


Célia Luiza Petersen Vitello Kalil1,2; Clarissa Prieto Herman Reinehr1,2; Laura de Mattos Milman1,3; Christine Prescendo Chaves4
Received on: 10/04/2019
Approved on: 06/06/2019
Study conducted at Clínica Célia Kalil, Porto Alegre (RS), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Idiopathic guttate hypomelanosis is an acquired leukoderma, whose available therapeutic options have inconsistent results.
OBJECTIVES: To evaluate the effect of isolated or combined ablative fractionated laser to drug delivery of piperine for treatment of idiopathic guttate hypomelanosis.
MATERIALS AND METHODS: In a prospective and comparative study, seven patients with idiopathic guttate hypomelanosis in the legs were elected, andfive lesions were selected on each leg of each. Both legs of each patient were submitted to two Er:YAG 2940nm laser sessions, followed by drug delivery of piperine 20% only in the right leg. Blind evaluators conducted the assessment through photographs and comparative measurements of the lesions.
RESULTS: The lesion size ranged from 0.2cm to 1.5 cm. Both treatments significantly reduced lesion size (p< 0.00008, right leg;p< 0.002, left leg). Thegeneralized estimating equation method showed that there was no statistical difference between the groups regarding the reduction of lesion size. The evaluation achieved better scores for the right leg (laser + piperine) (p=0.126).
CONCLUSION: Although statistically significant differences were not found between the side treated with laser and drug delivery versus the side treated only with laser, we believe that the technique may represent an option in the therapeutic arsenal.
Keywords: Administration, topical; Drug administration routes; Lasers
Idiopathic guttate hypomelanosis (IGH) is an acquired leukoderma that begins to appear in middle-aged individuals.1 IGH represents an event of the skin aging process, along with senile lentigos and whitening of the hair, among others.2 Clinically, IGH presents as hypopigmented, asymptomatic, rounded or oval macules in photoexposed areas, mainly in limbs.1 The pathogenesis of IGH is not completely elucidated: senile degeneration, exposure to ultraviolet radiation, trauma, autoimmunity, and local inhibition of melanogenesis may be involved.3,4 Also, lesions, in general, are accompanied by other photodamage signals, and some authors believe that its pathogenesis may be similar to that observed in hair whitening.2
Therapeutic options for IGH treatment include topical tretinoin, calcineurin inhibitors, cryotherapy, dermabrasion, and laser fractional photothermolysis; however, treatment results are sometimes discouraging in clinical practice.5-10 The use of ablative fractional laser is described in the literature; in one study, the CO2 laser 10,600 nm achieved improvement over 75% in 47.9% of patients two months after treatment with a single session; another study compared the use of CO2 laser 10600 nm with Er:YAG 2940 nm versus 0.025% topical tretinoin and observed better results in the group receiving the laser treatment (p<0.01). 1,10
Melanocytes are dendritic cells that produce melanin, the main component responsible for cutaneous pigmentation.2 They are located mainly in the skin, more specifically in the basal layer of the epidermis and in the matrix of the hair follicles, also found in the iris, the cochlea, and the midbrain.2 The melanin production occurs in cellular organelles called melanosomes and, later, melanin is transferred to the epidermal keratinocytes.2
Piperine, the main alkaloid present in black pepper (Piper nigrum L., Piperaceae), has stimulatory effects on the replication and dendrite formation of melanocytes, both in vitro and in vivo.11,12 The mechanism suggested in this melanocytic stimulus appears to be mediated by the protein kinase C (PKC) since this stimulus can be counteracted by PKC inhibitors.11 Also, piperine does not bind to DNA when applied to the skin, such as occurs with the use of psoralens, so they do not form photoadducts.13
The drug delivery assisted by ablative fractional lasers allows to optimize the skin permeation of drugs by tissue ablation, which favors its use for several topical medications.14 To date, drug delivery assisted by ablative fractional lasers has not been reported in the literature as an option for IGH treatment; for this reason, the authors conducted this pilot study in order to evaluate the effect of piperine drug delivery.
To assess the effect of isolated or combined ablative fractional laser on the immediate topical application of piperine (drug delivery) for the treatment of IGH by means of a pilot, prospective, and comparative study.
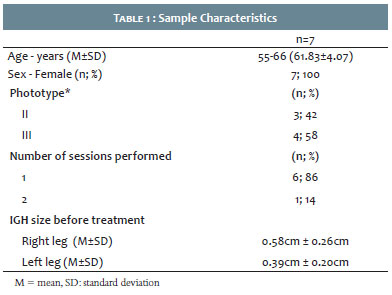
Seven female patients, aged 55-66 years, presenting IGH in the legs, were selected for this pilot study. All patients signed an informed consent form, and the study was conducted according to the rules of the Declaration of Helsinki. Five lesions were selected on each leg of each patient, which were measured for their largest diameter to allow objective comparative analysis at the end of the study. Both legs of each patient were submitted to two monthly sessions of ablative fractional laser Er:YAG 2940 nm (Etherea MX®, Vydence Medical, São Carlos, São Paulo, Brazil) 8mm, 100 MTZ/cm2, single mode (500µs) with an energy of 12.5mJ/MTZ, followed by cleaning with 0.9% saline immediately after the procedure to remove debris. Soon after the end of the described laser protocol, an anhydrous serum formulation containing 20% piperine was applied (drug delivery) only in the right leg of each patient; the patients were instructed to apply the formulation for three days after the procedure, three times a day. An important consideration is that piperine undergoes photoisomerization and loses its ability to stimulate melanocytes if exposed to visible light or ultraviolet radiation; for this reason, patients were instructed to avoid sun exposure during the application period of the product.13 The patients were evaluated one month after the second session; on this occasion, all lesions were measured again at their largest diameter and photographic records of the lesions were performed for the subjective analysis of the results.
The subjective evaluation of IGHs was conducted by two dermatologists blinded to the type of treatment performed in each leg. The following score was used to evaluate the improvement: 1 - worsening; 2 - no response; 3 - mild improvement (reduction of lesion size between 25-50%); 4 - good response (reduction of lesion size between 50-75%); 5- excellent response (reduction of lesion size over 75%).
Data were analyzed by SPSS version 21.0 (IBM Corporation, United States). Quantitative variables were compared between groups (laser + piperine versus laser alone) before and after treatment using the generalized estimating equation (GEE) method and the Bonferroni test. The paired T-test was used to evaluate the response to treatment (before and after) of each leg.
Seven patients were selected; six were submitted to two sessions and one to only one session (Table 1).
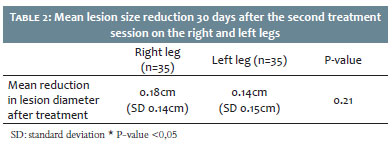
In total, 35 IGH lesions were treated in the right legs of the patients and 35 in the left legs. The size of the lesions ranged from 0.2cm to 1.5cm. The mean pre-treatment lesion size was 0.58cm in the right leg, where piperine was applied in drug delivery (confidence interval [CI]: 0.45-0.7 cm; standard deviation [SD]: 0.06cm) and 0.59 cm in the left leg (CI: 0.49-0.68cm; SD: 0.05cm), where only the laser was performed. Thirty days after the second session, the mean lesion size in the right leg was 0.39cm (CI: 0.28-0.51cm; SD: 0.06cm) and 0.45cm in the left leg (CI: 0.34-0.55cm; SD: 0.05cm) (Table 2). The paired T-test demonstrated that both treatments significantly reduced the lesion size (p<0.00008 for the right leg and p<0.002 for the left leg). The GEE method showed that there was no difference between the groups regarding the reduction of the size of the lesions (Bonferroni test: 0.083). The subjective evaluation reached better scores for the right leg (laser + piperine) (mean 4.72 versus 4.28 for the left leg); however, this difference did not reach statistical significance (p=0.126).
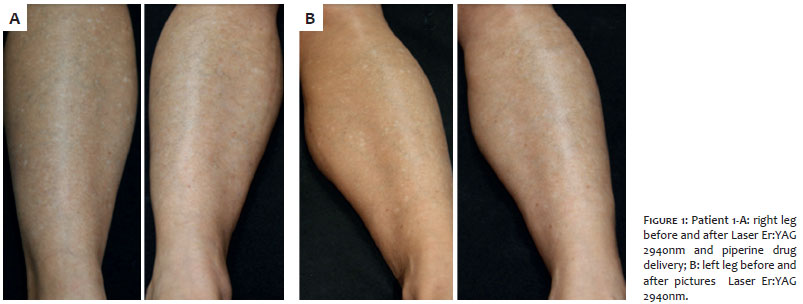
The photographic evaluation record of the clinical result achieved can be observed in Figure 1.
The ablative fractional laser produce ablation microchannels, surrounded by a thin coagulation zone, which facilitates the permeation of topical medications applied to the skin immediately after the procedure, this process is called laser-assisted drug delivery. A positive aspect of this method is the fact that the laser technique allows modulating the microchannels by changing the parameters used in the laser device. Thus, it is possible to modulate them in terms of size, depth and distance between each other.15 A noteworthy fact is that the formed microchannels are more permeable in the first hours after the procedure and, therefore, the medication should be applied immediately after the laser, as it was performed in this pilot study.15
When we think about the IGH treatment, it is important to try to understand its pathogenesis: there seems to be an associated genetic component that favors the physiological aging of melanocytes,16 as well as physical, chemical and biological factors that can cause DNA mutations resulting in depletion of stem cells in melanocytes.17 Also, TGF-beta signaling appears to be involved in the process.18
Some authors believe that there is an active process of depigmentation by inhibition of melanogenesis in IGH lesions. This hypothesis justifies the use of piperine as a therapeutic option.19 Some studies have evaluated the use of piperine for vitiligo treatment. A clinical study that assessed 18 vitiligo lesions treated in three patients observed repigmentation in the lesions with the use of piperine. Both the use of the Piper nigrum extract and that of the purified piperine in ointment vehicle promoted the pigmentation.20 The same study demonstrated the antioxidant activity of piperine by spectrophotometry.20 The use of piperine associated with narrow-band UVB phototherapy was described in a clinical study that evaluated 63 patients with facial vitiligo and observed superiority in repigmentation in patients in the group that received the application of piperine associated with phototherapy in relation to those who only performed isolated phototherapy (p<0.0001).21 In this case, the 1% piperine solution was applied one hour after the phototherapy since it is photoisomerized and inactivated if it is applied before the phototherapy session. Adverse events described with the application of piperine include burning sensation and erythema.21 To date, no study has evaluated the effect of piperine on the treatment of IGH.
Choosing the right vehicle for drug delivery is also extremely important. In the present study, we chose the vehicle anhydrous fluid serum, which has low viscosity and allows occlusion, and these factors potentiate the permeation of the assets added to it. Also, the vehicle is free of preservatives that could cause contact dermatitis or foreign body reaction.
Although our study found no statistically significant differences between the side treated with laser associated with piperine drug delivery and the side treated with ablative fractional laser alone, we believe that the technique may represent an option in the therapeutic arsenal of IGH. Limitations of the study include the small sample size, which was possibly one of the factors involved in the fact that no statistically significant differences were observed between treatment outcomes, despite the positive trend of higher response on the side receiving the associated drug delivery. Even if a result is not statistically positive due to the small sample size, in this case, the variability between the groups tends to have a significant impact. The mean of one group was higher than that of the other and, possibly, a larger group could demonstrate the superiority of the proposed technique. The small number of sessions and the short follow-up time are also relevant limitations. Since this is a pilot study, we assume that future studies, with larger sample size and a longer follow-up period, may clarify the doubts that have remained.
The search for effective treatments for IGH has not yet reached its final goal. The results of the currently available treatments are variable and often unsatisfactory. Such dissatisfaction with the results occurs both on the part of the dermatologist and the patient. The optimization of drug administration routes through drug delivery, as presented in this study with piperine, has been discussed for a number of dermatological conditions. Although the results of this pilot study are not definitive, we provide an option to be remembered when other therapies have not been effective in the treatment of IGH.
Célia Luiza Petersen Vitello Kalil | ORCID 0000-0002-1294-547X
Approval of the final version of the manuscript; data collection, analysis and interpretation; research guidance; intellectual participation in propaedeutic and / or therapeutic treatment of cases studied; critical review of the literature; critical review of the manuscript.
Clarissa Prieto Herman Reinehr | ORCID 0000-0003-1811-4519
Approval of the final version of the manuscript; study design and planning; manuscript preparation and Drafting; data collection, analysis and interpretation; research guidance; intellectual participation in propaedeutic and / or therapeutic management of the cases studied; critical review of the literature.
Laura de Mattos Milman | ORCID 0000-0002-3249-0396
Approval of the final version of the manuscript; study design and planning; manuscript preparation and Drafting; data collection, analysis and interpretation; research guidance; critical review of the literature.
Christine Prescendo Chaves | ORCID 0000-0001-8861-6499
Approval of the final version of the manuscript; study design and planning; manuscript preparation and Drafting; data collection, analysis and interpretation; research guidance; intellectual participation in propaedeutic and / or therapeutic management of the cases studied; critical review of the literature.
1. Koh WS, Kim JE, Ro YS, Ko JY. Comparative study of ablative fractional photothermolysis versus topical retinoid cream in the treatment of idiopathic guttate hypomelanosis. J Cosmet Laser Ther. 2018;20(7-8):405-9.
2. Yamaguchi Y, Hearing VJ. Melanocytes and Their Diseases. Cold Spring Harb Perspect Med. 2014;4(5):a017046.
3. Juntongjin P, Laosakul K. Idiopathic Guttate Hypomelanosis: A Review of its Etiology, Pathogenesis, Findings, and Treatments. Am J Clin Dermatol. 2016;17(4):403-11.
4. Shin M-K, Jeong K-H, Oh I-H, Choe B-K, Lee M-H. Clinical features of idiopathic guttate hypomelanosis in 646 subjects and association with other aspects of photoaging: Clinical features of idiopathic guttate hypomelanosis. Int J Dermatol. 2011;50(7):798-805.
5. Asawanonda P, Sutthipong T, Prejawai N. Pimecrolimus for idiopathic guttate hypomelanosis. J Drugs Dermatol. 2010;9(3):238-9.
6. Rerknimitr P, Disphanurat W, Achariyakul M. Topical tacrolimus significantly promotes repigmentation in idiopathic guttate hypomelanosis: a double-blind, randomized, placebo-controlled study: Tacrolimus promotes repigmentation in IGH. J Eur Acad Dermatol Venereol. 2013;27(4):460-4.
7. Ploysangam T, Dee-Ananlap S, Suvanprakorn P. Treatment of idiopathic guttate hypomelanosis with liquid nitrogen: light and electron microscopic studies. J Am Acad Dermatol. 1990;23( 4 Pt 1):681-4.
8. Hexsel DM. Treatment of idiopathic guttate hypomelanosis by localized superficial dermabrasion. Dermatol Surg. 1999;25(11):917-8.
9. Rerknimitr P, Chitvanich S, Pongprutthipan M, Panchaprateep R, Asawanonda P. Non-ablative fractional photothermolysis in treatment of idiopathic guttate hypomelanosis. J Eur Acad Dermatol Venereol. 2015;29(11):2238-42.
10. Goldust M, Mohebbipour A, Mirmohammadi R. Treatment of idiopathic guttate hypomelanosis with fractional carbon dioxide lasers. J Cosmet Laser Ther. 2013 may 8 ;1-10. Epub.
11. Lin Z, Hoult JRS, Bennett DC, Raman A. Stimulation of Mouse Melanocyte Proliferation by Piper nigrum Fruit Extract and its Main Alkaloid, Piperine. Planta Med. 1999;65(7):600-3.
12. Faas L, Venkatasamy R, Hider RC, Young AR, Soumyanath A. In vivo evaluation of piperine and synthetic analogues as potential treatments for vitiligo using a sparsely pigmented mouse model. Br J Dermatol. 2008;158(5):941-50.
13. Soumyanath A, Venkatasamy R, Joshi M, Faas L, Adejuyigbe B, Drake AF, et al. UV Irradiation Affects Melanocyte Stimulatory Activity and Protein Binding of Piperine. Photochem Photobiol. 2006;82(6):1541-8.
14. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
15. Banzhaf CA, Wind BS, Mogensen M, Meesters AA, Paasch U, Wolkerstorfer A, et al. Spatiotemporal closure of fractional laser-ablated channels imaged by optical coherence tomography and reflectance confocal microscopy. Lasers Surg Med. 2016;48(2):157-65.
16. Nishimura EK. Mechanisms of Hair Graying: Incomplete Melanocyte Stem Cell Maintenance in the Niche. Science. 2005;307(5710):720-4.
17. Inomata K, Aoto T, Binh NT, Okamoto N, Tanimura S, Wakayama T, et al. Genotoxic Stress Abrogates Renewal of Melanocyte Stem Cells by Triggering Their Differentiation. Cell. 2009;137(6):1088-99.
18. Nishimura EK. Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and skin pigmentation: Melanocyte stem cells. Pigment Cell Melanoma Res. 2011;24(3):401-10.
19. Falabella R, Escobar C, Giraldo N, Rovetto P, Gil J, Barona MI, et al. On the pathogenesis of idiopathic guttate hypomelanosis. J Am Acad Dermatol. 1987;16(1 Pt 1):35-44.
20. Mihăilă B, Dinică RM, Tatu AL, Buzia OD. New insights in vitiligo treatments using bioactive compounds from Piper nigrum. Exp Ther Med. 2019;17(2):1039-44.
21. Shafiee A, Hoormand M, Shahidi-Dadras M, Abadi A. The effect of topical piperine combined with narrowband UVB on vitiligo treatment: A clinical trial study: The effect of topical piperine/NB-UVB on vitiligo treatment. Phytother Res. 2018;32(9):1812-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}