


Ludmilla Cardoso Gomes; Abes Mahmed Amed Filho; Mariana Figueiroa Careta; Isabelle I Hue Wu; Vivian Barzi Loureiro; Luis Antonio Ribeiro Torezan
Received on: 12/08/2019
Approved on: 15/09/2019
Study conducted at the Department of Dermatology, Clinic Hospital, Medical School, Universidade de São Paulo - São Paulo (SP), Brazil.
Financial support: None.
Conflict of interests: None.
Vascular anomalies correspond to a broad spectrum of changes that fall into two main groups: 1) vascular tumors, which represent proliferative lesions, and 2) vascular malformations, caused by ectasia in vessels, whether capillary, venous or lymphatic.This article reviews the main vascular anomalies observed in dermatological practice, their main classifications and available treatments, focusing on the use of lasers and intense pulsed light to lighten cutaneous vascular lesions, especially those resulting from malformations.
Keywords: vascular Malformations; Hemangioma; Vascular neoplasms; Laser therapy; Intense pulsed light therapy; Dermatology
Vascular anomalies have a broad clinical spectrum, from an aesthetic-only cutaneous manifestation to life-threatening lesions. They predominate in children and young adults and can be classified into proliferative lesions (tumor) and vascular malformations.1,2 Distinguishing these lesions is difficult due to their phenotypic diversity, and, not infrequently, the term "hemangioma" is misused to describe vascular malformations.1,3 Due to the large number of diseases that constitute vascular anomalies, we review those of primary dermatological interest as well as their main therapeutic approaches.
The oldest classification of vascular anomalies was described in 1863 by Virchow, who divided them into angioma simplex, cavernous angioma, racemic angioma, and lymphangioma, considering the pathology of the lesions.1
Over time, the nomenclature of vascular anomalies changed, and, in 1982, Mulliken and Glowacki proposed a classification that correlated the clinical presentation with the natural history and histopathology of the lesions, dividing them into two main types: hemangiomas and vascular malformations.2,3 Analyzing the clinical evolution and cellular characteristics of 49 specimens of vascular lesions, the authors identified differences that supported the new nomenclature. Hemangiomas in the proliferative phase showed endothelial hyperplasia with 3H-thymidine incorporation (cell proliferation marker), subendothelial multi-laminated basement membranes formation, and were clinically characterized by rapid growth in early childhood. In the involution phase, hemangiomas showed histological fibrosis and fat deposition, low or absent 3H-thymidine cell aggregation, and clinical regression of the lesion. The endothelium of hemangiomas showed in the histology Weibel-Palade bodies, presence of alkaline phosphatase, and factor VIII production. On the other hand, they observed that vascular malformations revealed no incorporation of 3H-thymidine and maintained normal cellular structural characteristics.4
In 1996, the International Society for the Study of Vascular Anomalies (ISSVA) adopted the division of vascular anomalies into tumors and malformations, using this classification for over a decade.1,3
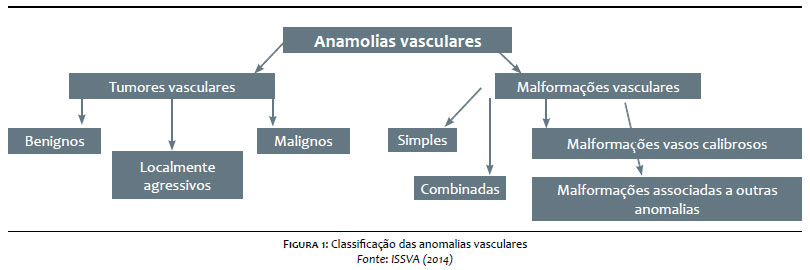
Starting in 2013, a group of ISSVA leaders sought to update the classification of vascular anomalies to describe new findings, including genetic and histological information. In 2014, this group added the description of diseases associated with vascular anomalies, such as Klippel-Trenaunay and Sturge-Weber Syndromes, for example.1 The classic names: capillary hemangioma, cavernous hemangioma, and tuberous hemangioma were abolished.2 Figure 1 summarizes the ISSVA classification adopted in 2014.
In 2018, ISSVA presented the evolution in the classification of these anomalies, with the identification of new genes implicated in some diseases (Chart 1).5
Also according to ISSVA, there are some provisionally unclassified vascular anomalies because they are not defined as tumors or malformations or because they have clinical and pathological characteristics still incompletely understood. Examples are: intramuscular hemangioma; angiokeratoma; sinusoidal hemangioma; acral arteriovenous tumor; multifocal lymphangioendotheliomatosis with thrombocytopenia/ cutaneovisceral angiomatosis with thrombocytopenia; PTEN harmatoma of soft tissue/ soft tissue angiomatosis; fibro-adipose vascular anomaly.5
It is essential to differentiate between malformations and vascular tumors that appear during childhood since the diagnosis can change the treatment direction and the outcome for the patient. It is also essential to know that vascular anomalies can have various effects on the child's psychosocial development because depending on their location, extent, and severity, it can cause significant aesthetic disfigurement.
Vascular tumors are neoplasms characterized by increased endothelial cell proliferation. Lesions usually overgrow, and most are not present at birth, following a phase of proliferation and subsequent involution. They can be classified as benign, locally aggressive, and malignant, based on cellular behavior.1
Infantile hemangioma, congenital hemangioma, tufted angioma, and pyogenic granuloma are examples of benign vascular tumors. Kaposiform hemangioendothelioma (KHE) exemplifies locally aggressive or borderline tumors. Angiosarcoma and epithelioid hemangioendothelioma, in turn, represent malignant vascular tumors, which we don't address here.1,2
Infantile hemangioma (IH) is the most common benign vascular tumor among children, with an incidence of 4% to 10%, most frequently observed in the cervicofacial region (80% of cases), in women, and in Caucasians.1,2 It may have superficial (telangiectatic macules and papules), deep (poorly delimited bluish nodules with fibroelastic consistency), or mixed components. In the first weeks of life, a phase of rapid growth is observed, up to eight to 12 months of age, when most IHs have reached their maximum growth. From then on, an involutive tumor phase begins, with color whitening and volume decrease. Approximately 20% to 50% of IHs involve leaving scarred areas with atrophy, hypopigmentation, fibrous adipose tissue, or residual telangiectasias.2
Immunohistochemistry is positive in all evolutionary stages of IH for GLUT-1, which is a glucose transporter generally expressed in brain microvascular endothelium, retina, endoneurium, and placenta, but it is not expressed in healthy skin. GLUT-1 positivity differentiates IH from vascular malformations and kaposiform hemangioendothelioma.2 The most studied cytokines involved in the pathogenesis of IH are VEGF, b-FGF, metalloproteinases (MMP) 2 and 9, insulin-like growth factor (IGF), osteoprotegerin, and angiotensin-converting enzyme.
Treatment consists of follow-up when the lesions are small and without associated complications, as most IHs spontaneously involve.
In most cases, topical treatment is preferred. Still, immediate systemic treatment should be instituted in cases of potentially disfiguring hemangiomas, in the presence of risk of functional sequelae, or risk of airway obstruction. In 2008, the use of systemic beta-blockers for the treatment of IH was introduced, and propranolol has since been described as the drug of choice for these tumors.2
Congenital hemangioma is a vascular tumor that is completely formed at birth and has no postnatal proliferation. It can be identified intrauterine by obstetric ultrasound, usually in the third trimester of pregnancy. It presents as solitary exophytic plaques or masses of violet color and telangiectatic surface and may have hypochromic areas in the center and periphery. Immunohistochemistry is negative for GLUT-1 in these tumors.2
According to natural history, it is classified as rapidly involuting, partially involuting, and non-involuting.1 The treatment of this hemangioma depends on its size, location, and presence or absence of associated complications, such as ulceration, bleeding, and pain. The application of pulsed dye laser can improve the superficial aspect of the lesion and has applicability in residual lesions of tumors that did not completely regress.2
Tufted angioma (TA) is a rare and benign vascular tumor, also known as Nakagawa's angioblastoma or progressive capillary hemangioma. It is most commonly located in the cervical region, shoulder, and upper trunk. Few cases are present at birth or associated with hyperhidrosis or hypertrichosis.1 It presents a risk of association with the Kasabach-Merritt phenomenon, in which severe thrombocytopenia with mild to moderate coagulopathy occurs. There are no effective treatments for TA, and the use of interferon alfa (IFN-alpha) and laser is described.2
Pyogenic granuloma is a common benign vascular tumor. Also described as lobular capillary hemangioma, most are acquired and manifest as an erythematous nodule or papule, usually with a scaly collar and bleeding surface. It can be localized in any region of skin and does not involve spontaneously. Therapeutic options include the use of topical timolol, electrocoagulation, laser, cryotherapy, and surgical exeresis.2
Kaposiform hemangioendothelioma (KHE) is a rare, locally aggressive vascular tumor. Some authors consider KHE and tufted angioma (TA) as spectra of the same disease.
KHE is present at birth or early in childhood and is more frequent in the trunk, extremities, and retroperitoneal region. Clinically, it is observed as an erythematous-brown macula or plaque that evolves into a poorly defined tumor of hard consistency, similar to tufted angioma. It is an immunohistochemical negative GLUT-1 tumor.2
Like TA, KHE is at risk of association with Kasabach-Merritt phenomenon.2
Vascular malformations are caused by an alteration in angiogenesis during the embryological period, presenting vascular ectasia with normal endothelial growth.1,6 They affect 0.3% to 0.5% of the population and are present at birth in 90% of cases. Also, they increase in length following the child's growth without spontaneous involution.1,2,6 Although usually sporadic, vascular malformations may be familial and genetically determined.6
In 2018, Al-Olabi et al. studied sporadic vascular malformations with excluded genetic causes, sequenced the DNA from the tissue of patients with vascular lesions, and found the presence of multiple mosaic-activating variants in four genes of the RAS/MAPK pathway (KRAS, NRAS, BRAF e MAP2K1), commonly activated in cancer cases. They then tested the use of vemurafenib, a BRAF inhibitor, in an animal model with mutations in this pathway, and observed improvement in vascular lesions and re-establishment of blood flow in arteriovenous malformations.7
Vascular malformations are divided into four groups: simple malformations, combined malformations, malformations of major named vessels, and malformations associated with other anomalies (bone, soft tissue, visceral).1
They are malformations composed of only one type of vessel: capillary, lymphatic or venous.
Capillary malformations consist of dilation of capillaries and/or postcapillary venules and mainly affect the skin and mucosa. They present from birth and generally persist throughout life. They may darken and become thicker as the child grows, manifest in isolation or be associated with increased soft and bone tissue.1,6
The Port-wine stain is a simple capillary congenital vascular malformation, usually of unilateral, segmental manifestation, without involution tendency.2,6 Also known as flame nevus, it is commonly mistakenly referred to as "flat hemangioma". It has no predilection for sex and is less frequent in Asian and African American populations. It is the second most common congenital vascular malformation in childhood, characterized by capillary and venous ectasia in the dermis, which results in increased hemoglobin in the skin, giving it a more reddish or purpuric pigmentation.8,9
The Port-wine stain originates from irregularities in neural development and genetic mutations, which may be familial or sporadic.6,8,9 It was recently associated with a mosaic mutation in GNAQ gene.2,5
Mutations in the expression of RASA 1 and vascular endothelial growth factor (VEGF) have also been implicated in the pathogenesis and progression of these lesions.5,10
In 1986, Smoller and Rosen documented a significant reduction in perivascular nerve fiber density in Port-wine stain compared to healthy skin.11 Because neural mechanisms regulate cutaneous vascular flow, changes in nerve distribution would affect the development of these lesions.8,9,11
They are often seen in the distribution of dermatomes, involving one or more branches of the trigeminal nerve, when located on the face.8,10
It presents as a pink, red or purplish-colored macula or plaque on the skin that progressively darkens if not treated early and becomes hypertrophic or nodular with age in approximately two-thirds of patients at 50 years of age.8,10
Although it can be located in any region of the body, the face and cervical region are the most affected areas, especially in the distribution of dermatomes V1 (upper third of the face, innervated by the ophthalmic branch of the trigeminal nerve) and V2 (centrofacial region, innervated by the maxillary branch of the trigeminal), and, when present in these topographies, causes marked disfigurement.1,2,8
Port-wine stains located on the face may be associated with changes such as jaw hypertrophy, increased lip volume, bite deformity, and spontaneous gingival bleeding.2
When located on the face and neck, these stains respond better to laser treatment compared to those in other body areas.12 The thicker lesions represent great therapeutic difficulty. Therefore, treatment should be conducted early, before thickening and as a way to prevent the development of psychosocial problems resulting from the functional or aesthetic impairment that the lesions cause.8,13
The possibility of recurrence or aggravation of capillary malformation even after its treatment should also be considered.
Michel et al. reported recurrence in 16.3% of patients with Port-wine stain treated with pulsed dye laser and noted that in children under 10 years of age there was no recurrence of the lesion.14
Port-wine stain manifests itself or in association with other changes, such as Sturge-Weber syndrome, Klippel-Trenaunay syndrome, and Proteus syndrome.2
Also known as nevus simplex, Unna nevus, nevus flammeus nuchae, "angel's kiss" (when located on the glabella), "stork bite" (in the occipital region), the salmon patch occurs in 50% of newborns.1,2
It most often affects the midline of the head on the forehead, eyelids, glabella, or neck. Most present lightening or disappear over time, usually before the age of five, but lesions may persist to adulthood in 50% of patients when located in the neck and sacral regions.1,2 It should be differentiated from the Port-wine stain, which tends to be more winemaking and unilateral.
Telangiectasias are small dilated vessels that manifest in childhood or puberty. Spider angioma, angioma serpiginosum, and unilateral nevoid telangiectasia are examples of primary telangiectasias.2
Lymphatic malformations (LM) consist of several lymphatic channels or dilated cysts, lined with endothelial cells with lymphatic phenotype.1 They may be primary or secondary, localized, or diffuse. They are classified as microcystic, macrocystic, or mixed.
Microcystic LM, or circumscribed lymphangioma, is composed of abnormal microscopic lymphatic vessels, characterized by plaques surmounted by clear or violaceous vesicles.
Macrocystic LM, also known as cystic hygroma, is usually seen at birth or until the second year of life. It presents as a soft, translucent cystic mass with healthy skin coating.
Mixed LMs are more common in the cephalic segment, particularly in the malar region and in the mouth, and may lead to macroglossia. LM treatment includes compression, sclerotherapy, surgical exeresis, and laser.2
Venous malformations (VM) are relatively rare congenital anomalies present at birth and not always evident.2 They usually manifest as blue-colored lesions, when superficial, or as compressible masses, which may increase with exercise. They are the most common type of low-flow vascular lesions and account for about two-thirds of congenital vascular malformations.1,2
They present as sporadic and solitary lesions in 90% of patients and as familial multifocal lesions in 10% of them. May be associated with bleeding, aesthetic impairment, and difficulty breathing or eating.15
Imaging such as ultrasound, Doppler flowmetry, and magnetic resonance imaging (MRI) help determine the extent of tissue involvement and differentiate between high and low flow lesions.16
Venous vascular malformations, in general, are not eradicated. Its usual treatment is sclerotherapy, using solutions such as alcohol 95% or sodium tetradecyl sulfate 1% for small lesions. Surgery may also be performed after obliteration through sclerotherapy. Although surgical excision is the definitive therapy, anatomical and functional limitations and the possibility of aesthetic impairment often hamper its performance.2
Malformations of major named vessels affect large-caliber veins, arteries, or vessels, usually axial. Congenital arteriovenous fistulas and persistent embryonic vessels are included in this group of malformations.1
Although they represent a significant clinical impact, they have few dermatological manifestations..
Combined vascular malformations associate two or more malformations in the same lesion. Examples are: capillary and venous malformations; capillary and lymphatic malformations; venous and lymphatic malformations; capillary, lymphatic and venous malformations; capillary, lymphatic, venous and arteriovenous malformations.5
Vascular malformations, whether simple, major named vessels, or combined, may be associated with bone, soft tissue, or visceral abnormalities.5
Chart 2 shows the principal syndromes of dermatological interest.
Although there are different therapeutic alternatives described for the treatment of cutaneous vascular malformations, such as percutaneous sclerosis, surgical resection, laser therapy, or a combination of them, there is not yet a method that guarantees the permanent cure of these lesions. Thus, their treatment is still a challenge to physicians.
The word "laser" is an acronym for Light Amplification by Stimulated Emission of Radiation.17 Its use in medicine began in the 1960s when Leon Goldman created the ruby laser to treat skin lesions.9
Before its use to treat cutaneous vascular malformations, local and systemic therapies were applied, such as hypertonic glucose injection, monoethanolamine oleate injection (Ethamolin, Farmoquímica S/A, Rio de Janeiro, Brazil) associated with glucose, morrhuate sodium injection, aethoxysklerol injection, ethanol injection, surgical excision, corticosteroid use, interferon, cryotherapy, arterial embolization, beta therapy, and bleomycin, with varied responses.16,18
Lasers and other light sources represent a breakthrough in dermatology for both cosmetic and non-cosmetic applications. They have been increasingly used to remove or lighten many vascular lesions that were once considered untreatable.13,19,20
The laser is considered the gold standard for treatment of cutaneous capillary malformation. However, its indication to treat hemangiomas remains controversial, and it is not recommended in arteriovenous malformations treatment.9,17,21
In the 1970s, the argon laser, which emits a continuous beam of blue-green light with wavelengths between 488nm and 514nm, was widely used to lighten cutaneous vascular lesions, but pigmentary changes and scarring were frequent due to the non-selective effects of this laser in the tissues.2,13,22
Ablative lasers such as carbon dioxide (CO2) 10,600nm and erbium:yttrium-aluminum-garnet (Er:YAG) 2,940nm lasers have also been used for this purpose. Although they did not reach the vessels, they aimed at destroying the lesion by absorbing laser energy by water from adjacent tissues. The 511nm and 578nm copper vapor laser represented an improvement over those already used. However, pulsed dye laser has replaced other lasers in the treatment of Port-wine stains.13
More recently, longer wavelength lasers - 755nm alexandrite laser; long pulse 1,064-nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser - have been used to treat vascular lesions with the advantage of deeper penetration in the skin.22
In 1983, Anderson and Parrish developed the theory of selective photothermolysis, allowing the understanding of the interaction between laser and treated tissue. The authors demonstrated that target chromophores selectively absorb specific wavelengths of light and produce thermal energy, enabling selective destruction of lesions with minimal damage to adjacent tissues.23
In vascular lesions, the target chromophores are oxyhemoglobin and deoxyhemoglobin, which absorb visible wavelengths of 400 to 780nm, with absorption peaks between 542 and 577nm.22
Port-wine stains were the most studied vascular malformations in laser therapy.13
Pulsed dye laser (PDL) emit lights of wavelengths between 585nm and 600nm and penetrate to a depth of up to 1.8mm.2 They were introduced in 1989 and revolutionized the therapy of cutaneous vascular lesions, becoming the method of choice for treating vascular malformations such as Port-wine stains.13,24,25 Its active medium is a fluorescent dye, which may be rhodamine 6G, fluorescein, coumarin, stilbene, umbeliferone, tetrazene, or malachite green.13
Older PDLs had a pulse duration of 0.45ms. Later models were developed with a longer pulse duration. Because they do not penetrate deep into the skin, their use became limited in the treatment of deeper localized lesions. Most patients require multiple sessions to improve Port-wine stains, yet not always achieving complete elimination of the lesion. Its main adverse event is the formation of purpura, which usually lasts between five and 14 days.13
There is a heterogeneity in the response of cutaneous vascular malformations to available therapies, and some factors that influence the unpredictability and resistance to pulsed dye laser treatment are described (Chart 3).10 Centrofacial lesions, located in the V2 dermatome pathway, have a lower response than those located in the upper and lower thirds of the face, corresponding to V1 and V3 dermatomes, respectively.10,26 Also, up to one-third of patients do not respond to treatment despite multiple sessions. Leg and hand lesions are less responsive to PDL treatment compared to facial injuries.13
The topical use of rapamycin and imiquimod showed antiangiogenic effects with encouraging results in improving the lightening of Port-wine stains when associated with pulsed dye laser.11
Cardoso et al. described, in 2006, the use of PDL to treat tufted angioma, which resulted in significant improvement of local pain and partial reduction of lesion size.27
In 2007, Chapas et al. first described the efficacy and safety of treating Port-wine stains with the high-energy pulsed dye laser in children under six months of age. Responses from 49 children submitted to 595nm V Beam® laser associated with dynamic cooling with cryogen tetrafluoroethane and energy ranging from 7.75 to 9.5J/cm2 were assessed. This study showed good laser tolerance without atrophy or residual skin scarring and demonstrated the importance of early initiation of treatment of these malformations.12 Bae et al. evaluated the outcome of the use of bipolar radiofrequency (RF) associated with pulsed dye laser and pointed out RF as an alternative for the treatment of Port-wine stains resistant to therapy with PDL alone in adults.28
The neodymium:yttrium-aluminum-garnet (Nd:YAG) laser has a wavelength of 1,064nm. It acts by selective photocoagulation, and its great advantage is the greater depth of tissue penetration when compared to other lasers in the treatment of vascular lesions. It can penetrate the skin up to 4mm to 6mm, and it is also used for the treatment of Port-wine stains. The laser energy is transmitted through the superficial tissue layers and distributed to the deepest layers.21
Long pulse or continuous Nd:YAG lasers have been the method of choice for the treatment of venous malformations due to the wide experience and good results of their use.15
Although most body tissues do not absorb this wavelength, pigmented tissues do absorb this wavelength better than unpigmented ones.25
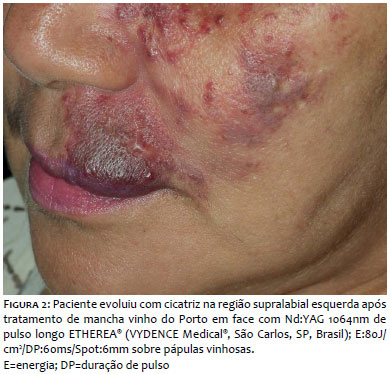
Also, though the Nd:YAG laser has been shown to be effective in treating deep vascular lesions, it should be considered that its use at fluences slightly above the minimum purpuric dose may lead to complications such as scarring and dyschromia.10,29
Figure 2 shows an example of scar formation after the use of long pulse 1064nm Nd:YAG in hypertrophic capillary malformation located in the upper left lip.
Alcántara-González et al. studied the efficacy and safety of using pulsed dye laser combined with Nd:YAG laser, showing good results in 30 patients aged 8 to 65 years who had mucous and cutaneous venous malformations.15
Van Drooge et al. presented, in 2013, the first case series showing the long-term effect of the long pulse 1.064nm Nd:YAG laser on the treatment of hypertrophic areas in Port-wine stains. When evaluating the outcome in 32 patients with a mean age of 51.4 years, followed after a mean of 37 months from the last laser treatment, they observed good and excellent response in 91% of the hypertrophic areas and 63% of color improvement of the lesions treated, with report of hypopigmentation and residual scar in seven and 14 participants, respectively.29
Liu et al. assessed the role of the long-pulse, high-energy 1.064nm Nd:YAG laser in the treatment of isolated PDL-resistant Port-wine stains in 20 patients aged 16 to 46 years. The authors observed lightening over 90% of the lesions in 20% of participants, suggesting that the long-pulse 1.064nm Nd:YAG laser may be promising in the treatment of capillary malformations non-responsive to PDL.30
In 2017, Murthy et al. studied the response of long-pulse Nd:YAG laser treatment to cutaneous vascular malformations excluding Port-wine stains and showed good to excellent results in 66.7% of the patients assessed, with a mean of 4.6 laser sessions per patient. Most lesions were located in the head and neck (48%) and extremities (31%). They concluded that the laser used in the study is a therapeutic option in the management of symptomatic and stigmatizing lesions resulting from vascular malformations in children and adolescents.31
A prospective controlled study that sought to investigate the efficacy and safety of double wavelength laser (595nm pulsed dye laser + 1.064nm Nd:YAG laser) in the treatment of Port-wine stains showed no significant difference in outcome compared to treatment with pulsed dye laser alone.32
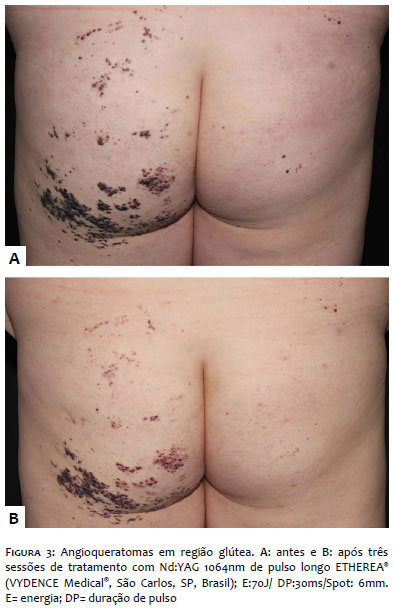
Nd:YAG laser has also been used to treat angiokeratomas.33 Figure 3 shows satisfactory response of lesions located on the buttocks, with reduced bleeding and local infections and consequent improvement in the patient's quality of life.
The potassium-titanyl-phosphate (KTP) laser uses a 1.064nm Nd:YAG laser source, whose frequency is doubled using a KTP crystal, producing 532nm wavelength green light.2,10 KTP has already been used to treat vascular lesions with good results.2,21
A study comparing PDL with KTP laser found that it left less purpuric lesion immediately after treatment, although patients reported higher pain intensity with KTP.10
Kwiek et al. evaluated the response based on comparing three-dimensional photographs of 44 patients with facial capillary malformations treated with doubled frequency 532nm Nd:YAG laser (KTP) and concluded that 77.3% of them had at least a 50% improvement in lesion lightening, with a mean of 7.1 sessions per patient.21
Intense pulsed light (IPL) is a non-coherent, high-intensity, polychromatic light source that emits light in a spectrum spanning 400nm to 1,200 nm wavelengths.13 It resembles the laser by the mechanism of action based on selective photothermolysis but differs from it by the possibility of selecting pulse duration and wavelength using filters.
IPL is an effective treatment modality for a growing range of dermatological diseases, and it may represent a treatment of choice in some situations.34
In the pediatric population, different vascular lesions have been treated with IPL, including Port-wine stains.21,25 Greater variability in pulse duration and fluency makes IPL useful in treating vessels of varying diameter and depth.10
In 2014, Adatto et al. studied the response of IPL in the treatment of Port-wine stains in 18 participants with Fitzpatrick skin phototypes to IV and a mean age of 32.1 years. The treatment was performed with two-wavelength tip: 500nm to 670nm and 870nm to 1200nm (LuxGTM; Palomar Medical Technologies, Inc., Burlington, MA, USA) to achieve higher vessel specificity and avoid absorption by melanin. Response analysis was based on qualitative (subjective improvement scale, based on comparison of patient photographic records) and quantitative (erythema and pigmentation measurements in treated lesions using the photometric scale using DermaType TM; Palomar Medical; Technologies, Inc.) evaluations. The study showed efficacy and safety of the IPL use in the treatment of Port-wine stains in various anatomical locations, with minimal adverse events: transient pain, erythema, scabbing, and purpura.35
Campolmi et al. describe in 2011 the efficacy of the IPL use in the treatment of vascular lesions, solar lentigos, and actinic keratoses in 85 patients and concluded that IPL is an effective and safe measure for the treatment of these lesions, with better results observed in patients with Fitzpatrick skin phototypes I and II.36
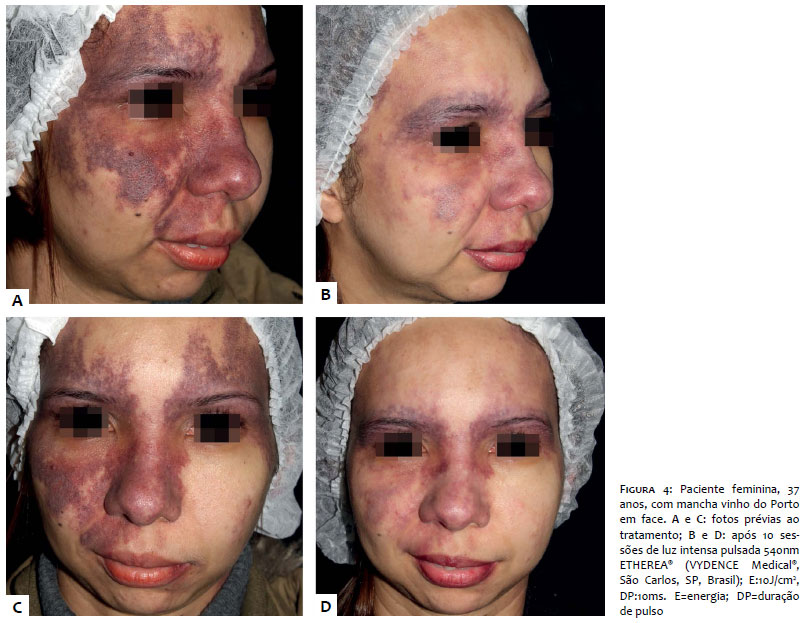
Evidence suggest that IPL is a safe and effective modality for the treatment of capillary malformations. It may be especially useful for darker, more vascularized areas, but with minimal or absent nodular lesions.34 Figure 4 shows good results obtained with the use of IPL in the treatment of Port-wine stain located on the face.
Faurschou et al. included, in a 2011 review, five randomized controlled trials involving patients with Port-wine stain to assess efficacy, adverse events, and satisfaction of participants after treatment with pulsed dye laser (PDL), long pulse Nd:YAG laser, and intense pulsed light (IPL). All studies showed lightening of lesions within three months of treatment. Adverse events described included pain, edema, hypo and hyperpigmentation, scabbing, blistering, hypertrophic scarring, and pyogenic granuloma. Participants preferred the PDL over the IPL result. It was also observed preference to the Nd:YAG laser when compared with the PDL, considering the shorter purpura duration time; PDL associated with cooling was preferred to PDL alone.22
Although laser and other light sources represent effective measures in the treatment of cutaneous vascular malformations, some care must be taken to avoid undesirable effects with their use. Table 4 presents measures to be adopted to reduce the risk of laser and intense pulsed light complications, based on the literature and clinical practice.37
Photodynamic therapy (PDT) is a photochemical reaction between a light source and a photosensitizing drug that produces reactive oxygen species (ROS) and induces cell death. Its first use was directed to the treatment of non-melanoma skin cancer and preneoplastic skin lesions. Some studies have shown that PDT can cause endothelial injury, vasoconstriction, thrombus formation, and blood flow stasis.10
In 2011, Xiao et al. assessed the outcome and complications of photodynamic therapy following intravenous use of hematoporphyrin monomethyl ether (HMME) photosensitizer followed by the application of a copper vapor laser on Port-wine stains in 507 Chinese participants. This study showed that in 29.8% of cases there was lightening higher than 50% in the treated lesions and 10% of participants had complications such as blistering, scabbing, eczema, hypo and hyperpigmentation, and photoallergy. The authors suggest PDT as a therapeutic option for Port-wine stains, especially in patients with high Fitzpatrick skin phototype and nodular vascular lesions.38
Although the role of PDT in vascular malformations treatment has been studied, its efficacy and safety have not been well established for this purpose.
The identification of somatic mutations in vascular anomalies is changing the understanding of these lesions, with potential targets for new pharmacotherapies being discovered.39
Vascular anomalies have a significant physical and psychological impact on patients. Knowledge of their characteristics and classifications is essential to establish the correct diagnosis and initiate appropriate and early treatment, resulting in a better quality of life for patients. Psychological damage can be avoided if treatment is instituted before school age and before the onset of interaction with other children. With the introduction of laser use and the understanding of selective photothermolysis, there has been a considerable advance in dermatological therapy, especially with the use of pulsed dye laser for capillary malformations. Although numerous treatment options for vascular anomalies are available, and many have been investigated in the literature, therapeutic decision-making is still mainly based on expert opinion. In a not too distant future, we expect these cases to be conducted more successfully, with the use of different combinations of laser and other light sources, alone or in association with antiangiogenic agents and, promisingly, gene therapy when needed and well indicated.
Ludmilla Cardoso Gomes | 0000-0002-8165-5345
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Abes Mahmed Amed Filho | 0000-0002-2847-6030
Preparation and writing of the manuscript; critical revision of the manuscript.
Mariana Figueiroa Careta | 0000-0002-5565-4859
Approval of the final version of the manuscript; critical revision of the manuscript.
Isabelle I Hue Wu | 0000-0003-4436-7237
Critical revision of the manuscript.
Vivian Barzi Loureiro | 0000-0002-0862-5959
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Luis Antonio Ribeiro Torezan | 0000-0003-0482-6515
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Wassef M, Blei F, Adams D, Alomari A, Baselga E, Berenstein A, et al. Vascular anomalies classification: recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics. 2015;136(1): e203-14.
2. Belda Júnior W, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 3rd ed. São Paulo: Editora Atheneu; 2018. p.2291-2316
3. Hassanein AH, Mulliken JB, Fishman SJ, Greene AK. Evaluation of terminology for vascular anomalies in current literature. Plast Reconstr Surg. 2011; 127(1):347-51.
4. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982;69(3):412-422.
5. International Society for the study of vascular anomalies. ISSVA Classification of Vascular Anomalies [Internet]. Melbourne: International Society for the Study of Vascular Anomalies; 2018 [cited 2019 Jun 18]. Available from: www.issva.org/classification.
6. Gontijo B, Pereira LB, Silva CMR. Vascular malformations. An Bras Dermatol 2004; 79(1):7-25.
7. Al-Olabi L, Polubothu S, Dowsett K, Andrews KA, Stadnik P, Joseph AP, et al. Mosaic RAS/MAPK variants cause sporadic vascular malformations which respond to targeted therapy. J Clin Invest. 2018;128(4):1496-1508.
8. Updike KM, Khachemoune A. Port-wine stains: A focused review on their management. J Drugs Dermatol. 2017;16(11):1145-51.
9. Stier MF, Glick SA, Hirsch RJ. Laser treatment of pediatric vascular lesions: Port wine stains and hemangiomas. J Am Acad Dermatol. 2008;58(2):261-85.
10. Savas JA, Ledon JA, Franca K, Chacon A, Nouri K. Pulsed dye laser resistant port-wine stains: mechanisms of resistance and implications for treatment. Br J Dermatol. 2013;168(5):941-53.
11. Smoller BR, Rosen S. Port-wine stains. A disease of altered neural modulation of blood vessels? Arch Dermatol 1986;122(2):177-9.
12. Chapas AM, Eickhorst K, Geronemus RG. Efficacy of Early Treatment of Facial Port Wine Stains in Newborns: A Review of 49 Cases. Lasers in Surgery and Medicine. 2007;39:563–568.
13. Schmults CD. Laser Treatment of Vascular Lesions. Dermatol Clin. 2005; 23(4):745-55.
14. Michel S, Landthaler M, Hohenleutner U. Recurrence of port-wine stains after treatment with the flashlamp-pumped pulsed dye laser. Br J Dermatol. 2000;143(6):1230-4.
15. Alcántara-González J, Boixeda P, Pérez-García B, Truchuelo-Díez MT, González-Muñoz P, Jaén-Olasolo P. Venous malformations treated with dual wavelength 595 and 1064 nm laser system. J Eur Acad Dermatol Venereol. 2013; 27(6):727-33.
16. Judith N, Ulrike E, Siegmar R, Matthias N, Jürgen H. Current concepts in diagnosis and treatment of venous malformations. J Craniomaxillofac Surg. 2014;42(7):1300-4.
17. Labau D, Cadic P, Ouroussoff G, Ligeron C, Laroche JP, Guillot B, et al. Therapeutic indications for percutaneous laser in patients with vascular malformations and tumors. J Mal Vasc. 2014;39(6):363-72.
18. Garzon MC, Huang JT, Enjolras O, Frieden IJ. Vascular malformation: Part I. J Am Acad Dermatol. 2007;56(3):353-70.
19. Shofner JD, Lipworth A, Tannous Z, Avram MM. When Not to Treat Cutaneous Vascular Lesions With the Pulsed Dye Laser. Lasers Surg Med. 2011; 43(8):792-6.
20. Kalil CLPV, Curcio BL, Cignachi S. Laser Nd: YAG and intense pulsed light in the treatment of port-wine stain: case report and review of literature. Surg Cosmet Dermatol. 2009;1(2):95-8.
21. Kwiek B, Rozalski M, Kowalewski C, Ambroziak M. Retrospective Single Center Study of the Efficacy of Large Spot 532nm Laser for the Treatment of Facial Capillary Malformations in 44 Patients With the Use of Three-Dimensional Image Analysis. Lasers Surg Med. 2017;49(8):743-9.
22. Faurschou A, Olesen AB, Leonardi-Bee J, Haedersdal M. Lasers or light sources for treating port-wine stains. Cochrane Database Syst Rev. 2011; (11):CD007152.
23. Anderson RR, Parrish JA. Selective Photothermolysis: Precise Microsurgery by Selective Absorption of Pulsed Radiation. Science. 1983;220(4596):524-7.
24. Dummer R, Graf P. Treatment of Cutaneous Vascular Lesions with the Variable Pulse Widht Frequency Doubled Neodymium:YAG Laser. Med Laser Appl. 2001; 16(4):277-82.
25. Athavale SM, Ries WR, Carniol PJ. Laser Treatment of Cutaneous Vascular Lesions. Facial Plast Surg Clin N Am. 2011; 19(2):303-12.
26. Renfro L, Geronemus RG. Anatomical differences of port-wine stains in response to treatment with the pulsed dye laser. Arch Dermatol. 1993; 129(2): 182-8.
27. Cardoso AEO, Tayti T, Oliveira JP, Torezan LA, Sotto MN, Vilela MA, et al. Tufted angioma: a case report treated with pulsed-dye laser. An Bras Dermatol. 2006;81(5 Supl 3):S273-6.
28. Bae YC, Alabdulrazzaq H, Brauer JA, Geronemus RG. Treatment of recalcitrant port-wine stains (PWS) using a combined pulsed dye laser (PDL) and radiofrequency (RF) energy device. J Am Acad Dermatol. 2017;76(2):321-6.
29. van Drooge AM, Bosveld B, van der Veen JP, de Rie MA, Wolkerstorfer A. Long-pulsed 1064 nm Nd:YAG laser improves hypertrophic port-wine stains. J Eur Acad Dermatol Venereol. 2013; 27(11):1381-6.
30. Liu S, Yang C, Yang S. Long-pulsed 1,064-nm high-energy dye laser improves resistant port wine stains: 20 report cases. Lasers Med Sci. 2012;27(6):1225-7.
31. Murthy MD, Dawson A, Gupta D, Spring S, Cordoro KM. Utility and tolerability of the long-pulsed 1064-nm neodymium: yttrium-aluminum-garnet (LP Nd:YAG) laser for treatment of symptomatic or disfiguring vascular malformations in children and adolescents. J Am Acad Dermatol. 2017;77(3)473-9.
32. Wang T, Chen D, Yang J, Ma G, Yu W, Lin X.Safety and efficacy of dual-wavelength laser (1064 + 595 nm) for treatment of non-treated port-wine stains. J Eur Acad Dermatol Venereol. 2018; 32(2):260-4.
33. Kutlubay Z, Gökler G, Küçüktas M, Engin B, Serdaroglu S. A case of solitary angiokeratoma successfully treated with a 1064-nm long-pulsed Nd:YAG laser. J Cosmet Laser Ther. 2015; 17(2):93-5.
34. Wat H, Wu DC, Rao J, Goldman MP. Application of intense pulsed light in the treatment of dermatologic disease: a systematic review. Dermatol Surg. 2014; 40(4):359-77.
35. Adatto MA, Luc-Levy J, Mordon S. Efficacy of a novel intense pulsed light system for the treatment of port wine stains. J Cosmet Laser Ther. 2010;12(2):54-60.
36. Campolmi P, Bonan P, Cannarozzo G, Bruscino N, Troiano M, Prignano F, et al. Intense pulsed light in the treatment of non-aesthetic facial and neck vascular lesions: report of 85 cases. J Eur Acad Dermatol Venereol 2011;25(1):68-73.
37. Wanner M, Sakamoto FH, Avram MM, Anderson RR. Immediate skin responses to laser and light treatments: Warning endpoints: How to avoid side effects. J Am Acad Dermatol. 2016;74(5):807-20.
38. Xiao Q, Li Q, Yuan KH, Cheng B. Photodynamic therapy of port-wine stains: long-term efficacy and complication in Chinese patients. J Dermatol. 2011; 38(12):1146-52.
39. Greene AK, Goss JA. Vascular Anomalies: From a Clinicohistologic to a Genetic Framework. Plast Reconstr Surg. 2018; 141(5):709e-17e.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}