


Giovanna de Araujo Horcel; Juliana da Silva Milhomem; Camila Crosara; Adriane Volkmann; Samuel Henrique Mandelbaum
Received on: 31/07/2018
Approved on: 06/03/2019
This study was performed at the Department of Dermatology of the Santa Casa de São José dos Campos, São José dos Campos (SP), Brazil.
Financial support: None
Conflict of interests: None
Malignant melanoma is a melanocyte tumor responsible for more than 75% of skin cancer deaths. The rare variants of this pathology are responsible for 5% of the cases and may mimic other pathologies. We report the case of a patient with spitzoid melanoma and we discuss the dermoscopic, histopathological, and immunohistochemical findings, as well as the follow-up of this rare variant of melanoma.
Keywords: Melanoma; Nevus, epithelioid and spindle cell; Melanoma-specific antigens; Skin neoplasms; Dermoscopy
Corresponding to less than 5% of all melanomas, rare histological variants may mimic other malignant tumors,1,2 which often makes early diagnosis difficult.
The spitzoid variant of melanoma is rare and underdiagnosed due to its unusual clinical appearance and lack of pigment. Sometimes, definitive diagnosis can only be established after the onset of metastases.3
A 52-year-old female patient was referred to the care of the authors of the present article due to the presence of an asymptomatic violaceous lesion in her left thigh that had emerged two years before. The patient had Fitzpatrick IV phototype, and fibromyalgia and rheumatoid arthritis history, in addition to an intermittent and significant sun exposure without photoprotection throughout her life.
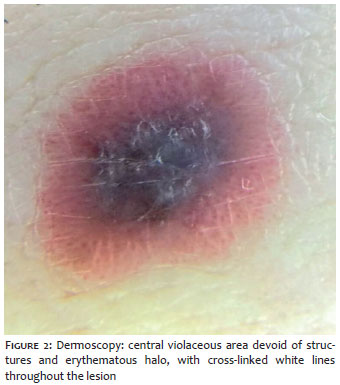
Dermatological examination revealed a well-defined erythematous papule with a violaceous center, measuring 1cm in its longest diameter (Figure 1). Dermoscopic analysis showed a central violaceous area devoid of structures, with white reticulated lines with erythematous interior and halo interspersed by red dots (Figure 2).
Diagnostic hypotheses of hemosiderotic dermatofibroma, thrombosed angiokeratoma and amelanotic melanoma were raised.
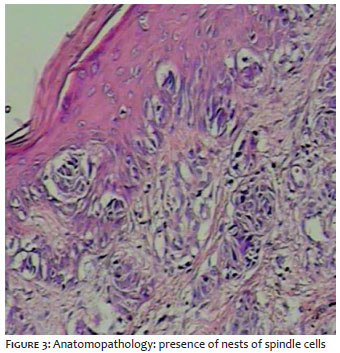
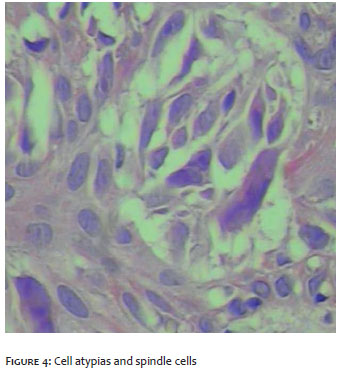
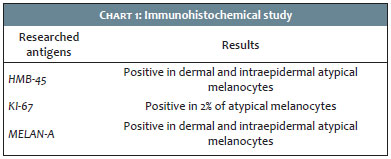
The authors of the present article chose to perform an excisional biopsy with pathological examination of the material, which suggested the presence of a spitzoid subtype of invasive malignant melanoma in its vertical growth phase, Clark level IV, Breslow thickness 1,1mm and 1 mitosis/mm2, without perineural or perivascular involvement. The presence of pagetoid ascension (Figure 3) and spindle cells nests (Figure 4) was key for this difficult diagnosis. The pathologist physician suggested the performance of an immunohistochemical study for diagnostic complementation. The results can be seen on Chart 1.
After the surgical margins were widened (2cm) according to protocols recommended by the Melanoma Brazilian Group (GBM), the patient was referred to the oncological surgeon for sentinel lymph node biopsy, with negative outcome.
The patient is currently being periodically followed-up by Dermatology and Oncology teams.
Spitzoid melanoma occurs more frequently in the head and extremities, and shares many clinical and histopathological similarities with the Spitz nevus. 3, 4, 5 Papagiorgiou et al. consider that young age is an important diagnostic clue for the spitzoid subtype, a factor that has not been demonstrated in the present case report. 6
Spitzoid melanomas often have the clinical appearance of amelanotic nodules, with crusts and ulceration, and have the following characteristics as differential diagnosis: hemangioma, pyogenic granuloma, xanthogranuloma and basal cell carcinoma.4
Although the clinical diagnosis is more difficult due to lack of pigment, the study by Semkova K et al. found no difference in mortality rates between melanoma and its spitzoid subtype.7
One of the greatest difficulties for the pathologist physician is the differentiation between Spitz nevus and spitzoid melanoma. Characteristics that corroborate the diagnosis of spitzoid melanoma include: size in excess of 1cm, ulceration, deep dermal penetration, asymmetry, lack of circumscription, absence of Kamino bodies, high degree of cytological atypia and of mitotic rate.8, 9 Most of these criteria could be observed in the case described by the present paper.
In cases of atypical histopathologic characteristics, immunohistochemical analysis is crucial. In the present case, the authors investigated HMB-45, KI-67 and Melan-A. The Melan-A antigen peptide is one of the most studied, and is expressed in healthy melanocytes and melanomas. It is most commonly used in addition to the S-100 protein and the HMB-45 dye, for the immunohistochemical identification of malignant melanoma. 10 In face of this immunohistochemical profile, associated with the clinical-pathological findings, it is possible to determine whether the lesion is a spitzoid variant melanoma.
Although some studies have demonstrated the importance of the CD99 marker in the differentiation between Spitz nevus and spitzoid melanoma, this research was not used in the present case report. 11
The histopathological diagnosis of the described case was established by an experienced dermatopathologist physician.
Identifying this rare melanoma subtype of atypical morphology is crucial due to the high mortality rate associated with the disease.
When anatomopathological analysis is not enough to reach clear diagnosis, immunohistochemical methods are an important tool for diagnostic assistance.
Long-term follow-up of the patient is instrumental for conducting studies on the prognosis associated with this atypical morphology.
Giovanna de Araujo Horcel | ORCID 0000-0002-8739-3462
Study design and planning; manuscript preparation and drafting; data collection, analysis and interpretation.
Juliana da Silva Milhomem | ORCID 0000-0002-1514-4117
Preparation and drafting of the manuscript.
Camila Crosara | ORCID 0000-0002-3457-1640
Preparation and drafting of the manuscript.
Adriane Volkmann | ORCID 0000-0002-7182-5507
Intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied; critical review of the manuscript.
Samuel Henrique Mandelbaum | ORCID 0000-0002-4631-4828
Approval of the final version of the manuscript.
1. Zacharias DPM, Santos IDAO. Melanoma cutâneo. In: Mélega JM. Cirurgia plástica fundamentos e arte: princípios gerais. Rio de Janeiro: Guanabara Koogan; 2009. p.361-70.
2. Araujo IC, Coelho CMS, Salida GAM, Lana PC, Almeida ACM, Pereira NA, et al. Melanoma cutâneo: aspectos clínicos, epidemiológicos e anatomopatológicos de um centro de formação em Belo Horizonte. Rev Bras Cir Plast. 2014;29(4):497-503.
3. Kim HY, Yoon JH, Cho EB, Park EJ, Kim KH, Kim KJ. A Case of Spitzoid Melanoma. Ann Dermatol. 2015;27(2):206-9.
4. Kim JY, Choi JE, Ahn HH, Kye YC, Sei SH. A case of spitzoid melanoma with lymph node metastasis in a child. J Korean Med Sei. 2012;27(4):454-7.
5. Kamino H. Spitzoid melanoma. Clin Dermatol. 2009;27(6):545-55.
6. Papageorgiou V, Apalla Z, Sotiriou E, Papageorgiou C, Lazaridou E, Vakirlis S, et al. The limitations of dermoscopy: false-positive and false-negative tumours. J Eur Acad Dermatol Venereol. 2018;32(6):879-88.
7. Semkova K, Lott JP, Lazova R. Clinicopathologic features and survival in Spitzoi malignant melanoma and conventional malignant melanoma. J Am Acad Dermatol. 2014;71(3):516-20.
8. Crotty KA, Scolyer RA, Li L, Palmer AA, Wang L, McCarthy SW. Spitz naevus versus Spitzoid melanoma: when and how can they be distinguished? Pathology. 2002; 34(1):6-12.
9. Requena C, Botella R, Nagore E, Sanmartín O, Llombart B, Serra-Guillén C, et al. Characteristics of spitzoid melanoma and clues for differential diagnosis with spitz nevus. Am J Dermatopathol 2012;34(5):478-86.
10. Wiltz K, Quereshi H, Patterson J, Mayes DC, Wick MR. Immunostaining for MART-1 in the interpretation of problematic intra-epidermal pigmented lesions. J Cutan Pathol. 2007;34(8):601-5.
11. King MS, Porchia SJ, Hiatt KM. Differentiating spitzoid melanomas from Spitz nevi through CD99 expression. J Cutan Pathol. 2007;34(7):576-80.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}