


Leonardo Rotolo Araújo; Joaquim Mesquita Filho; Guillermo Loda
Received on: 02/05/2019
Approved on: 01/07/2019
Study conducted at Institute of Dermatology Prof. Rubem David Azulay, Santa Casa de Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
Financial support: None.
Conflito de Interesses: None.
Neck appearance is one of the indicators of a person's biological age. Conventional rhytidoplasty has been the standard treatment for correction of cervical aging. Some patients, especially men, show evident changes in the neck, with excess skin and/or fat in the anterior cervical region, but with little flaccidity of the face. Cervical facelift, combined with zetaplasty, is a surgical option for rhytidoplasty and treats excess skin, fat, and platysma bands. It can be performed under local anesthesia, presenting low morbidity, rapid recovery, and high level of satisfaction.
Keywords: Rhytidoplasty; Rejuvenation; Cervicoplasty; Neck
The appearance of the neck is one of the most accurate indicators of a person's biological age. With the aging process, this region loses its natural shape and contour due to the fat accumulation in the sub-segment, formation of platysma bands, laxity, and excess skin.1
Treatments aim to restore the neck to a youthful appearance, characterized by a well-defined mandibular border, visible thyroid cartilage, well-demarcated anterior border of the sternocleidomastoid muscle, and a cervical-mentonian angle between 105 and 120 degrees.1 Non-surgical therapeutic options have gained popularity in the last decade. However, long-term benefits are limited and ineffective for treating excess cervical skin.2
Facial and neck lift (rhytidoplasty) with periauricular incision has been the most traditional surgical option for the treatment of aging of the lower third of the face and cervical region.2 However, this is an invasive surgery with long recovery time and high cost. A growing number of patients, particularly men and elderly population, have sagging and excess skin more evident in the neck than in the face, a condition called "turkey neck".3
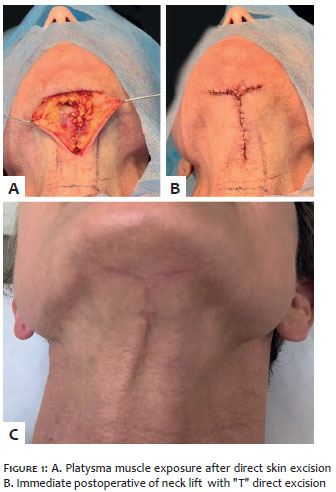
Several surgical techniques of neck lift with direct skin excision have been described to treat this condition. The original technique consisted of performing a "T" excision (Figure 1) in the submental region, and it is an option for patients with slight skin and fat excess. For moderate to severe cases, zetaplasty neck lift achieves superior results and is an ideal choice. Zetaplasty increases the cervical-mentonian angle definition due to increased neck constriction and helps to improve the functional and aesthetic outcome of the resulting cervical scar.4
Direct excision neck lift and zetaplasty is suitable for patients with sagging neck, with or without submental fat, who do not wish to undergo traditional rhytidoplasty or who are contraindicated for this procedure. It can be performed under local anesthesia, presenting low surgical morbidity, fast recovery and high level of patient and surgeon satisfaction.4
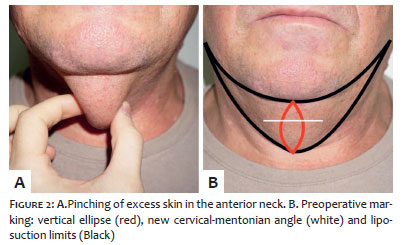
With the patient seated, the excess skin is pinched in the anterior neck (Figure 2A), and a vertical ellipse (spindle) is marked in the midline, with the apex in the submental sulcus and the inferior extension covering the entire redundant skin. The ellipse diameter is conservatively marked. Then the level of the new cervical-mentonian angle is marked with a horizontal line approximately at the level of the hyoid bone. If submental liposuction is required, the following limits are marked: lower border of mandible, superiorly; thyroid cartilage or suprasternal notch, inferiorly; anterior border of the sternocleidomastoid muscle, laterally (Figure 2B).
After local antisepsis, subcutaneous infiltration of a tumescent anesthetic solution with 0.9% saline, 1% lipid, and 1:100,000 epinephrine is performed. In individuals with excess cervical fat, preplatysmal fat liposuction (above the platysma) is performed using 3mm diameter cannulas coupled to a 20ml or 60 ml aspirator or syringe.
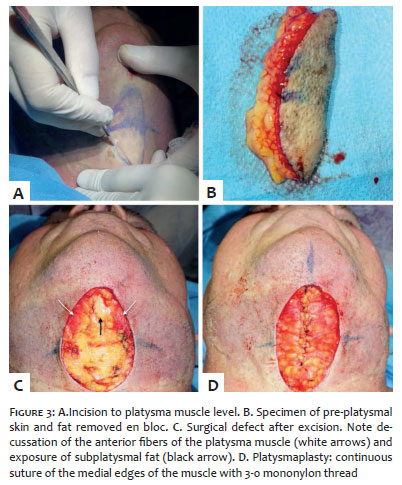
Subsequently, skin and subcutaneous tissue incisions are made to the platysma muscle. Excess preplatysmal skin/fat is removed "en bloc", exposing the platysma muscle (Figures 3A, B, and C). Since liposuction only removes preplatysma fat, when there is extreme adipose tissue accumulation (morbidly obese), direct lipectomy of subplatysmal fat (located between the platysma and the anterior belly of the digastric muscles) may be performed. Removing it, if necessary, will help to improve the contour and shape of the neck, making it more concave. Excessive removal of subplatysmal fat should be avoided as it may cause an unsightly result called "snake neck". Most patients with cervical aging also have flaccidity and/or division of the medial borders of the platysma muscle. Thus, platysmaplasty is usually performed (Figure 3D). It consists of approaching and suturing the medial borders of the muscle with single or continuous stitches and 3-0 mononylon thread. It helps to reverse the platysma laxity and to provide a better tightening effect of the neck. Before border suturing, a platysma portion of the midline can be removed, allowing for a firmer approach.
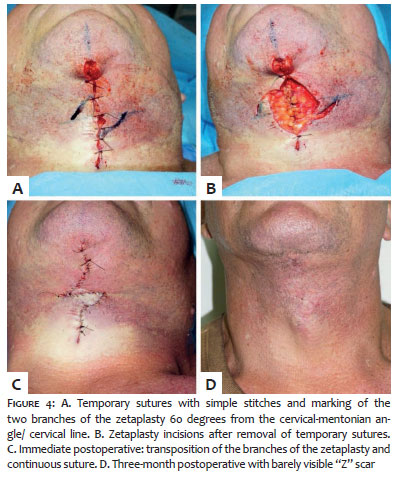
After completion of the treatment of preplatysmal, platysmal and, if necessary, subplatismal fat, zetaplasty is performed. Initially, the sides of the neck should be detached in the subcutaneous plane. Then the surgical defect is temporarily closed in a vertical line. The marking of the cervical-mentonian angle is again verified and used as the central branch of zetaplasty. Two oblique lines of 2cm and 60 degrees are drawn (Figure 4A). Temporary sutures are removed, and incision and transposition of both flaps are made (Figure 4B).
Finally, the surgical wound is sutured with 4-0 polyglactin 910 intradermal sutures in the deep layers and continuous 5-0 mononylon suture in the superficial layer. The resulting zetaplasty is in the cervical line/ cervical-mentonian angle drawn preoperatively (Figure 4C).
A compressive dressing and bandage are placed to prevent bruising. The patient is reevaluated after 24 hours for dressing change, and the sutures are removed within seven to 10 days.
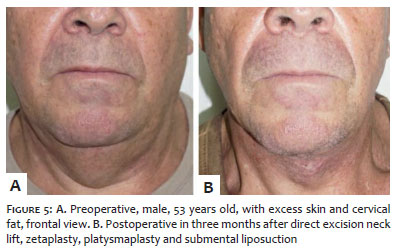
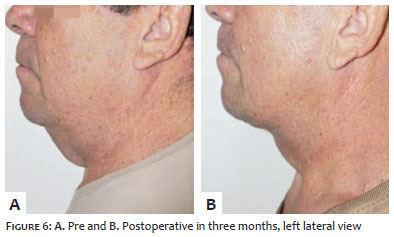
Significant improvement of the cervical region can already be observed in the immediate postoperative period. Three-month postoperative photography exhibits excellent results (Figures 5, 6, 7, and 8). The three assessed patients reported a high level of satisfaction with the results and believed that the aesthetic improvement of the neck exceeds the resulting scar.
Cronin and Biggs originally described the neck lift technique associated with zetaplasty in 1971 for the treatment of men with cervical sagging and "turkey neck" appearance. It has emerged as an alternative to traditional facial lift and can be indicated for any patient, including women, who have excess neck skin, apparent platysma bands, submental fat, and who is willing to accept isolated neck rejuvenation in exchange for a discreet scar in "Z".3
The negative aspects of the described technique include the presence of visible scar and little improvement of the jowl, as it only treats the neck. Scars in the anterior cervical region are usually well camouflaged. The upper portion (above the thyroid cartilage) is usually not seen in daily life unless the patient performs a neck extension movement, and the visible lower portion is usually little evident.4 Hypertrophy may occur, and Miller reported this complication in 12 of 74 patients who underwent this procedure.5 Erythema improves over time or with intense pulsed light sessions. The zetaplasty allows the resulting vertical scar to be less visible, more camouflaged, and with a lower risk of contracture. Other complications, such as expansive hematoma and necrosis, are rare.4
The technique can also be used concomitantly with rhytidoplasty in patients with severe excess cervical skin or with recurrence of sagging after surgery. Although not as comprehensive as a conventional face and neck lift, this technique presents surgery, anesthesia, recovery, and cost markedly lower. As with any surgical procedure, it is necessary to understand the benefits and disadvantages of this technique and to note that it does not apply to all patients but to a specific group of individuals.3
Neck lift with the direct excision technique and zetaplasty is a procedure that achieves a high level of patient and surgeon satisfaction and may be an alternative to conventional rhytidoplasty.
Leonardo Rotolo Araújo | ORCID 0000-0003-0481-8224
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Joaquim Mesquita Filho | ORCID 0000-0001-6047-0205
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Guillermo Loda | ORCID 0000-0003-0511-0025
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Ellenbogen R, Karlin JV. Visual criteria for success in restoring the youthful neck. Plast Reconstr Surg. 1980; 66(6):826-37.
2. Joseph JH. Nonsurgical neck laxity correction. Clin Plast Surg. 2014;41(1):7-9.
3. Cronin TD, Biggs TM. The T-Z-plasty for the male "turkey gobbler" neck. Plast Reconstr Surg 1971;47(6):534-38.
4. Biggs TM, Steely RL. The male neck and T-Z-plasty:28 years later. Aesthetic Surg J. 2000;20(1):31-4.
5. Miller TA. Excision of redundant neck tissue in men with platysma plication and Z plasty closure. Plast Reconstr Surg. 2005;115(1):304-13.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}