


Carla Corrêa Martins; Juliana Catucci Boza; Natalia Piccinini Giongo; Roberta Horn; Amanda Rodrigues Fabbrin; Priscilla Granja Machado; Tania Ferreira Cestari
Received on: 25/02/2019
Approved on: 06/04/2019
Study conducted at Hospital de Clínicas de Porto Alegre - Porto Alegre (RS), Brazil.
Financial support: Fundo de Incentivo à Pesquisa e Eventos (FIPE) of the Hospital de Clínicas de Porto Alegre.
Conflict of interests: None
INTRODUCTION: The relationship between cardiovascular disease, insulin resistance and vitiligo has been evaluated in studies. However, there is still no consensus on the subject.
OBJECTIVES: To evaluate the relationship between insulin resistance and vitiligo, in addition to the prevalence of risk factors for cardiovascular disease, in adults with vitiligo when compared to the control group.
METHODS: Cross-sectional study with a control group. A convenience sample of consecutive patients aged 14 years and over was used. Patients and controls were assessed with laboratory tests and anthropometric measurements. The LAP, HOMA-IR, and HOMAβ indices were calculated.
RESULTS: We included 130 patients, 73 with a diagnosis of vitiligo and 57 controls. There were no significant differences between groups when LAP, HOMA-IR, and HOMAβ were evaluated. Among the risk factors for cardiovascular disease, systolic blood pressure was significantly higher in patients with vitiligo.
CONCLUSIONS:There was no higher prevalence of insulin resistance among patients with vitiligo. Regarding the risk factors for cardiovascular diseases, only systolic blood pressure was higher in patients with vitiligo. Further studies are needed to elucidate the prevalence of insulin resistance and cardiovascular risk factors in patients with vitiligo.
Keywords: Vitiligo; Skin diseases, Metabolism; Metabolic diseases; Insulin resistance
Vitiligo is an acquired multifactorial disease that is characterized by the appearance of macromolecules and achromatic spots on the skin and mucous membranes due to the disappearance of melanocytes in the affected areas.1 According to data from regional studies worldwide, its prevalence can vary from 0.06% to 2.28% in adults and from 0 to 2.1% in children.2 Studies show an increased prevalence of autoimmune diseases in vitiligo patients, such as Hashimoto's thyroiditis, type 1 diabetes mellitus, Addison's disease, alopecia areata, and pernicious anemia, among others.3,4 In addition to these associations, the relationship between cardiovascular disease, insulin resistance (IR) and vitiligo has been studied. Some studies suggest a higher prevalence of type 2 diabetes in patients with vitiligo;5 the only study that related the disease with IR, comparing patients with controls, found a higher prevalence of IR among patients with vitiligo.6 However, another study that assessed diagnostic criteria for metabolic syndrome found a better metabolic profile in patients with vitiligo. Therefore, there is no consensus on the subject to date.7
The dysfunction of β-cells and IR are interrelated metabolic abnormalities in the etiology of type 2 diabetes mellitus (T2DM). IR is characterized by target cells failure to respond to normal levels of circulating insulin, resulting in compensatory hyperinsulinemia in an attempt to obtain an adequate physiological response. Due to the association between IR and endothelial dysfunction, an initial step for the atherosclerosis process, the disease has been considered as an independent predictor of cardiovascular disease.8 The hyperinsulinemic-euglycemic clamp is the gold standard for evaluating IR, but difficult to perform. The Homeostasis Model Assessment Insulin Resistance (HOMA-IR) and Homeostasis Model Assessment β-Cell Function (HOMAβ) methods, which measure the functional capacity of β-pancreatic cells, were validated for the diagnosis of IR against the gold standard, supporting its use in epidemiological studies.8,9
LAP (lipid accumulation product) is a central lipids accumulation index based on a combination of waist circumference (WC) and triglycerides (TG). It was created to describe how an individual altered the path of abdominal waist growth and serum triglyceride levels in the Third National Health and Nutrition Examination Survey (NHANES III). The calculation formula includes the minimum WC values used to define specific points according to the patient's gender (65cm and 58cm for men and women, respectively). Current literature suggests a strong association between the lipid accumulation product (LAP) and metabolic syndrome.10,11,12
The objective of this study was to assess the relationship between IR and vitiligo by the HOMA-IR, HOMAβ and LAP methods, as well as to evaluate the cardiovascular risk factors in adults with vitiligo when compared with the control group.
The sample size calculation was performed aiming to find a four times higher difference in the HOMA-IR variable than that found in the study by Karadag et al.,6 which was 0.3, with a standard deviation of 2.6 in the cases and 1.2 in the controls. Considering a power of 80%, and a significance level of 5%, a total sample size of 110 subjects was reached, with 55 in each group. The program WinPepi, version 11.43 was used.
A cross-sectional study with the control group was conducted. We used a convenience sample of cases and controls with consecutive 14 years or more of patients in the Dermatology Outpatient Clinic of the Hospital de Clínicas de Porto Alegre. Patients with psoriasis, diabetes and using immunosuppressive drugs were excluded. Patients and controls were investigated with laboratory tests including insulin, C-peptide, fasting glycemia (FG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), and triglycerides (TG). Anamnesis and physical examination were performed, measuring waist circumference (WC), hip (HC), weight, height, and blood pressure (BP). From these data, HOMA-IR, HOMAβ, LAP indexes and waist-hip ratio (WC/HC) were calculated. The HOMAβ index was calculated by the formula (FG (mg/dL)) x (insulin (µUI/mL))/22.5, and HOMA-IR by the formula (20 x insulin (µUI/mL) mg/dL) - 3.5).13
The LAP index was calculated using the formula: (WC(cm) - 65) x (TG concentration (mmol/l)) for men, and (WC(cm) – 58) x (TG concentration (mmol/l)) for women.12 The statistical analysis was performed in the SPSS 18.0 program. The categorical variables were compared by the chi-square test or Fisher's exact test. The quantitative variables with symmetrical distribution were compared between the groups by Student's t-test and described with mean ± standard deviation. Those with asymmetric distribution were compared by the Mann-Whitney test and described with median and interquartile range.
Covariance analysis (ANCOVA) was used to adjust the difference in the outcomes for potential confounding factors: age, BMI, dyslipidemia, hypertension, smoking, alcohol consumption, and antihypertensive use. A significance level of 5% was considered. The study was approved by the institution's ethics committee, and patients signed an informed consent.
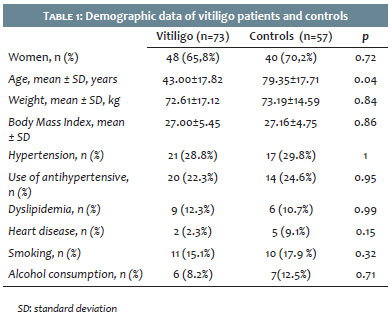
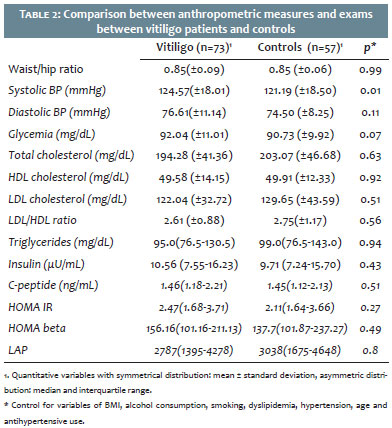
A total of 130 patients were included, 73 with diagnosis of vitiligo and 57 controls; 65% of the patients were women in the vitiligo group and 70% in the control group. The mean age in the vitiligo group was 43 years, and 49 years in the control group (p=0.04). There was no statistical difference between the groups when gender, BMI, weight, hypertension diagnosis or antihypertensive use, cardiopathy, dyslipidemia, alcohol consumption or current smoking were assessed (Table 1). There were no significant differences between groups when LAP, HOMA-IR, HOMAβ, insulin, and C-peptide measures were compared, even when the variables were controlled for potential confounding factors. The groups were also not statistically different when the waist-hip ratio, HDL, LDL, LDL/HDL ratio, and TG were assessed. Mean systolic BP was significantly higher in the vitiligo group when compared with controls (124.57 ± 18.01 mmHg versus 121.19 ± 18.5 mmHg; p=0.01). The glycemia levels were higher in the vitiligo group than in the control group (92.04 ± 10.01mg/dL versus 90.73 ± 9.92mg / dL), but without statistical significance (p = 0.07) (Table 2).
Different from our results, the only controlled study in adults with vitiligo that assessed IR, published by Karadag et al., found significantly higher insulin resistance among vitiligo patients. This study evaluated 96 individuals, 57 patients with vitiligo and 39 individuals in the control group, all with similar age and body mass index. In fasting, insulin, C-peptide, glucose, CT, TG, LDL, HDL, and BP were collected. IR was calculated using the HOMA-IR assessment method. Patients with vitiligo had significantly higher levels of HOMA-IR, insulin, and C-peptide.6 In our study, higher levels of insulin, C-peptide, and HOMA-IR were also found in the vitiligo group, but without statistical significance. It is not known, however, whether these differences in insulin levels between the groups found in these studies actually have any clinical impact, posing a greater risk of progression to T2DM or cardiovascular events. Longitudinal studies and larger sample sizes are needed to elucidate this question.
As in our study, the systolic blood pressure of patients with vitiligo was higher in comparison with the patients of the control group in the study cited above.6
The controlled study that addressed the prevalence of diagnostic criteria for metabolic syndrome in adult patients with vitiligo, published by Rodríguez-Martín et al., found a better metabolic profile in patients with vitiligo. It included 105 patients with vitiligo and 95 in the control group and found a lower prevalence of altered levels of triglycerides and abdominal circumference in patients with vitiligo.7 Also, there was a lower prevalence of altered levels of HDL in the vitiligo group, unlike the Karadag study, which found lower levels of HDL and a higher LDL/HDL ratio in patients with vitiligo.6 The authors believe that this finding may have an enzymatic basis that results in a negative association between vitiligo and cardiovascular risk factors.7
The biological hypotheses used to explain the probable relationship between vitiligo, insulin resistance, and risk factors for cardiovascular disease are based on the likely dysfunction in the antioxidant mechanism of vitiligo patients.14 Studies have shown a tendency to low activity of enzymatic and non-enzymatic antioxidants, such as catalase, glutathione peroxidase, and vitamin E, in patients with vitiligo, possibly increasing H2 O2 toxicity in affected tissues.15,16 However, some studies found no difference in these markers when comparing vitiligo patients and controls.17,18 The melanocytes production in adipose tissue would act as a protective factor against oxidative stress in this tissue, which could lead to greater oxidative stress in the adipose tissue of individuals with vitiligo, according to the study.19 Another study found high levels of homocysteinemia in patients with vitiligo, which could be related to increased cardiovascular risk, according to authors.20 However, the real influence of these markers on systemic oxidative stress is questioned, since to date the clinical studies have had conflicting results. As a limitation of the study, we can cite the cross-sectional design. To date, there are no studies with another design.
Our results showed no difference between groups when assessed for IR. Among the risk factors for cardiovascular diseases, only systolic BP was higher in the vitiligo group. Therefore, we cannot affirm that patients with vitiligo present a poorer metabolic profile or higher IR when compared with controls. Further studies are needed to evaluate the relationship between vitiligo, IR, and cardiovascular risk in order to elucidate the importance of these factors in the evolution of the disease, which is of great relevance for the clinical management of patients.
We thank the Dermatology staff of the Hospital de Clínicas of Porto Alegre and all the patients who accepted to participate in the research.
Carla Corrêa Martins | ORCID 0000-0003-4341-1005
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the literature, critical review of the original.
Juliana Catucci Boza | ORCID 0000-0002-0573-1617
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the literature, critical review of the original.
Natalia Piccinini Giongo | ORCID 0000-0001-5139-2719
Design and planning of the study, data collection, analysis and interpretation.
Roberta Horn | ORCID 0000-0002-4965-895X
Design and planning of the study, data collection, analysis and interpretation.
Amanda Rodrigues Fabbrin | ORCID 0000-0001-9629-5218
Design and planning of the study, data collection, analysis and interpretation.
Priscilla Granja Machado | ORCID 0000-0002-8139-7171
Data collection, analysis and interpretation.
Tania Ferreira Cestari | ORCID 0000-0003- 3001-0202
Statistical analysis, approval of the final version of the original, design and planning of the study, active participation on mentoring the research, intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the original.
1. Tarlé RG, Nascimento LM, Mira MT, Silva de Castro CC. Vitiligo - Part 1. An Bras Dermatol. 2014;89(3):461-70.
2. Krüger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206-12.
3. Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. 2015; 386(9988):74-84.
4. Gill L, Zarbo A, Isedeh P, Jacobsen G, Lim HW, Hamzavi I. Comorbid autoimmune diseases in patients with vitiligo: A cross-sectional study. J Am Acad Dermatol. 2015;74(2):295-302
5. Afkhami-Ardekani M, Ghadiri-Anari A, Ebrahimzadeh-Ardakani M, Zaji N. Prevalence of vitiligo among type 2 diabetic patients in an Iranian population. Int J Dermatol. 2014;53(8):956-8.
6. Karadag AS, Tutal E, Ertugrul DT. Insulin resistance is increased in patients with vitiligo. Acta Derm Venereol. 2011;91(5):541-4.
7. Rodríguez-Martín M, de Paz NM, Mehtani P, Ferrer PC, Eliche MP, Martín BR, et al. Patients with vitiligo present fewer cardiovascular risk factors: results from a case-control study. J Eur Acad Dermatol Venereol. 2013;27(1):124-5.
8. Vasques AC, Rosado LE, Cássia G, Alfenas RD, Geloneze B. Critical analysis on the use of the homeostasis model assessment (HOMA) indexes in the evaluation of the insulin resistance and the pancreatic beta cells functional capacity. Arq Bras Endocrinol Metabol. 2008;52(1):32-9.
9. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and B-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412-9.
10. Taverna MJ, Martínez-Larrad MT, Frechtel GD, Serrano-Ríos M. Lipid accumulation product: a powerful marker of metabolic syndrome in healthy population. Eur J Endocrinol. 2011;164(4):559-67.
11. Motamed N, Razmjou S, Hemmasi G, Maadi M, Zamani F. Lipid accumulation productand metabolic syndrome: a population-based study in northern Iran, Amol. J Endocrinol Invest. 2016;39(4):375-82.
12. Kahn HS. The "lipid accumulation product" performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC Cardiovasc Disord. 2005;5:26.
13. Radziuk J. Insulin sensitivity and its measurement: structural commonalities among the methods. J Clin Endocrinol Metab. 2000;85(12):4426-33.
14. Pietrzak A, Bartosińska J, Hercogová J, Lotti TM, Chodorowska G. Metabolic syndrome in vitiligo. Dermatol Ther. 2012;25(Suppl 1):S41-3.
15. Yildirim M, Baysal V, Inaloz HS, Kesici D, Delibas N. The role of oxidants and antioxidants in generalized vitiligo. J Dermatol. 2003;30(2):104-8.
16. Koca R, Armutcu F, Altinyazar HC, Gürel A. Oxidant-antioxidant enzymes and lipid peroxidation in generalized vitiligo. Clin Exp Dermatol. 2004;29(4):406-9.
17. Picardo M, Passi S, Morrone A, Grandinetti M, Di Carlo A, Ippolito F. Antioxidant status in the blood of patients with active vitiligo. Pigment Cell Res. 1994;7(2):110-5.
18. Beazley WD, Gaze D, Panske A, Panzig E, Schallreuter KU. Serum selenium levels and blood glutathione peroxidase activities in vitiligo. Br J Dermatol. 1999;141(2):301-3.
19. Page S, Chandhoke V, Baranova A. Melanin and melanogenesis in adipose tissue: possible mechanisms for abating oxidative stress and inflammation. Obes Rev. 2011;12(5):21-31.
20. Karadag AS, Tutal E, Ertugrul DT, Akin KO, Bilgili SG. Serum holotranscobalamine, vitamin B12, folic acid and homocysteine levels in patients with vitiligo. Clin Exp Dermatol. 2012;37(1):62-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}