


Farida Tabri
Received on: 04/04/2019
Approved on: 13/06/2019
Study conducted at the Dermatology and Venereology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Financial support: None
Conflict of interests: None
INTRODUCTION: Acne vulgaris is an inflammatory disorder of the pilosebaceous gland. Palmitic acid is one of the major types of free fatty acid and may play a role in acne pathogenesis. In addition, recent studies suggested that Staphylococcus epidermidis might be involved in acne.
OBJECTIVE: To explore the association between Staphylococcus epidermidis and palmitic acid in acne vulgaris.
METHODS: Forty-three high school students at an urban area in South Sulawesi, Indonesia, were included. The palmitic acid level was measured using gas chromatography and comedone was cultured to detect the microbiota profile. Mann-Whitney test was used to analyze the median palmitic level diference between groups with different acne vulgaris severity.
RESULTS: Fourteen patients (32.6%) had mild acne vulgaris, while 14 and 15 patients had moderate and severe acne vulgaris, respectively The severe and moderate group showed significantly higher palmitic acid level compared with the mild group. Subgroup analysis of patients with moderate and severe acne vulgaris positive for S. epidermidis showed a significantly higher palmitic acid level compared with the mild group.
CONCLUSIONS: This result suggests that S. epidermidis may be associated with the palmitic acid level and may contribute to acne pathogenesis.
Keywords: Acne vulgaris; Staphylococcus epidermidis; Palmitic acid
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous glands where lesions can be non-inflammatory (open and closed comedones) or inflammatory (papules and pustules).1, 2 Acne vulgaris mostly occurs in adolescence to young adulthood and can cause post-inflammatory hyperpigmentation and scarring. A study conducted by Bhate et al showed that acne can be found in about 20% of young adults.3 In addition, acne has a high persistence in which 43% of those over 30 years still have acne. Acne also has a strong genetic predisposition in which 80% of acne cases can be inherited to close relatives.3, 4
The human skin hosts a diverse group of microorganisms in which Staphylococcus, Cornybacterium, and Propionibacterium constitute 60% of all bacterial species.5 However, there are only limited studies examining the entire microbiota population in patients with acne and their role in acne pathophysiology. Despite the widely accepted view of the role of Propionibacterium acnes (P. acnes) in triggering acne, recent studies have suggested that Staphylococcus epidermidis (S. epidermidis) may also be involved in acne pathogenesis. Pathak et al.6 showed that the microbial load of S. epidermidis increases in acne lesions compared with control. This result is in line with a recent study where S. epidermidis was found in a more abundant manner compared to P. acne.7, suggesting the possible role of S. epidermidis in acne pathogenesis.
Besides microbiome, free fatty acid (FFA) has also been shown to be involved in the development of acne as increased level of FFA will lead to neutrophils influx through chemotaxis process.8 A high-fat diet has been shown to induce or aggravate acne vulgaris lesions.9 Of all FFA types, palmitic acid and its derivatives have been shown to be the most abundant type.10-12 Palmitic acid may stimulate the release of various proinflammatory cytokines and contribute to pilosebaceous duct hyperkeratinization and acne inflammation.13
To the best of our knowledge, no study has observed the association between S. epidermidis and palmitic acid and their association with acne vulgaris. The aim of this study is to investigate the microbiome profile, especially S. epidermidis, in patients with acne vulgaris and to investigate its association with palmitic acid level in inducing acne vulgaris lesions.
This cross-sectional study was conducted in a high school in Makassar, South Sulawesi, Indonesia, from July to August 2017. The subjects were given explanation about the study and those who agreed were asked to sign an informed consent form (Ref. Number; 145/H4.8.4.5.31/PP36-KOMETIK/2017 from Hasanuddin University Ethics Committee). Subjects who did not take retinoids, antibiotics, anti-inflammatory drugs, and other anti-microbial products, such as antifungal soap and shampoo, in the last one month were assessed for acne severity with the Lehman Criteria and classified into mild, moderate, or severe acne vulgaris.14 They were also given questionnaires to record family history of acne and dietary consumption.
Sebum was extracted from the forehead, nasolabial, cheek, and chins by an absorbent paper using acetone and diethyl ether with a ratio of 1:1 and then methylated using 0.2 M phenyltrimethylamine hydroxide solution in methanol. Gas chromatography was used to examine the product. The standard reference used was Supelco® 37 component FAME Mix. The standard concentration used for palmitic acid was 601 ppm injected into the gas chromatograph. Analysis was performed on a GC-MS QP 2010 Ultra Shimadzu Autosampler with a splitless injector. Separations were achieved using SH-Rxi-5Sil MS capillary column (30m x 0.25mm). Helium was used as the carrier gas at flow rates of 1.99mL/min and a split less ratio of 1:10. The injector temperature was 250ºC. The oven temperature was programmed at 140ºC for a hold of 10 minutes and increased to 250ºC with a flow of 7º C/min. It was further held for 10 minutes, resulting in a total analysis time of 35.71 minutes. MS spectra were obtained at range width m/z 40-500m/z, ion source and interface temperature 210ºC and 255ºC, respectively, and solvent cut time 3 minutes.
Sample from comedonal lesions was taken using a sterile comedone extractor and cultured in blood agar which was incubated at 37ºC for 48-72 hours. The growing colonies were observed under the microscope with gram staining. Each colony was made into a suspension equivalent to McFarland 0.5. The gram-positive and the gram-negative suspensions were taken 145µl and 280µl, respectively, and added into reaction tubes containing 3 ml saline solution. The gram-positive suspension was put into GPcard and AST GP 67 cards and the gram-negative suspension was put into GNcard dan ASTN 100 cards before final analysis using Vitek®.
Data analysis was done by using Statistical Package for Social Sciences (SPSS) 18.0 for Windows (SPSS Inc. Chicago, IL, USA). Mann-Whitney test was used to analyze the median palmitic level difference between groups with different acne vulgaris severity. A p-value <0.05 was considered significant.
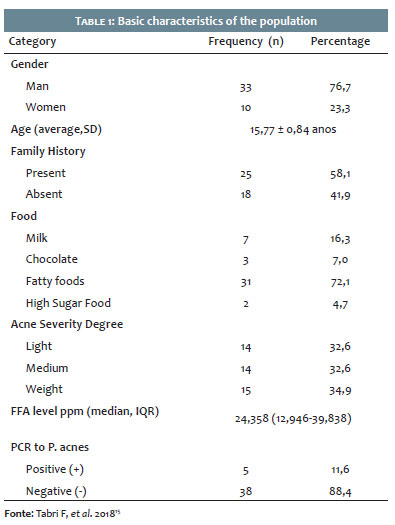
The demographic data in table 1 shows that of 43 participants, most participants (33 patients, 76.7%) were men and adolescent (15.77 ± 0.84 years). There were 25 participants with a positive family history of acne vulgaris (58.1%). As for the disease duration, 34.8% of the participants (15 subjects) have been having acne for 2 years and 10 subjects (23.3%) had had acne for 1 year and 3 years, respectively. Most of the patients (31 subjects, 72.1%) consumed fatty foods. The population showed almost uniform acne severity distribution: 14 patients were diagnosed with mild acne, 14 patients with moderate, and 15 patients with severe acne.
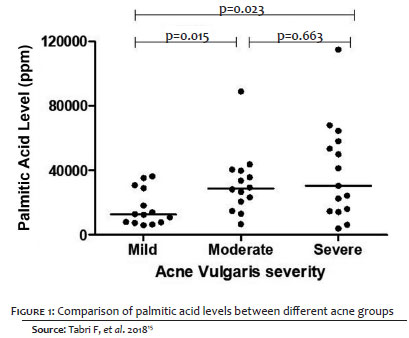
Figure 1 shows the concentration of palmitic acid in severe acne (median = 30,400 ppm) was significantly higher than that in the mild acne (30,400ppm vs 12,746ppm). The palmitic acid level in moderate acne was also found to be significantly higher than in the mild acne (p<0.05). However, no difference in palmitic acid level was found between patients with moderate and severe acne.
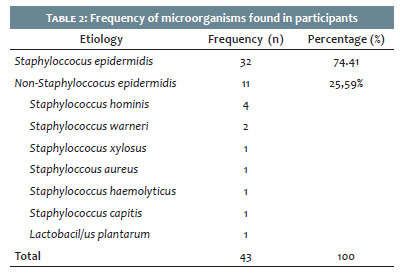
Table 2 shows the frequency of the microorganism found in the participants. It was shown that S. epidermidis was the most common microorganism cultured (32 subjects, 74.41%) and while non-S. epidermidis organisms were isolated in 11 cases (25.59%). The isolated non-S.epidermidis microorganisms were Staphylococcus hominis (4 cases), Staphylococcus warneri (2 cases) Staphylococcus xylosus (1 case), Staphylococcus aureus (1 case), Staphylococcus haemolyticus (1 case), Staphylococcus capitis (1 case), Lactobacillus plantarum (1 case).
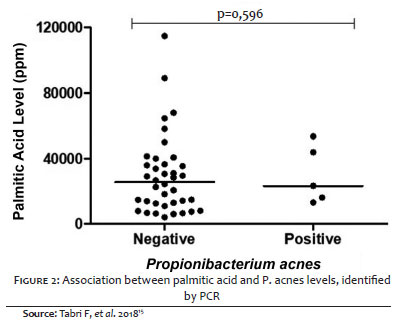
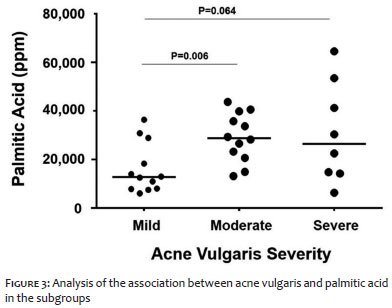
Data in Figure 2 shows that there was no association between S. epidermidis and palmitic acid level. However, the data in Figure 3 on subgroup analysis of patients with positive S. epidermidis culture showed that palmitic acid level in subjects with moderate acne vulgaris was significantly higher compared with mild acne vulgaris (p=0.006). Furthermore, subjects with severe acne vulgaris were also found to have higher palmitic acid level compared with those with mild acne with a borderline significance level (p=0.064).
Data from our study showed that higher palmitic acid level indicated a greater degree of acne severity. Palmitic acid levels in the facial skin of patients with severe and moderate acne vulgaris were found to be significantly higher than those with a mild degree of acne vulgaris. Several studies have suggested the role of palmitic acid in inducing pro-inflammatory cytokines, which contributes to inflammation and pilosebaceous duct hyperkeratinization.13, 15 Palmitic acid was shown to inhibit hydrogen peroxide which caused proinflammatory mediators to pass more easily to the dermis and aggravate inflammation.15
Data in table 2 showed that Staphylococcus epidermidis was the most common microorganism found in the subjects. Interestingly, there was no P. acne obtained through culture, despite the classical view that P. acne induces acne. Dreno et al.7 found a similar result, where S. epidermidis was the most abundant bacteria found in patients with acne vulgaris. They also observed that P. acne only constitutes less than 2% of the whole population. In contrast, other studies showed that in normal population, P. acne may represent up to 30% of the whole facial microbiota.16, 17 One possible explanation for this finding is that the aerobic and facultative anaerobic S. epidermidis mediates fermentation process which inhibits the growth of the anaerobic P. acne.18
Although the data in figure 2 shows that S. epidermidis was not associated with palmitic acid level, subgroup analysis of patients with positive S. epidermidis culture interestingly showed that the palmitic acid level in patients with moderate acne vulgaris to be significantly higher compared with those with mild disease (p=0.006). Those with severe acne were also found to exhibit higher palmitic acid level compared with those presenting mild acne with borderline significance level (p=0.064). Studies have suggested the possible role of palmitic acid inducing acne vulgaris through the activation of mechanistic target of rapamycin complex 1 (mTORC1) signaling pathway, triggering the activation of toll-like receptor 2 (TLR2), and pilosebaceous duct hyperkeratinization,13, 19, 20 In addition, the expression of NLRP3 and inflammasome-mediated IL-1β production are also upregulated which further perpetuates the inflammation process.21 Taken together, this result suggests that S. epidermidis may be associated with the level of palmitic acid level and hence be involved in the pathogenesis of acne vulgaris. Further biomolecular studies are needed to confirm this hypothesis.
Recent literature showed that S. epidermidis may be involved in the pathogenesis of acne vulgaris.22 A study by Bialtecka et al. showed that S.epidermidis induces inflammation in the form of Nitric Oxide production within the infected tissue. They also induce macrophage activation, as shown by the increase of TNF-alpha production and IL-12 production after incubation with S. epidermidis.23 This topic remains contentious, however, as Staphylococcus was shown to activate TLR2 and induce miR-143 in the keratinocytes that target 3' UTR of TLR2 and decrease the stability of TLR2 MRNA and TLR2 protein; resulting in the inhibition of P. acne proinflammatory cytokines.24, 25 Also, a study has suggested that fatty acid composition did not associate with the presence of acne, although they might differ in accordance with the amount of triglyceride.26 Furthermore, S. epidermidis is able to form biofilm by secreting the exopolysaccharide intercellular adhesion, which supports an anaerobic condition for P. acne to flourish.27, 28 With the above-mentioned data, whether skin microbiome provides a protective or pathogenic effect remains debatable.29
To the best of our knowledge, this is the first study to explore the association between S. epidermidis and palmitic acid level and their effect in acne vulgaris. This is an initial study conducted to assess the prevalence of acne vulgaris in the adolescent population of an urban area and its association with palmitic acid levels patients with acne vulgaris. However, as a preliminary study, the sample size is limited and hence some subgroup analysis could be conducted. This study also only assessed one type of free fatty acid. Squalene and its peroxide, for example, has been thought to contribute to inducing inflammation and comedone formation.30 Futures larger scale studies examining more than one type of free fatty acid need to be done. Nevertheless, this study provided important data and thus delivered a foundation for future studies in this field.
The result of this study shows that S. epidermidis is the most common microorganism cultured from the participants. In addition, S. epidermidis may be associated with higher palmitic acid levels which may contribute to the development of acne vulgaris. Further studies on the underlying mechanism of S. epidermidis in inducing palmitic acid level and acne vulgaris need to be conducted to confirm this hypothesis.
Farida Tabri | ORCID 0000-0003-4913-0909
Design and planning of the study, data collection, analysis and interpretation, preparation and writing of the manuscript, critical review of the manuscript. Approval of the final version of the manuscript.
1. Mourelatos K, Eady EA, Cunliffe WJ, Clark SM, Cove JH. Temporal changes in sebum excretion and propionibacterial colonization in preadolescent children with and without acne. Br J Dermatol. 2007;156(1):22-31.
2. Degitz K, Placzek M, Borelli C, Plewig G. Pathophysiology of acne. J Dtsch Dermatol Ges. 2007;5(4):316-23.
3. Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-85.
4. Szabo K, Kemeny L. Studying the genetic predisposing factors in the pathogenesis of acne vulgaris. Hum Immunol. 2011;72(9):766-73.
5. Grice EA, Segre JA. The skin microbiome. Nat Rev Microbiol. 2011;9(4):244-53.
6. Pathak R, Kasama N, Kumar R, Gautman H. Staphylococcus epidermidis in human skin microbiome associated with acne: a cause of disease or defence? Res J Biotechnol. 2013;8(12):78-82.
7. Dreno B, Martin R, Moyal D, Henley JB, Khammari A, Seite S. Skin microbiome and acne vulgaris: Staphylococcus, a new actor in acne. Exp Dermatol. 2017;26(9):798-803.
8. Katsuta Y, Iida T, Inomata S, Denda M. Unsaturated fatty acids induce calcium influx into keratinocytes and cause abnormal differentiation of epidermis. J Invest Dermatol. 2005;124(5):1008-13.
9. Burris J, Rietkerk W, Woolf K. Relationships of Self-Reported Dietary Factors and Perceived Acne Severity in a Cohort of New York Young Adults. J Acad Nutr Diet. 2014;114(3):384-92.
10. Berg JM, Tymoczko JL, Stryer L. Biochemistry. 5th ed. New York: W H Freeman; 2002.
11. Smith RN, Braue A, Varigos GA, Mann NJ. The effect of a low glycemic load diet on acne vulgaris and the fatty acid composition of skin surface triglycerides. J Dermatol Sci. 2008;50(1):41-52.
12. Desbois AP, Smith VJ. Antibacterial free fatty acids: activities, mechanisms of action and biotechnological potential. Appl Microbiol Biotechnol. 2010;85(6):1629-42.
13. Zhou BR, Zhang JA, Zhang Q, Permatasari F, Xu Y, Wu D, et al. Palmitic Acid Induces Production of Proinflammatory Cytokines Interleukin-6, Interleukin-1, and Tumor Necrosis Factor- via a NF-B-Dependent Mechanism in HaCaT Keratinocytes. Mediators Inflamm. 2013;2013:530429.
14. Lehmann HP, Robinson KA, Andrews JS, Holloway V, Goodman SN. Acne therapy: a methodologic review. J Am Acad Dermatol. 2002;47(2):231-40.
15. Tabri F, Anwar AI, Massi N, Patellongi IJ, Anwar R. Profile of free fatty acid in patients with acne vulgaris. Surg Cosmet Dermatol. 2018; 10(2):108-12.
16. Akamatsu H, Niwa Y, Matsunaga K. Effect of palmitic acid on neutrophil functions in vitro. Int J Dermatol. 2001;40(10):640-3.
17. Grice EA. The skin microbiome: potential for novel diagnostic and therapeutic approaches to cutaneous disease. Semin Cutan Med Surg. 2014;33(2):98-103.
18. Grice EA, Kong HH, Conlan S, Deming CB, Davis J, Young AC, et al. Topographical and temporal diversity of the human skin microbiome. Science. 2009;324(5931):1190-2.
19. Wang Y, Kuo S, Shu M, Yu J, Huang S, Dai A, et al. Staphylococcus epidermidis in the human skin microbiome mediates fermentation to inhibit the growth of Propionibacterium acnes: Implications of probiotics in acne vulgaris. Appl Microbiol Biotechnol. 2014;98(1):411-24.
20. Melnik BC. Acne vulgaris: The metabolic syndrome of the pilosebaceous follicle. Clin Dermatol. 2018;36(1):29-40.
21. Huang S, Rutkowsky JM, Snodgrass RG, Ono-Moore KD, Schneider DA, Newman JW, et al. Saturated fatty acids activate TLR-mediated proinflammatory signaling pathways. J Lipid Res. 2012;53(9):2002-13.
22. Snodgrass RG, Huang S, Choi I-W, Rutledge JC, Hwang DH. Inflammasome-Mediated Secretion of IL-1β in Human Monocytes through TLR2 Activation; Modulation by Dietary Fatty Acids. J Immunol. 2013;191(8):4337-47.
23. Nishijima S, Kurokawa I, Katoh N, Watanabe K. The Bacteriology of Acne Vulgaris and Antimicrobial Susceptibility of Propionibacterium acnes and Staphylococcus epidermidis Isolated from Acne Lesions. J Dermatol. 2000;27(5):318-23.
24. Bialecka A, Mak M, Bideron R, Bobek M, Kasprowicz A, Marcinkiewicz J. Different pro-inflammatory and immunogenic potentials of Propionibacterium acnes and Staphyloccocus epidermidis: implication for chronic inflammatory acne. Arch Immunol Ther Exp. 2005;53(2):79-85.
25. Xia X, Li Z, Liu K, Wu Y, Jiang D, Lai Y. Staphylococcal LTA-Induced miR-143 Inhibits Propionibacterium acnes-Mediated Inflammatory Response in Skin. J Invest Dermatol. 2016;136(3):621-30.
26. Christensen GJM, Scholz CFP, Enghild J, Rohde H, Kilian M, Thürmer A, et al. Antagonism between Staphylococcus epidermidis and Propionibacterium acnes and its genomic basis. BMC Genomics. 2016;17:152.
27. Akaza N, Akamatsu H, Numata S, Matsusue M, Mashima Y, Miyawaki M, et al. Fatty acid compositions of triglycerides and free fatty acids in sebum depend on amount of triglycerides, and do not differ in presence or absence of acne vulgaris. J Dermatol. 2014;41(12):1069-76.
28. Vuong C, Voyich JM, Fischer ER, Braughton KR, Whitney AR, DeLeo FR, et al. Polysaccharide intercellular adhesin (PIA) protects Staphylococcus epidermidis against major components of the human innate immune system. Cell Microbiol. 2004;6(3):269-75.
29. Fey PD, Olson ME. Current concepts in biofilm formation of Staphylococcus epidermidis. Future Microbiol. 2010;5(6):917-33.
30. Cogen AL, Nizet V, Gallo RL. Skin microbiota: a source of disease or defence? Br J Dermatol. 2008;158(3):442-55.
31. Ottaviani M, Camera E, Picardo M. Lipid mediators in acne. Mediators Inflamm. 2010;2010.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}