


Carlos Roberto Antonio1,2; Lívia Arroyo Trídico2,3; Ana Luiza Valle Esteves4
Received on: 10/04/2019
Approved on: 01/08/2019
Study conducted at the Pelle Medical Center - São José do Rio Preto (SP), Brazil.
Financial support: None.
Conflict of interests: None.
INTRODUCTION: Facial aging occurs due to loss of facial volume and altered skin texture. Hyaluronic acid fillers are the main non-surgical tools used to recover the volume loss, since, besides filling, they act as skin remodeling.
OBJECTIVE: To describe a new facial rejuvenation technique with hyaluronic acid: delta V lifting. Through this technique, we seek not only to fill in areas with volume deficits but mainly to stimulate tissue regeneration through the interaction between hyaluronic acid and superficial subcutaneous tissue, the main application plan.
METHODS: A retrospective observational study assessing 200 patients treated with 2 ml of hyaluronic acid at a concentration of 23 mg/ml in a single therapy session with the delta V lifting technique.
RESULTS: 87% of patients rated the result as “great improvement” and 13% as “good improvement” according to the Global Aesthetic Improvement Scale. Also, they all reported progressive improvement of the result until the moment of return within one month after the procedure.
CONCLUSIONS: The delta V lifting technique was effective in bringing satisfactory aesthetic results with a minimal amount of hyaluronic acid. The interaction between hyaluronic acid and adipose tissue is believed to be involved in optimizing results.
Keywords: Hyaluronic acid; Rejuvenation; Techniques
Facial aging is characterized by different phenomena that occur at about the same time: variable skin atrophy and wrinkle formation caused by genetic, actinic and environmental factors; loss of bone volume; loss of facial fat, and sagging skin.1 Thus, facial aging consists of a dynamic and complex interaction of several factors involving three-dimensional changes that occur in the skeleton, as well as in soft tissue structure, associated with superficial skin changes.2,3
The drooping appearance associated with aging is due to both facial volume loss and skin texture change.4 Thus, flattening of the concavities of the forehead, eyebrow, glabella and temporal region of the upper face, drooping of the nasal tip, flattening of the cheek in the middle third and retraction of the chin, loss of lip volume, and drooping of the oral commissure in the lower face characterize the aged face.5
Hyaluronic acid fillers are the main non-surgical tools used to recover the lost volume. In the past, fillers were mostly used for surface treatments, but nowadays, they have been widely used in volumizing, prioritizing in-depth application plans, and not just superficial skin. By promoting volumization, fillers help limit the impact of sagging and ensure a lifting effect. 6
There are several filling techniques with hyaluronic acid, such as serial puncture, linear threading, fanning, cross-hatching, and tower technique. An excellent technique depends on the filling agent, the target area to be corrected, and the physician's preference. Their use seeks the best aesthetic results for each case.7
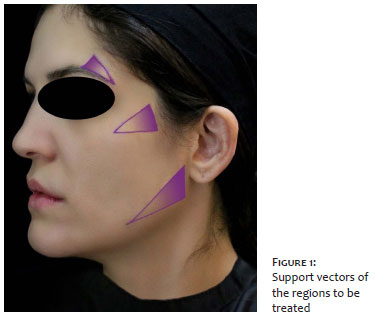
The main objective for rejuvenating the face as a whole should be to restructure the lost volume and treat sagging skin. The areas of resorption should be selected and individualized according to each person's characteristics. Thus, we seek to promote rejuvenation with hyaluronic acid through a new technique: delta V lifting. This technique consists of identifying areas with sagging and/or loss of volume and marking them individually in the shape of a triangle (delta). The base of the triangle is the region that presents the highest tissue resorption and, therefore, should receive the most substantial filler volume, while the apex (delta tip) receives the least amount of hyaluronic acid. Also, the triangle represents support vectors (V) (traction movement effect) to perform the lifting effect of the region to be treated.
This new technique can be safely used in various regions of the face, as it should be performed with the use of a cannula (preferably 22G) to prevent the involvement of facial blood vessels. Thus, we seek to perform facial restructuring by identifying areas of volume loss and distribution of hyaluronic acid in triangle-shaped support vectors, promoting more harmony and naturalness to the aged face.
Retrospective, observational study that assessed 200 patients treated at a private clinic in the city of São José do Rio Preto, SP, Brazil, from January to December 2018. We included patients over 20 years old, men and women, who did not perform any other treatments than the one proposed in this study. The Research Ethics Committee of the São José do Rio Preto Medical School, SP, approved this study.
All patients were treated with hyaluronic acid 2ml at a concentration of 23 mg/ml in a single therapeutic session. The areas to be treated were marked in triangles (deltas) individually, assessing the areas of volume loss and support in each patient. The triangles size triangles and the number of deltas marked in the patients were specific to each individual according to their needs. However, the primary identified regions to be filled in were: temporal region, supraciliary region, zygomatic region, mandibular region, nasojugal groove region, nasolabial fold region, labiomental groove region, and labial region.
After identifying the treatment areas and the support vectors of each region, the deltas were designed with the base corresponding to the area with the highest support loss. Thus, the direction of the sustaining vectors moves from the triangle apex to its base (Figure 1). For each triangle to be filled, anesthesia was administered about 0.5 cm from the apex with lidocaine hydrochloride 2.0% associated with norepinephrine hemitartrate (1:50,000 in norepinephrine).
After performing the anesthetic button, we used a 21G needle to make the cannula insertion hole. We inserted the 22G cannula at the apex of the triangle, applying hyaluronic acid in the subcutaneous plane through retro-injection with a larger amount of filler at the base of the triangle. We administered three to four retro-injection lines in each triangle. The application plan is in the superficial dermis, just below the dermis, except for the nasojugal groove region, where it is applied in the periosteum plane, and in the lip, where it is performed in the muscle.
After the procedure, the patients returned within one month for medical evaluation, photography, and satisfaction questionnaire. Two physicians not involved in the research evaluated the photographs to rank the results according to the Global Aesthetic Improvement Scale:8 great improvement (excellent cosmetic result), good improvement (marked improvement in appearance, but not entirely optimal), regular improvement (obvious improvement of the appearance, but a touch-up or a new treatment is advised), unaltered (the appearance is essentially the same compared with the original condition) and worsening (the appearance is worse compared with the original condition).
Of the 200 patients assessed, 18 (9%) were 20 to 30 years old, 55 (27.5%) were 31 to 40 years old, 50 (25%) were 41 to 50 years old, 56 (28%) were 51 to 60 years old, and 21 (10.5%) were 60 to 70 years old. Most of the evaluated patients were women: 184 female patients and 16 male patients.
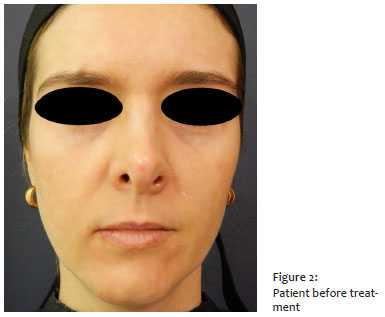
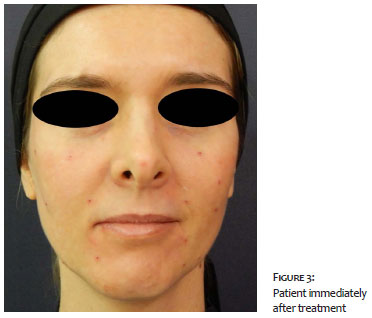
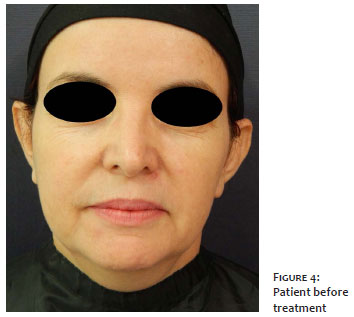
According to the physicians' assessment, 58% of patients were rated as presenting "great improvement" according to the Global Aesthetic Improvement Scale, 30% were rated as "good improvement", and 12% were rated as presenting "regular improvement" (Figures 2, 3, 4, 5).
According to the patient satisfaction questionnaire, 87% rated the result as "great improvement" and 13% as "good improvement" according to the Global Aesthetic Improvement Scale. All were satisfied with the treatment and would indicate the procedure for a family member or friend. All patients answered positively when asked if they would like to perform the procedure in the future. Also, all patients reported realizing the progressive improvement of the result until the time of return within one month after the procedure.
Regarding pain, most patients reported mild pain during the procedure (58%), some reported no pain (39%), and only six patients reported moderate pain. The only adverse event observed was mild hematoma in 35% of patients. Patients were followed for three months after treatment, and no other adverse event occurred.
Hyaluronic acid (HA) is widely used for aesthetic treatments due to its efficacy, safety, low allergen potential, and versatility. In addition to replenishing volume, hyaluronic acid acts as a skin remodeling thanks to the observation of the filling effect persistence for a much longer time than the filler bioavailability. Studies have shown that HA can induce increased collagen and elastic fiber production, restoring extracellular matrix by direct stimulation and/or mechanical stretching of fibroblasts.9
The location of the filler on the skin is one of the determinants of the cosmetic result.10 Dermal localization is not required for excellent results, as studies show that the vast majority of dermal fillers are predominantly subcutaneous, regardless of the various application techniques.10, 11, 12, 13 On the other hand, when fillers are placed on a deeper plane (deep subcutaneous or periosteum), more product is needed to achieve the desired effect.14 In the present study, by injecting hyaluronic acid into the superficial subcutaneous, it was possible to obtain excellent results of volume restoration, sustaining and improvement of facial flaccidity with a small amount of the product (hyaluronic acid 2ml at a concentration of 23mg/ml) and high safety.
An interaction between hyaluronic acid and the subcutaneous tissue where the filler is placed is believed to occur. By increasing the concentration of hyaluronic acid in the adipose tissue, adipocyte expansion occurs in a non-rigid environment, causing a mechanical stress reaction in adipose tissue. Mechanical stress is one of the known factors that induce differentiation of fat-derived stem cells. By injecting hyaluronic acid, mesenchymal stem cells derived from adipose tissue find a microenvironment optimized for expansion and differentiation in connective tissue and endothelial cells, a regenerative pathway resulting in lower filler volume required for facial rejuvenation.15, 16, 17
It is also known that subcutaneous adipocytes control the activity of dermal fibroblasts by cytokine secretion. Human dermal fibroblasts express genes that encode receptors for adiponectin and leptin, cytokines that increase the production of hyaluronic acid in fibroblasts.17, 18 Thus, subcutaneous hyaluronic acid also treats the adjacent dermis, improving sagging skin quality.
Through this new facial rejuvenation technique with hyaluronic acid, we seek not only to fill in areas of volume deficit but mainly to stimulate tissue regeneration through the interaction of hyaluronic acid with the superficial dermis. We thus seek to optimize results with the least amount of hyaluronic acid required for facial remodeling.
The present study demonstrated a high satisfaction rate of the treated patients, minimal adverse events, and positive assessment by the evaluating physicians. Further studies are needed to investigate the exact mechanisms of interaction between hyaluronic acid and subcutaneous acid using this facial rejuvenation technique. Also, the use of a cannula for the hyaluronic acid injection and the delta retro-injection technique brings us certainty regarding the possibility of vascular involvement.
The delta V lifting facial rejuvenation technique is effective in providing satisfactory aesthetic results with a minimal amount of hyaluronic acid. It is believed that the interaction between hyaluronic acid and adipose tissue is involved in optimizing the results.
Carlos Roberto Antonio | 0000-0001-9243-8293
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Lívia Arroyo Trídico | 0000-0002-7743-4195
Statistical analysis; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Ana Luiza Valle Esteves | 0000-0001-9535-1601
Critical literature review.
1. Salti G, Rauso R. Facial Rejuvenation with Fillers: The Dual Plane Technique. J Cutan Aesthet Surg. 2015; 8(3):127-33.
2. Klein AW, Elson ML. The history of substances for soft tissue augmentation. Dermatol Surg. 2000;26(12):1096-1105.
3. Thomas MK, Dsilva JA, Borole AJ, Naik SM, Sarkar SG. Anatomic and mechanical considerations in restoring volume of the face with use of hyaluronic acid fillers with a novel layered technique. Indian J Plast Surg. 2014; 47(1):43-9.
4. Pessa JE, Zadoo VP, Yuan C, Ayedelotte JD, Cuellar FJ, Cochran CS, et al. Concertina effect and facial aging: nonlinear aspects of youthfulness and skeletal remodeling, and why, perhaps, infants have jowls. Plast Reconstr Surg. 1999; 103(2):635-44.
5. John HE, Price RD. Perspectives in the selection of hyaluronic acid fillers for facial wrinkles and aging skin. Patient Prefer Adherence. 2009;3:225-30.
6. Duranti F, Salti G, Bovani B, Calandra M, Rosati ML. Injectable hyaluronic acid gel for soft tissue augmentation. A clinical and histologic study. Dermatol Surg. 1998; 24(12):1317-25
7. Mashiko T, Kinoshita K, Kanayama K, Feng J, Yoshimura K. Perpendicular Strut Injection of Hyaluronic Acid Filler for Deep Wrinkles. Plast Reconstr Surg Glob Open. 2015; 3(11):e567.
8. Hexsel D, Dini TDF, Souza JS, Siega C. Rejuvenation of aging hands with a hyaluronic acid soft tissue filler range: efficacy, safety and patient satisfaction during six months. Surg Cosmet Dermatol 2017; 9(4):297-303.
9. Almeida ART, Sampaio GAA. Hyaluronic acid in the rejuvenation of the upper third of the face: review and update - Part 1. Surg Cosmet Dermatol 2016;8(2):148-53.
10. Wollina UW, Goldman A. Hyaluronic Acid Dermal Fillers: Safety and Efficacy for the Treatment of Wrinkles, Aging Skin, Body Sculpturing and Medical Conditions. Clinical Medicine Reviews in Therapeutics. 2011; 2011(3):107-21.
11. Arlette JP, Trotter MJ. Anatomic location of hyaluronic acid filler material injected into nasolabial fold: a histologic study. Dermatol Surg. 2008; 34 (Suppl 1): S56-62.
12. Greco TM, Elenitsas R. Localization and histological characterization of injected hyaluronic acid in excised nasolabial fold tissue. J Drugs Dermatol. 2010; 9(4):399-404.
13. Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GB. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venereol. 2012; 26(3):292-301.
14. Pontius AT, Chaiet SR, Williams EF 3rd. Midface injectable fillers: have they replaced midface surgery? Facial Plast Surg Clin North Am. 2013; 21(2):229-39.
15. Bayati V, Sadeghi Y, Shokrgozar MA, Haghighipour N, Azadmanesh K, Amanzadeh A, et al. The evaluation of cyclic uniaxial strain on myogenic differentiation of adipose-derived stem cells. Tissue Cell. 2011; 43(6):359-66.
16. Alkhouli N, Mansfield J, Green E, Bell J, Knight B, Liversedge N, Tham JC, et al. The mechanical properties of human adipose tissues and their relationships to the structure and composition of the extracellular matrix. Am J Physiol Endocrinol Metab. 2013; 305(12):E1427-35.
17. Wollina U. Midfacial rejuvenation by hyaluronic acid fillers and subcutaneous adipose tissue--a new concept. Med Hypotheses. 2015; 84(4):327-30.
18. Ezure T, Amano S. Adiponectin and leptin up-regulate extracellular matrix production by dermal fibroblasts. Biofactors. 2007;31(3-4):229-36.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}