


Elisa Raquel Martins da Costa Marques1; Ada Regina Trindade de Almeida2; Vanessa Rocha de Moura Moreira1; Maria Victoria Suarez Restrepo3
Received on: 10/08/2019
Approved on: 01/09/2019
Study conducted at the Hospital do Servidor Público Municipal de São Paulo - São Paulo (SP), Brazil.
Financial support: None.
Conflito de Interesses: None.
INTRODUCTION: Raynaud's phenomenon (RP) is an exaggerated physiological response of the extremity vessels, mainly to cold and stress. Patients refractory to clinical treatment or intolerant to its adverse events may be treated with local injection of botulinum toxin (BTX).
OBJECTIVE: To describe the experience of botulinum toxin use in severe cases of RP.
METHODS: Observational, descriptive, retrospective, and unicenter study of case series of severe RP treated with BTX-A, from 2011 to 2015. Parameters of pain, numbness, color, and stiffness were scored by visual analogical scale (VAS) and tabulated and compared before and after the treatment.
RESULTS: Total pain improvement in 71.4% of cases and partial improvement in 28.6%. Numbness disappeared in 57.1% of cases and improvement in 42.9%. There was a total regression of stiffness in 57.1% of cases and partial improvement in 28.6%. The color was completely reversed in 57.1% of the patients. There was ulceration healing in the only case in with they were present. Ischemic attacks were reduced in 85,7% of cases. No complications occurred.
CONCLUSIONS: This study suggests that the use of BTX-A in patients with severe RP is a promising therapeutic option.
Keywords: Raynaud disease; Botulinum toxins; Botulinum toxins, type A
Raynaud's phenomenon (RP) is an exaggerated physiological response of the extremity vessels, especially to cold and emotional stress.1 Traditionally, three phases characterizes it: pallor (vasoconstriction), cyanosis (due to blood deoxygenation), and redness (reactive hyperemia).2
Most cases of RP are classified as primary or idiopathic and are not associated with other conditions. Less often, RP is classified as secondary and is associated with conditions such as connective tissue diseases, especially systemic scleroderma (SSc).3,4
The pathogenesis of primary RP is related to the exacerbated stimulation of alpha-adrenergic receptors present in vascular smooth muscle, causing its vasoconstriction. Primary RP can be controlled with preventive measures, keeping the patient away from triggering factors such as cold exposure, stress, caffeine, vasoconstrictor medications, and smoking.1,4 On the other hand, in secondary RP, the presence of structural vasculopathies characteristic of associated diseases potentiates the reduction of vessel caliber and makes such patients more prone to develop pain, numbness, and ischemic complications, such as functional limitation, digital ulcers, and partial digit amputations, promoting strong impact on quality of life.4
In the presence of RP signs and symptoms, despite the adoption of preventive measures, pharmacological treatment is required to regulate vasodilation/ vasoconstriction. Several drug classes are available, such as antiplatelet agents, cilostazol, sarpogrelate, intravenous and oral prostanoids, phosphodiesterase type 5 inhibitors (PDE5), endothelin receptor antagonists (ERA), and bosentan. However, calcium channel blockers remain the therapy of choice in treating this condition.5 When patients are refractory to clinical treatment or cannot tolerate the adverse events, there are few alternative therapies, including surgical treatment (periarterial sympathectomy), and, more recently, the use of local botulinum toxin injection (BTX).6
Botulinum toxin is a polypeptide composed of a light chain (50kDa) and a heavy chain (100kDa) joined by disulfide bond. It is produced by the gram-negative bacterium Clostridium botulinum and was discovered in 1897 by Emile van Ermengen, in Belgium. In 1949, Arnold Burgen described the first elucidation of its mechanism of action as an inhibitor of acetylcholine release in neuromuscular junctions.7
Of the seven existing types of BTX (A-G), two (BTX-A and BTX-B) have been successfully used in both dermatological and cometic therapy, and in recent years they have been cited as a therapeutic option for symptomatic RP cases refractory to clinical treatment. This is because they act on the various pathogenesis of the disease, inhibiting adrenergic or cholinergic sympathetic vasoconstriction and acting on various pain-related neurotransmitters, such as norepinephrine, substance P, glutamate, and calcitonin gene-related peptide (CGRP).2,8-11
Such use was first reported in 2004 by Sycha et al. in two patients with severe and intractable Raynaud's phenomenon. These patients showed improvement in stiffness and numbness as well as increased digital perfusion.12
In 2007, Vanbeek et al. described a series of 11 patients with Raynaud's phenomenon secondary to connective tissue disease. In this study, the injections were performed only on the affected fingers, with early recurrence on the uninjected fingers, which justified a change in the treatment protocol for all fingers. All patients received a total dose of 100 U/hand and showed pain relief within two days (pain score decrease from 9-10 to 0-2). Nine out of 11 patients had ulcer healing and two underwent successful grafts.3
Then, Fregene et al. sought to standardize the injection technique in a series of 26 patients. However, statistical evaluation did not define a specific injection site with superior results.1
Most botulinum toxin publications in RP show the experiences of countries in North America (USA and Canada), Europe (France, Austria and England), Asia (Japan and China), and South America (represented by Colombia only). However, so far, national research on the subject has not been found.
To describe the experience of using botulinum toxin type A in patients with severe Raynaud's phenomenon.
Observational, descriptive, retrospective, single-center, case series study conducted following the ethical principles of the Declaration of Helsinki, the Americas document, following the guidelines of Good Clinical Practice (GCP) and local laws of Brazil where it was developed. It was submitted and approved by the institution's Research Ethics Committee (REC) under number 3.510.407.
Patients older than 18 years of age, treated at the Collagenosis Outpatient Clinic of the Dermatological Clinic of the Hospital do Servidor Público Municipal de São Paulo (HSPM), from June 2011 to July 2015, were selected. The inclusion criteria were previous diagnosis of clinically evident RP refractory to clinical treatment; application of botulinum toxin to treat RP in the period mentioned; follow-up for at least four months after the application, and signature of the Informed Consent Form (ICF).
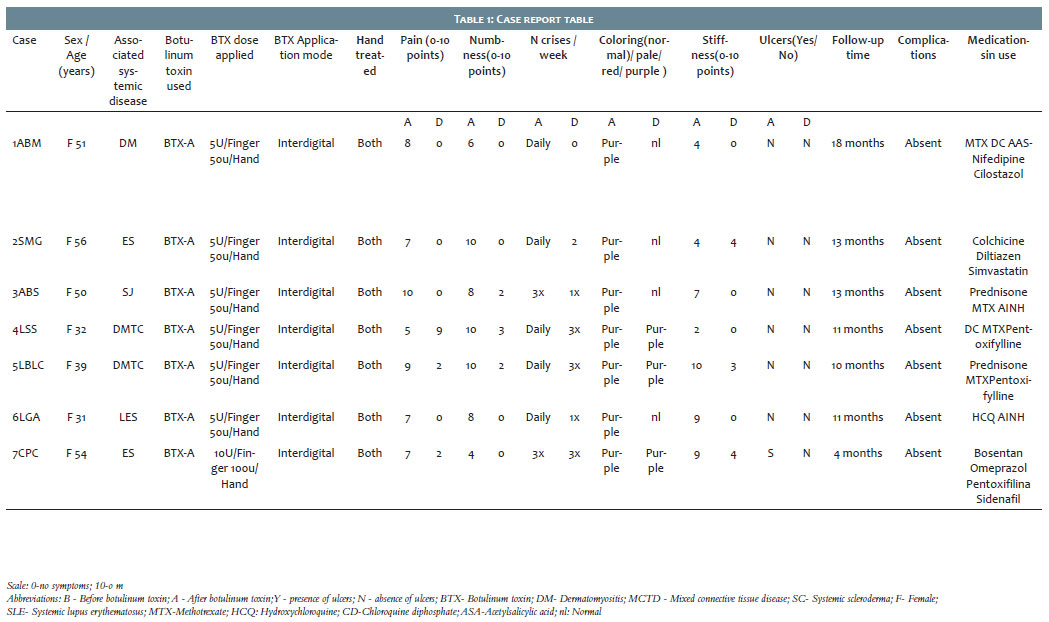
Patient data such as gender, age, associated disease and respective treatments, type of toxin, dose and mode of application, as well as the treated hand were evaluated. Information on pain, numbness, color, and stiffness were scored and evaluated using the visual analog scale (VAS) applied before and after the treatment. Episodes numbers, ulceration regression, follow-up time, and BTX adverse events were also recorded. All information was collected from the HSPM medical records and transcribed into a data collection table designed by the researchers.
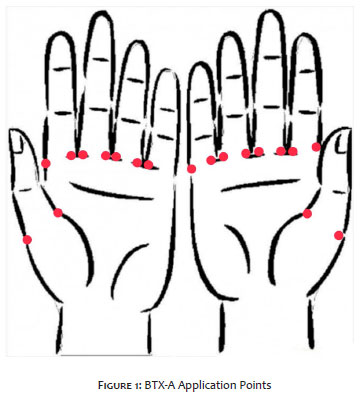
We found seven women (100%) with a mean age of 45 years, ranging from 31 to 56 years. All had been treated with BTX-A injections on the lateral and medial surfaces of the finger bases, as shown in Figure 1.
The doses applied were 10 UI/finger in one case (14.3%) and 5 UI/finger in six cases (85.7%). All seven patients had RP secondary to collagenosis (100%), one had dermatomyositis (14.3%), one had systemic lupus erythematosus (14.3%), two had systemic scleroderma (28.55%), two had mixed connective tissue disease (28.55%), and one had Sjögren's syndrome (14.3%). Table 1 presents the demographic data.
The mean follow-up was 11.4 months, ranging from 4 to 18 months. Pain improved by 100% in five of the seven cases (71.4%). In the remaining two cases (28.6%), this improvement was over 70%. Numbness disappeared after treatment in four of seven cases (57.1%) and improved 70% or more in three cases (42.9%). Regarding finger stiffness, there was total regression in four of seven patients (57.1%), partial improvement greater than 50% in two cases (28.6%), and no change in one patient (14.3%). The color, which was related to perfusion, was reversed entirely from purple to normal in four of seven cases (57.1%), and in three cases (42.9%), there was no change.
In the only case where ulcerations were present, complete healing occurred within 90 days post-toxin. Regarding the frequency of ischemic attacks, in six women (85.7%) the reduction ranged from 50% to 100%, and in only one case (14.3%) it did not change. No early or late postoperative complications were described in any of the seven patients.
Since the first description in 2004 by Sycha et al., several authors have been reporting promising results in the use of botulinum toxin for refractory RP cases.1,3,5,8,11
In our study, we used BTX-A to treat RP in 100% of patients, following the literature trend due to its already validated indications. Only one study used serotype B.2,13 According to Kranz et al., in 2010 there would be no difference in efficacy between these serotypes, and only their pharmacokinetics would be different. BTX-A would have the advantage of presenting a longer duration of action (>1 year), reducing the frequency of injections.14
Several studies describe botulinum toxin use, but most use heterogeneous populations, including patients with primary RP (which by definition is not associated with an underlying connective tissue disease) or with RP secondary to other connective tissue diseases.1,3,4,7,8,12,15-17 Only five studies specifically focus on RP secondary to scleroderma,2,13,18-20 limiting the interpretation of the evidence for this patient population.19
In our study, we used a heterogeneous group of patients with RP secondary to five different types of collagenosis. Only one of these patients, who had more severe sclerosis, responded less well to treatment, as in a single case series suggesting that individuals with sclerosis may be less responsive to BTX-A injections compared to other patients with RP.8 This may be because in scleroderma there is an association of vasospasm with the sclerotic mechanical component of the arterial wall that could theoretically make this group more prone to severe symptoms, frequent ischemia, and complications, as well as reducing its response to toxin.4,21,22
All other patients in our study, including the less severe case of scleroderma, presented a good response to BTX, suggesting that this treatment is also effective in RP secondary to scleroderma 2,14,18-22 and the other collagenoses.1,3,4,12,17,18,23 Regarding toxin application, there is no consensus on dilutions, injection sites, and doses, which vary according to the authors.1-3,5 The doses used in our study follow the literature trend of 50U to 100U BTX-A per hand described by Van Beek and Neumeister.3,8
Fregene et al. tried to standardize injection sites by separating patients into three application categories based on their symptoms: interdigital neurovascular bundles; distal superficial palmar arch; and proximal phalanges, adjacent to the radial and ulnar arteries in the wrist. However, the statistical evaluation was unable to find a better injection pattern.1,5
Thus, as distal digital injections can be equally effective, there is currently a tendency to avoid toxin application in the palmar region, as it is associated with muscle weakness, even without statistical significance. This adverse event, found in the literature, is related to neuromodulator diffusion to the intrinsic hand musculature.1,2,5 In our study, injections were limited to the lateral and medial sides of the digits. Thus, we didn't observe muscle weakness in our cases.
A previous study reporting cases of early recurrence in non-treated fingers when injections were restricted to the affected fingers only justified the choice of applying the toxin to the base of all fingers (affected or not) in both hands.3,5
Regarding the clinical presentation of RP, BTX-A injections showed promising results in improving pain, numbness, stiffness, number of seizures, ulcerations, and cold sensitivity.1,3,5,8,12
Decreased muscle contraction can explain the reduction of stiffness symptoms. When the toxin undergoes endocytosis in the presynaptic nerve ending, it binds to synaptosome nerve-associated protein 25 (SNAP-25 of the SNARE complex), inhibiting it and preventing the mobilization and exocytosis of acetylcholine vesicles in the nerve terminal membrane. Without cholinergic stimulation, muscle cells do not contract, contributing to the treatment of stiffness observed in patients.2,23,11 Our results showed improvement of this symptom, with total regression in 57.1% of patients, and partial regression in 28.6% of them, is consistent with the literature.2,11,12,17,23
Cholinergic neuromuscular action can also explain pain and numbness reduction, since vascular smooth muscle cells are also inhibited, promoting vasodilation and reperfusion. However, some authors question whether there would be other mechanisms involved. This is because the effect of the toxin on pain and numbness modulation is immediate and could not be explained only by the anticholinergic action, which would require a longer time to cause muscle paralysis and, consequently, flow restoration. BTX-A also acts by blocking several neurotransmitters related to C-fiber depolarization that propagate chronic pain, such as norepinephrine, substance P, glutamate, and calcitonin gene-related peptide.2,11,23
Another possible mechanism of action is the inhibition of alpha-2 adrenergic receptor expression both in the peripheral nerve walls chronically irritated by ischemia or trauma and in the vessel walls, suppressing cold-induced noradrenergic vasoconstriction. Also, it has been reported that, in vitro, the toxin would reduce the intracellular accumulation of reactive oxygen species (ROS) produced in response to cooling, which is responsible for enhancing surface expression of adrenergic receptors. Finally, BTX-A could further reduce pain by inhibiting ectopic sodium channels expressed chronically in nerves irritated or injured by chronic ischemia in patients with RP.20
Two case series reported pain and numbness improvement with the use of BTX-A was reported, which described a decrease in both symptoms in all patients evaluated.12,18 Other 16 studies have shown pain reduction in 75% to 100% of cases, but with no evaluation of numbness.1-3,6-8,11,13,16,18-21,23-25 In our study, total pain regression occurred in 71.4% of cases and partial improvement in the remaining 28.6%. Numbness disappeared in 57.1% of patients and partially decreased in 42.9%.
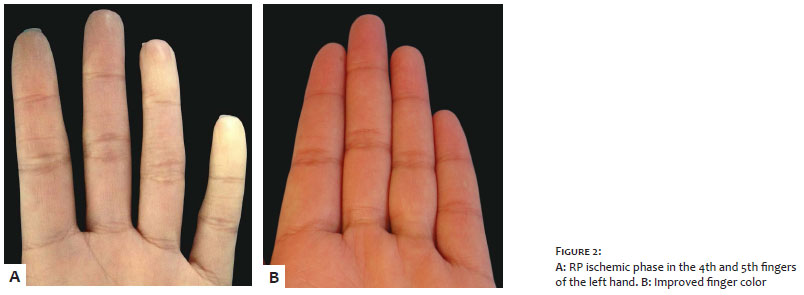
The normalization of the finger color using BTX-A is also described by some authors.1,11,20,24 The vasodilation provided by the neuromodulator leads to the blood flow restoration and fingers reperfusion. Thus, the fingers resume their pink color. In our study, 57.1% of the patients had a complete change from purple to pink, as shown in Figure 2.
A similar mechanism of action justifies the beneficial effects of BTX-A on the healing of digital ulcers secondary to RP.5 By acting to prevent disregulation between vasoconstriction and vasodilation in RP, the toxin disrupts the vicious cycle of ischemia-reperfusion (I/R). Blood reperfusion would lead to infiltration of inflammatory cells and production of pro-inflammatory cytokines in previously ischemic tissue, resulting in damage to vascular endothelium, edema, capillary narrowing, apoptosis, and tissue necrosis.20,26,27
An experimental study showed that BTX-A injection prevented the formation of skin ulcers after I/R induction in a murine model. The toxin reduced the area of hypoxic tissue and protected it from oxidative stress and cell apoptosis.28 Another 10 publications have reported human cases of healing of digital ulcer secondary to RP with BTX-A.2,3,8,13,16-21,23,25 In the only case of our study where ulcers were present, there was complete lesion closure within 90 days post-toxin (Figure 3), following the findings in the literature.
Regarding the frequency of ischemic attacks, our results showed a reduction in the number of episodes and were similar to those found in three other studies.3,18,20 Although the mechanism of action is not well established, it is believed that the toxin would act by reducing the expression of alpha-2-adrenergic receptors on vessel surfaces. Thus, patients would become less responsive to sympathetic discharges triggered by cold and stress,7 stimuli considered the main provokers of vasoconstriction and ischemic attacks in RP.1
Further research is still needed to build consensus on BTX-A doses, dilutions, and injection sites. Despite the small sample size, the beneficial and fast toxin results seen in our case series suggest this medication may be a promising therapeutic option in refractory RP cases.
Elisa Raquel Martins da Costa Marques | 0000-0001-7067-9002
Approval of the final version of the manuscript; study design and planning; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of cases studied; critical revision of the manuscript.
Ada Regina Trindade de Almeida | 0000-0002-4054-2344
Study design and planning; active participation in research orientation; intellectual participation in conduct propaedeutic and/or therapeutic of the studied cases.
Vanessa Rocha de Moura Moreira | 0000-0002-0239-8919
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Maria Victoria Suarez Restrepo | 0000-0002-2614-6011
Statistical analysis; approval of the final version of the manuscript; critical revision of the manuscript.
1. Fregene A, Ditmars D, Siddiqui A. Botulinum Toxin Type A: a treatment option for digital ischemia in patients with Raynaud's phenomenon. J Hand Surg Am. 2009; 34(3):446-52.
2. Serri J. Legré R, Veit V, Guardia C, Gay AM. [Botulinum toxin type A contribution in the treatment of Raynaud's phenomenon due to systemic sclerosis]. Ann Chir Plast Esthet. 2013; 58(6):658-62. Francês.
3. Van Beek AL, Lim PK, Engrenagem AJL, Pritzker MR. Management of vasospastic disorders with botulinum toxin A. Plast Reconstr Surg.2007; 119(1):217-26.
4. ebryk P, Puszczewicz MJ. Botulinum Toxin A in the Treatment of Ray- naud's Phenomenon: a Systematic Review. Arch Med Sci. 2016; 12(4):864-70.
5. Iorio ML, Masden DL, Higgins JP. Botulinum toxin A Treatment of Raynaud's Phenomenon: a Review. Semin Arthritis Rheum. 2012; 41(4):599- 603.
6. Devulder J, van Suijlekom H, van Dongen R, Diwan S, Mekhail N, van Kleef M, Huygen F. 25. Ischemic Pain in the Extremities and Raynaud's Phenomenon. Pain Pract. 2011; 11(5):483-91.
7. Neumeister MW. The Role of Botulinum Toxin in Vasospastic Disorders of the Hand. Hand Clin. 2015; 31(1):23-37.
8. Neumeister MW. Botulinum Toxin Type A in the Treatment of Raynaud's Phenomenon. J Hand Surg Am. 2010; 35(12):2085-92.
9. Wigley FM, Flavahan NA. Raynaud's Phenomenon. N Engl J Med. 2016; 375(6):556-65
10. Flavahan NA. A Vascular Mechanistic Approach to Understanding Raynaud Phenomenon. Nat Rev Rheumatol. 2015;11(3):146-58.
11. Zhou Y, Liu Y, Hao Y, Feng Y, Pan L, Liu W, et al. The Mechanism of Botulinum to Raynaud's Syndrome. Drug Des Devel Ther. 2018; 12:1905-15.
12. Sycha T, Graninger M, Auff E, Schnider P. Botulinum toxin in the treatment of Raynaud's phenomenon: a pilot study. Eur J Clin Invest. 2004; 34(4):312-13.
13. Motegi SI, Sekiguchi A, Saito S, Ishibuchi H, Kishi C, Yasuda M, et al. Successful treatment of Raynaud's phenomenon and digital ulcers in systemic sclerosis patients with botulinum toxin B injection: Assessment of peripheral vascular disorder by angiography and dermoscopic image of nail fold capillary. J Dermatol. 2018; 45(3):349-52.
14. Kranz G, Paul A, Voller B, Posch M, Windischberger C, Auff E, et al. Long- Term Effectiveness and their Powers of Botulinum Toxin A and B: a randomized, Double-Blind. Br J Dermatol. 2011; 164 (1):176-81.
15. Roguedas AM, Misery L. [Improvement of idiopathic Raynaud's phenomenon following local infusion of botulinum toxin]. Ann Dermatol Venereol. 2014; 141(6-7):462-63. Francês.
16. Navarro EP, Cañas CA, Tobón GJ. Digital Ulcer Management of Raynaud's with Interdigital Injection of Botulinum Toxin A. Rheumatology (Oxford). 2016;55(7):1216
17. Zhang X, Hu Y, Nie Z, Song Y, Pan Y, Liu Y, et al. Treatment of Raynaud's phenomenon with botulinum toxin type A. Neurological Sciences. 2015; 36(7):1225-31.
18. Uppal L, Dhaliwal K, Butler PE. A Prospective Study of the Use of Botulinum Toxin Injections in the Treatment of Raynaud's Syndrome Associated with Scleroderma. J Hand Surg Eur Vol. 2014; 39(8):876-80
19. Bello RJ, Cooney CM, Melamed E, Follmar K,Yenokyan G, Leatherman G, et al. The Therapeutic Efficacy of Botulinum Toxin in Treating Scleroderma- Associated Raynaud's Phenomenon: A Randomized, Double Blind, Pla- cebo-Controlled Clinical Trial. Arthritis Rheumatol. 2017; 69(8):1661-69.
20. Motegi S, Yamada K, Toki S, Uchiyama A, Kubota Y, Nakamura T, et al. Beneficial Effect of Botulinum Toxin A in Raynaud's Phenomenon in Japanese Patients with Systemic Sclerosis: a Prospective Study of Case Series. J Dermatol. 2016; 43(1):56-62.
21. Cappelli L, Wigley FM. Management of Raynaud Phenomenon and Digital Ulcers in Scleroderma. Rheum Dis Clin North Am. 2015; 41(3):419-38.
22. Wigley FM, Flavahan NA. Raynaud's Phenomenon. N Engl J Med. 2016; 375(6):556-65.
23. Neumeister, MW, Chambers, CB e Herron, MS (2010). Botox Therapy for Ischemic Digits. Journal of Vascular Surgery, 51 (2), 522. doi: 10.1016 / j.jvs.2009.12.053
24. Kossintseva I, Barankin B. Improvement in Both Raynaud Disease and Hyperhidrosis in Response to Botulinum Toxin Type a Treatment. J Cutan Med Surg. 2008; 12(4):189-93.
25. Polsky D. Botulinum Toxin-A for the Treatment of Raynaud Syndrome. Arch Dermatol. 2012; 148(4):426-8.
26. Carroll WR, Esclamado RM. Ischemia/reperfusion injury in microvascular surgery. Head Neck. 2000; 22(7):700-13.
27. Kasuya A, Sakabe J, Tokura Y. Potential Application of in Vivo Imaging of Impaired Lymphatic Duct to Evaluate the Severity of Pressure Ulcer in Mouse Model. Sci Rep. 2014; 4: 4173.
28. Uchiyama A, Yamada K, Perera B, Ogino S, Yokoyama Y, Takeuchi Y, et al. Protective Effect of Botulinum Toxin A After Cutaneous Ischemia-Reperfusion Injury. Sci Rep. 2015; 5: 9072.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}