


Gabriela Momente Miquelin; Mariana Morais Tavares Colferai; Denise Steiner
Received on: 12/04/2019
Approved on: 15/05/2019
Study conducted at Department of Dermatology of the Universidade de Mogi das Cruzes, Mogi das Cruzes (SP), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Vitiligo is a chronic acquired skin disease, which evolves with depigmentation. The control of disease activity is a therapeutic challenge. Systemic corticosteroids, in daily use or in pulse doses, are the most used treatment for the disease.
OBJECTIVE: To evaluate the effect of minocycline on the control over vitiligo activity compared with the corticosteroid therapy.
METHODS: Randomized clinical trial with 16 active vitiligo vulgaris patients, divided into two groups: MINO group: minocycline 100mg/day, orally, for three months; and CORT group: prednisolone 0.3mg/kg/day, orally, for two months, and 0.15 mg/kg/day in the third month. The patients were evaluated before and after the treatment by photographic records and evaluation of the scores obtained by the VIDA score (vitiligo disease activity score).
RESULTS: According to the photographic records, there was control of vitiligo activity in 100% of patients in the MINO group compared with 60% in the CORT group. In the comparison using the VIDA score, we noticed a statistically significant diference for both groups; however, we found that the reduction was greater in the MINO group, evidencing more effectiveness of minocycline in controlling the vitiligo activity.
CONCLUSION: This study demonstrated the efficacy of minocycline in the control of active vitiligo compared with a systemic corticosteroid regimen. Additional studies should be performed to confirm its efficacy.
Keywords: Vitiligo; Minocycline; Prednisolone
Vitiligo is a chronic acquired skin disease that evolves with depigmentation of the skin,1 2 with no difference between race, gender or age.3,4,5 The mean age of the disease onset is around 20 years.1
The clinical manifestations include achromic macules that initially may appear hypochromic, surrounded by skin with healthy or discreetly erythematous/ hyperchromic aspect. They usually occur in photoexposed areas such as the face, back of the hands, upper thorax and periorificial regions, as well as in hairs (leukotrichia), mainly pubic hair, eyebrows, and eyelashes.1,3,4,6 The lesions tend to exhibit centrifugal growth and can affect any skin site, including mucous membranes. Local trauma (acute or chronic) can trigger the onset of vitiligo characteristic lesions on the skin that has not previously been affected (isomorphic phenomenon of Köebner).3,6
The exact etiology is still not clearly defined, but it is believed in the influence of immunological, neurological, biochemical and genetic factors, with emphasis on the latest advances in genomic studies.3,4,7,8,9
It is important to assess whether vitiligo is stable or progressive since management strategies differ in each case. The vitiligo is considered stable when it presents no progression for a period of one year or more 10,11 and, if the disease presents evolution, it is considered active. However, there are controversies according to the reference consulted.
The treatment of vitiligo should be individualized, depending on the extent and evolution of the condition and on the disease activity.
The available information on systemic vitiligo treatment is limited.12 Recently, epidermal oxidative stress has been documented in patients with vitiligo, postulating that free radical-mediated damage acts as an initial pathogenic event in the degeneration of melanocytes.13
As one of the possible forms of systemic treatment currently under study, minocycline, an antimicrobial of the class of tetracyclines, presents anti-inflammatory and antioxidant effects in addition to its already well-established antimicrobial action.14 Its mechanism of action has not been completely elucidated, but it involves inhibition of free radicals and production of cytokines, interference in protein synthesis, modulation of metalloproteinases action, and antiapoptotic action. There is evidence regarding the safety and efficacy of its use at the dose of 100 mg/day for three months.14
In one study, Song et al.15 demonstrated that minocycline may spare melanocytes from oxidative stress in vitro. This study concluded that this drug protects melanocytes against apoptosis induced by H2 O2 (hydrogen peroxide) in vitro. 15
In a prospective study involving 32 patients, Parsad and Kanwar 14 showed the efficacy of minocycline at the dose of 100 mg/day in controlling vitiligo disease activity. A more recent prospective study involving 50 patients concluded that dexamethasone in oral minipulse therapy (OMT) and oral minocycline are effective drugs to control vitiligo activity. 13
In fact, topical and systemic corticosteroids are currently the standard treatment for active vitiligo. Corticosteroids administered systemically, daily or in the form of pulses, are efficient in controlling the disease activity.16 Its use is based on the physiopathogenic theory of vitiligo autoimmunity,17 and several studies demonstrate its effectiveness.16,18,19,20,21,22
However, the administration of systemic corticosteroids for prolonged periods may cause unacceptable adverse events. In patients with extensive or rapidly expanding vitiligo, Pasricha and Khaitan16 reported that oral minipulse therapy with betamethasone has minimized adverse events. With the administration of a single dose of betamethasone/dexamethasone 5 mg orally after breakfast on two consecutive days per week, the authors reported 80% repigmentation and control of disease progression in 89% of 40 vitiligo patients, without serious adverse events.16,21
Other studies have shown the efficacy of low dose oral prednisolone in controlling vitiligo activity. Using daily doses of oral prednisolone of 0.3 mg/kg body weight, long-term treatment was possible, and adverse events were kept to a minimum.18,21
The objective of this randomized, open-label clinical trial in patients with clinical diagnosis of active vitiligo vulgaris was to compare the effect of minocycline on vitiligo activity with the conventional treatment, which is systemic corticosteroid.
First used in the study by Njoo et al. in 1999,11 the vitiligo disease activity score (VIDA) consists of a scale that considers the presence of new lesions and/or the expansion of existing lesions and the period of evolution. Based on the patient's own reports, the VIDA score consists of a total of six points: VIDA score +4: activity lasting six weeks or less; score +3: activity lasting from six weeks to three months; score +2: activity lasting from three to six months; score +1: activity lasting from six to 12 months; score 0: stable disease for one year or more; score -1: stable disease with spontaneous repigmentation for one year or more. Lower VIDA score indicates less vitiligo activity.10
Twenty-five patients were invited to participate in the study. Of these, 16 presented the eligibility criteria and were included. The study elected men and women between 14 and 65 years old with clinical diagnosis of active vitiligo vulgaris, defined as a vitiligo disease activity score (VIDA11) of +3/+4; regardless of the duration of prior therapy, who were able and willing to comply with all scheduling and visiting, treatment, and evaluation requirements, and were also able to understand and provide the informed consent.
None of the patients presented a history of decompensated comorbidity; immunosuppression; abnormal photosensitivity; active cancer; current infection; collagenosis; and benign intracranial hypertension (pseudotumor cerebri). Pregnant women, nursing mothers, and women who intend to become pregnant during the course of the study were excluded; as well as patients on immunosuppressive drugs; concomitant use of other antimicrobials or who have shown hypersensitivity to tetracyclines.23 Patients participating in other studies involving drugs or other devices in the three months prior to or during enrollment in this study were not admitted.
We conducted the history and clinical examination, including information such as age at vitiligo onset, duration of the disease, presence of family history or any other associated disease, triggering factors (emotional, physical or medication), evaluation of the percentage of the affected body surface, and presence of mucous membranes and hairs involvement.
Patients who received topical or systemic therapy for vitiligo were given a washout period of two and four weeks, respectively, before inclusion in the study.
This study protocol was submitted and approved by the Committee for Ethics in Research of the University of Mogi das Cruzes (SP) (CAAE 57065116.0.0000.5497).
Randomization and intervention
Randomly, the 16 patients selected were assigned to one of the two treatment groups, 11 for the MINO Group and five for the CORT Group, defined as:
MINO Group - Patients receiving minocycline 100 mg/day, orally, for three months.
CORT Group - Patients receiving prednisolone 0.3 mg/kg/day, orally, for two months, and 0.15 mg/kg/day in the third month of treatment.
No topical or phototherapy was allowed during the study period.
The patients were followed up for three months and were evaluated at baseline, after four weeks, to check adherence to the treatment, and after 12 weeks.
At baseline and at the end of the treatment, after 12 weeks, photographic records were made in the studio, with a Lumix Panasonic camera, with entire body images of the patients under study and of each vitiligo lesion.
The endpoints assessed were:
1) Assessment of disease activity, from the objective judgment of comparative pre and post-treatment photographic records, by two blinded medical examiners, to determine the stabilization or not after one of the treatments. The agreement test between the two experts showed no difference in terms of results.
Each isolated lesion was assessed in terms of its expansion and skin presentation in an overall way regarding the appearance of new lesions, classified as: - Stable, for stabilization of vitiligo; and – Unstable, for absence of stabilization. Also, the presence or absence of repigmentation in the study groups was evaluated;
2) Assessment of disease activity based on patients' reports, using the VIDA11 questionnaire applied at baseline and at the 12th -week post-treatment.
Data analysis methodology
The following tests were used in the statistical analysis of the results: Wilcoxon test, Mann-Whitney test, Test for the Equality of Two Proportions, Fisher Exact Test, Confidence Interval for the Mean, P-value. We chose to use non-parametric tests since the data set had a low sampling rate (less than 30 subjects). In this statistical analysis, we used the software: SPSS V20, Minitab 16 and Excel Office 2010.24, 25, 26
Of the 16 patients selected for the study, the total number of individuals who completed the proposed treatment for the MINO Group was 11 patients; and, for the CORT Group, five patients. A subject who has completed the study is defined as a patient enrolled in accordance with the inclusion/ exclusion criteria and who attended the initial visit, the follow-up visit, and the visit immediately after the end of the treatment.
A significance level of 0.05 (5%) was defined for this study. All confidence intervals throughout the study were constructed with 95% statistical confidence.
The mean age of patients in the MINO Group was 42.6 years and in the CORT Group was 36.4 years. It was found that in both groups the age variability was low because the coefficient of variation was less than 50%, demonstrating that the data are homogeneous.
The percentage distribution of men and women between the study groups was: 81.8% of women and 18.2% of men in the MINO Group; 60% of women and 40% of men in the CORT Group.
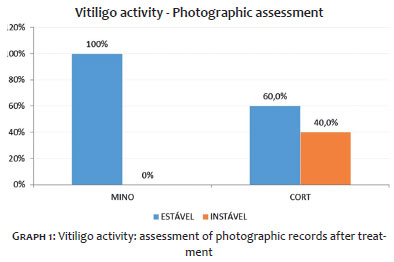
After three months of treatment, by analyzing the pre and post-treatment comparative photographic records, conducted by two blind medical examiners, we verified that there was control of vitiligo activity in 100% of patient in the MINO Group. In the CORT Group, 60% of the patients evolved with activity control (Chart 1).
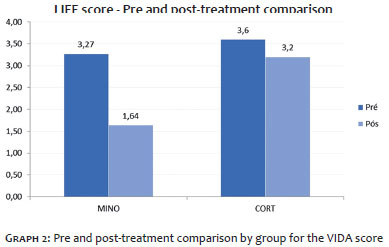
Regarding the analysis of the VIDA score, a statistically significant difference was observed for both groups regarding the control of vitiligo when the moments before and after treatment were compared. In the MINO Group, the mean score was reduced from 3.27 to 1.64 (p-value=0.002), while in the CORT Group it decreased from 3.60 to 3.20 (p-value=0.157) (Chart 2). This analysis was performed by group, using the Wilcoxon test.
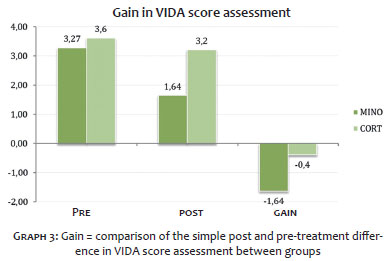
We also analyzed the groups in the gain, i.e., in the simple difference between the mean of the results of post minus pre-treatment of the VIDA questionnaire data, using the Mann-Whitney test and concluding that there was a statistically significant difference between the groups. The reduction, however, was higher in the MINO Group: -1.64 versus -0.40 in the CORT Group (p-value=0.004), showing higher effectiveness of minocycline in the control of vitiligo activity in this group of patients (Graph 3).
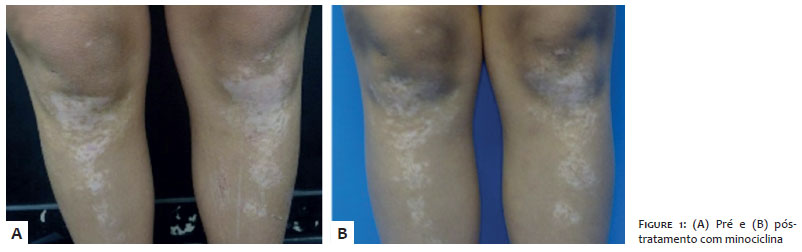
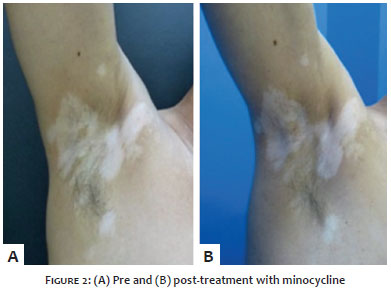
In some patients in the MINO Group, in addition to vitiligo stabilization, it was observed repigmentation at the end of the third month of treatment, as exemplified in Figures 1 and 2.
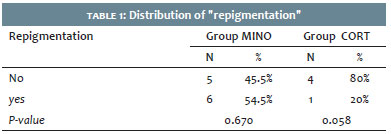
Table 1 presents the distribution regarding repigmentation between MINO and CORT Groups, showing, as additional data, repigmentation in 54.5% of the patients at the end of the treatment with minocycline, compared with 20% of the patients in the prednisolone group.
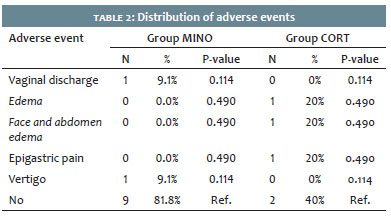
No patient presented severe adverse events during the study, and these were most often attributed to the use of corticosteroids. Only two of the 11 patients reported adverse events associated with the use of minocycline (vaginal discharge and vertigo), as shown in Table 2.
Vitiligo is a skin depigmentation disorder resulting from a selective loss of melanocytes. Both sexes are equally affected, and there are no apparent differences in occurrence rates according to phototype or race. 27
It is a complex disease, associating genetic aspects and environmental factors with metabolic and immune changes.27
Aiming to expand the therapeutic arsenal, the present study intended to evaluate the effect of minocycline on vitiligo activity compared with the conventional treatment, which is the corticosteroid.
Minocycline has a broad range of anti-inflammatory and immunomodulatory actions in addition to its already well-characterized antimicrobial effect.14 Its mechanism of action is complex and not fully understood, including inhibition of free radical and cytokine production, interference with protein synthesis, modulation of the metalloproteinases action, and antiapoptotic action.14 Both oxidative stress and apoptosis have been shown to play a significant role in the pathogenesis of vitiligo. Thus, minocycline offers a potentially powerful approach to controlling disease activity.14
In a previous study, Parsad and Kanwar14 evaluated the efficacy of minocycline 100 mg once daily in 32 patients. The study showed control in the disease progression in 29/32 patients and only three patients presented the development of new lesions and/or increase of existing lesions. Ten patients had discontinuation of depigmentation after four weeks of treatment. Also, seven patients presented moderate to severe repigmentation.
Recently, Singh et al.13 conducted a randomized controlled trial to evaluate the efficacy of dexamethasone oral minipulse therapy versus oral minocycline therapy in patients with active vitiligo vulgaris. They observed that of the 25 patients in the minocycline group, only six (24%) developed new lesions during 24 weeks of follow-up, while in the dexamethasone oral minipulse therapy only three (12%) patients presented disease activity. These results in the minocycline group were comparable to those observed in the Parsad and Kanwar study.14
The present study demonstrated that in both treatments, the MINO Group and the CORT Group showed control in the vitiligo activity with statistical significance assessed by the VIDA questionnaire. However, comparing the groups at each time of treatment (pre and post) and also evaluating the gain (simple difference between the mean of the results of post minus pre-treatment of the VIDA score), it was observed the existence of statistically significant difference among the groups assessed, pointing to better effects with the minocycline than with the corticosteroid treatment.
Analyzing the variables repigmentation and vitiligo stabilization in the treatment groups, it was observed that there is no statistical relationship between the data, i.e., they are independent variables.
The observed adverse events were, in a descriptive way, in the MINO Group: a patient with vaginal discharge and a patient with vertigo; and in the CORT Group: three of the five patients reported adverse events, being two patients with edema and one patient with epigastralgia. Studies with a more significant sample may be necessary to better evidence the results of the use of oral minocycline in the treatment of vitiligo.
Thus, the use of minocycline as a potential medication to control active vitiligo would be a therapeutic option with less severe adverse events compared with prolonged use of systemic corticosteroids.
The present study demonstrated the efficacy of minocycline in the control of active vitiligo compared with the treatment already established with systemic corticosteroid therapy, with an already well-established activity control effect. According to the judgment of the comparative photographic records before and after three months of treatment, the vitiligo activity was controlled in 100% of the patients in the MINO Group, while in the CORT Group the control of the activity was 60%.
Regarding the VIDA score, a statistically significant difference was observed for both groups in the disease control; however, it was found that the reduction was greater in the MINO Group, evidencing more effectiveness of minocycline in the control of vitiligo activity. Further controlled studies should be conducted to confirm its efficacy.
Gabriela Momente Miquelin | ORCID 0000-0002-8247-321X
Statistical analysis, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the literature, critical review of the original.
Mariana Morais Tavares Colferai | ORCID 0000-0002-1667-4988
Design and planning of the study, data collection, analysis and interpretation, intellectual participation in propaedeutics and/ or therapeutics in the cases studied.
Denise Steiner | ORCID 0000-0001-6450-9234
Approval of the final version of the original, active participation on mentoring the research, critical review of the original.
1. Steiner D, Bedin V, Moraes MB, Villas RT, Steiner TA. Vitiligo. An Bras Dermatol. 2004;79(3): 335-51.
2. Amer AA, Gao XH. Quality of life in patients with vitiligo: an analysis of the dermatology life quality index outcome over the past two decades. Int J Dermatol. 2016;55(6): 608-14.
3. Tarlé RG, Nascimento LM, Mira MT, Castro CC. Vitiligo-part 1. An Bras Dermatol. 2014;89(3):461-70.
4. Yaghoobi R, Omidian M, Bagherani N. Vitiligo: a review of the published work. J Dermatol. 2011;38(5):419-31.
5. Sampaio SAP, Rivitti EA. Dermatologia. 3th ed. São Paulo: Editora Artes Médicas; 2007.
6. Bellet JS, Prose NS. Vitiligo in children: a review of classification, hypotheses of pathogenesis and treatment. An Bras Dermatol. 2005;80(6): 631-6.
7. Silva CMR, Pereira LB, Gontijo B, Ribeiro GB. Childhood vitiligo: clinical and epidemiological characteristics. An Bras Dermatol. 2007;82(1):47-51.
8. Karsli N, Akcali C, Ozgoztasi O, Kirtak N, Inaloz S. Role of oxidative stress in the pathogenesis of vitiligo with special emphasis on the antioxidant action of narrowband ultraviolet B phototherapy. J Int Med Res. 2014;42(3):799-805.
9. Belda Junior W, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 2nd ed. São Paulo: Atheneu; 2014.
10. Dicle O, Assessment Methods in Vitiligo. J Pigment Disord 2015;02:160.
11. Njoo MD, Das PK, Bos JD, Westerhof W. Association of the Köbner phenomenon with disease activity and therapeutic responsiveness in vitiligo vulgaris. Arch Dermatol. 1999;135(4):407-13.
12. Bacigalupi RM, Postolova A, Davis RS. Evidence-Based Non-Surgical Treatments for Vitiligo: A review. Am J Clin Dermatol. 2012;13(4):217-37.
13. Singh A, Kanwar AJ, Parsad D, Mahajan R. Randomized controlled study to evaluate the effectiveness of dexamethasone oral minipulse therapy versus oral minocycline in patients with active vitiligo vulgaris. Indian J Dermatol Venereol Leprol. 2014;80(1):29-35.
14. Parsad D, Kanwar A. Oral Minocycline in the treatment of vitiligo - A preliminary study. Dermatol Ther. 2010;23(3):305-7.
15. Song X, Xu A, Pan W, Wallin B, Kivlin R, Lu S, et al. Minocycline protects melanocytes against H2O2- induced cell death via JNK and p38 MAPK pathways. Int J Mol Med. 2008;22(1):9-16.
16. Pasricha JS, Khaitan BK. Oral mini-pulse therapy with betamethasone in vitiligo patients having extensive or fast-spreading disease. Int J Dermatol. 1993;32(10):753-7.
17. Passeron T, Ortonne JP. Physiopathology and genetics of vitiligo. J Autoimmun. 2005;25 Suppl:63-8.
18. Kim SM, Lee HS, Hann SK. The efficacy of low-dose oral corticosteroids in the treatment of vitiligo patients. Int J Dermatol. 1999;38(7):546-50.
19. Radakovic-Fijan S, Furnsinn-Friedl AM, Honigsmann H, Tanew A. Oral dexamethasone pulse treatment for vitiligo. J Am Acad Dermatol. 2001;44(5):814-7.
20. Kanwar AJ, Dhar S, Dawn G. Oral minipulse therapy in vitiligo. Dermatology. 1995;190(3):251-2.
21. Banerjee K, Barbhuiya JN, Ghosh AP, Dey SK, Karmakar PR. The efficacy of low-dose oral corticosteroids in the treatment of vitiligo patient. Indian J Dermatol Venereol Leprol. 2003;69(2):135-7.
22. Marchioro HZ, Zunino MMB, Viesi JMZ, Cerci FB, De Castro CCS. Treatment of developing vitiligo with oral mini-pulse of Dexamethasone. Surg Cosmet Dermatol. 2012;4(3):284-7.
23. Cloridrato de minociclina. Rio de Janeiro: Ranbaxy Farmacêutica Ltda.,[2014]. Bula de remédio.
24. Spiegel MR, Estatística Coleção Schaum, 3. ed. São Paulo: Editora Afiliada, 1993.
25. Vieira S. Bio Estatística Tópicos Avançados, 2. ed. Rio de Janeiro: Campus, 2004.
26. Vieira S. Introdução à Bioestatística, Rio de Janeiro: Campus, 1991.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}