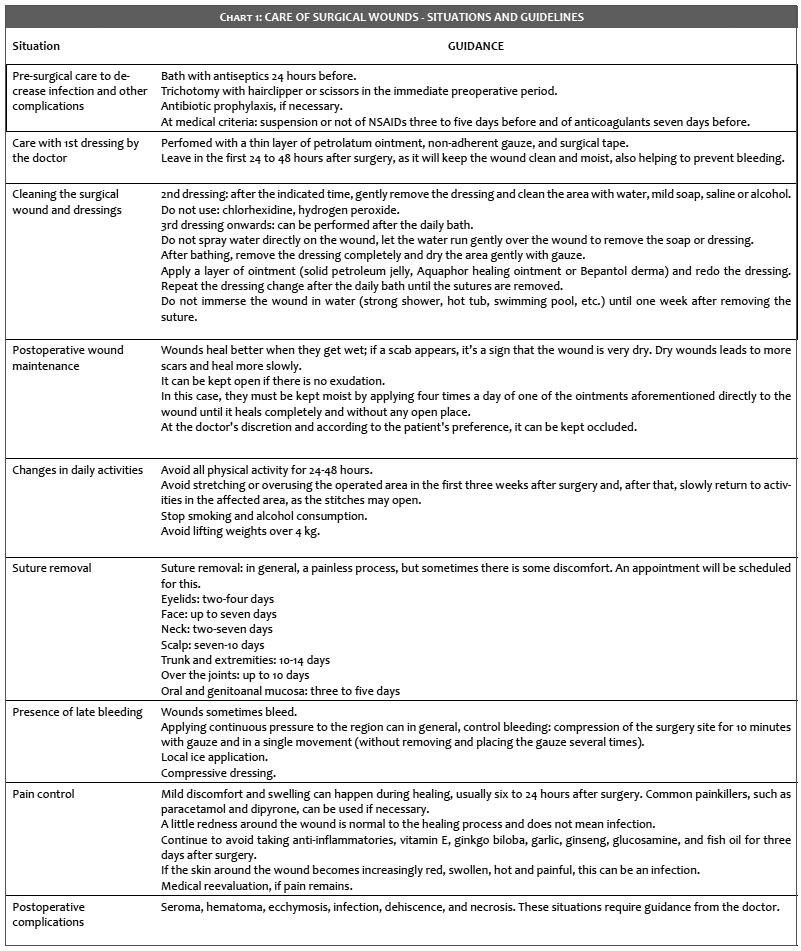
This article was created to facilitate the daily routine of dermatologic surgeons and to demystify some old practices, already updated in the literature. The authors' main objective was to provide concise information on postoperative care, summarized in the Chart 1 below.
Bruna Paninson | 0000-0001-9163-3265
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Caroline Brandão | 0000-0002-1955-4551
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marcia Ramos-E-Silva | 0000-0003-1625-0760
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Poblete-Lopes C. Cirurgia excisional básica. In: Vidimos AT, Ammirati CT, Poblete-Lopez C. Requisitos em Dermatologia: Dermatologia cirúrgica. Rio de Janeiro; Elsevier: 2010. p.123-137.
2. Ferreira AM, Andrade D. Sítio cirúrgico: avaliaçao e intervençoes de enfermagem no pós-operatório. Arq ciênc saúde. 2006;13(1):27-33.
3. Sharp KA, McLaws ML Wound dressings for surgical sites (Protocol). Cochrane Database of Systematic Reviews 2001;2(CD003091). DOI: 10.1002/14651858.CD003091.
4. Peruzzo AB, Negeliskii C, Antunes MC, Coelho RP, Tramontini SJ. Protocolo de cuidados a pacientes com lesões de pele. Mom & Perspec Saúde. 2005;18(2):56-69.
5. Ebner JA, Maytin EV. Cicatrizaçao de ferida cutânea. In: Vidimos AT, Ammirati CT, Poblete-Lopez C. Requisitos em Dermatologia: Dermatologia cirúrgica. Rio de Janeiro; Elsevier. 2010: 81-100.
6. Powers JG, Higham C, Broussard K, Phillips TJ. Wound healing and treating wounds: chronic wound care and management. J Am Acad Dermatol. 2016;74(4):607-25.
7. Moriya T, Módena JLP. Assepsia e antissepsia: técnicas de esterilização. Medicina (Ribeirao Preto). 2008;41(3):265-73.
8. Bezerra SMC. O pós operatório na cirurgia dermatológica. An Bras Dermatol. 2017;68(4):205-7.
9. Grandinetti LM, McGillis ST. Avaliaçao pré-operatória do paciente de cirurgia dermatológica. In: Vidimos AT, Ammirati CT, Poblete-Lopez C. Requisitos em Dermatologia: Dermatologia cirúrgica. Rio de Janeiro; Elsevier. 2010: 73-80.
10. Mirastschijski U, Jokuszies A, Vogt PM. Cicatrizaçao de feridas cutâneas: biologia do reparo, ferida e tratamento da cicatriz. In: Neligan PC, Gurtner GC. Cirurgia Plástica - princípios. Rio de Janeiro: Elsevier. 2015: 267-96.
11. Kim YS, Lee HJ, Cho SH, Lee JD, Kim HS. Early postoperative treatment of thyroidectomy scars botulinum toxin: a split-scar, double-blind randomized controlled trial. Wound Repair Regen. 2014;22(5):605-12.
12. Pimentel ER, Oliveira JP, Bloch LD, Niwa AB. Risk of complications during dermatologic surgery: protocol for excisional surgery. An Bras Dermatol. 2005;80(5):493-8.
13. Borges JR, Fleury Junior LFF, Ribeiro AMQ. Pre-operative care in dermatologic surgery. Surg Cosmet Dermatol. 2014;6(2):161-8.
14. Billinsley EM, Maloney ME. Intraoperative and postoperative bleeding problems in patients taking warfarin, aspirin, and others nonsteroidal anti-inflamatory agents: a prospective study. Dermatol Surg. 1997;23(5):381-5.
15. Cook JL, Perone JB. A prospective evaluation of the incidence of complications associated with Mohs micrographic surgery. Arch Dermatol. 2003;139(2):143-52.
16. Allen EJ, Youker SR. Complicaçoes cirúrgicas. In: Vidimos AT, Ammirati CT, Poblete-Lopez C. Requisitos em Dermatologia: Dermatologia cirúrgica. Rio de Janeiro; Elsevier. 2010:207-17.
17. Bordeaux JS, Martires KJ, Goldberg D, Pattee SF, Fu P, Maloney ME. Prospective evaluation of dermatologic surgery complications including patients on multiple antiplatelet and anticoagulant medications. J Am Acad Dermatol 2011;65(3):576-83.
18. Saleh K, Schmidtchen A. Surgical site infections in Dermatologic Surgery: etiology, pathogenesis, and current preventative measures. Dermatol Surg. 2015;41(5):537-49.
19. Stracieri LDS. Cuidados e complicaçoes pós-operatória. Medicina (Ribeirao Preto). 2008;41(4):465-8.
20. Reis NA, Machado Filho CDS, Timoner FR. Prophylaxis in dermatologic surgery. Surg Cosmet Dermatol. 2010;2(1):47-53.
21. Fernandes EO, Guerra EE, Pitrez FAB. Avaliaçao pré-operatória e cuidados em cirurgia eletiva: recomendaçoes baseadas em evidências. Rev AMRIGS. 2010;54(2):240-58.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}