


Ricardo Vieira1,2; João Goulão3
Received on:18/05/2019
Approved on: 12/06/2019
Study conducted at Service of Dermatology, Coimbra Hospital and Universitary Center, Coimbra, Portugal.
Financial support: None.
Conflict of interests: None.
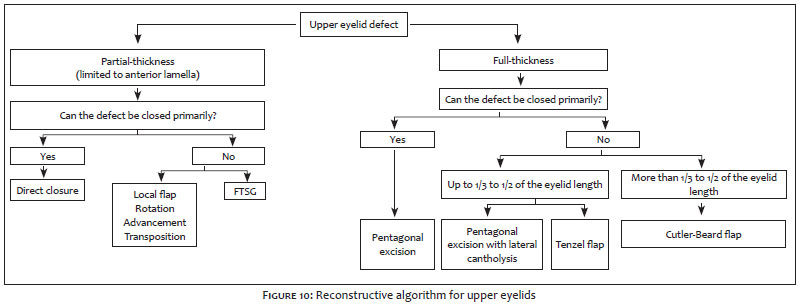
Eyelid defects resulting from skin cancer excision are common in the daily practice of dermatologic surgeons. The aim of this review is to summarize the most relevant methods for eyelid repair, proposing reconstructive algorithms for both lower and upper eyelids. Both algorithms were designed according with dichotomic decisions based on the thickness (partial- versus full-thickness) and the size of the eyelid defect (less than 1/3, less than 2/3 or larger than 2/3 of the eyelid length).
Keywords: Eyelids; Reconstruction; Eyelid Neoplasms; Eyelid Neoplasms/surgery; Cornea
Skin cancer excision is the main cause of eyelid defects to be treated by dermatologic surgeons. As occurs in other facial regions, basal cell carcinoma (BCC) is the most frequent neoplasm in the eyelids. Squamous cell carcinoma (SCC), melanoma and sebaceous carcinoma account for most of the remaining cases.1 The dermatologic surgeon has to be prepared to face this kind of defects, for which is essential to develop advanced surgical skills based on solid knowledge about eyelid anatomy and physiology.
Eyelid reconstruction is usually challenging and the decision about the optimal method to repair a specific defect is mainly based on two factors: the thickness and the extent of the defect.
The chosen closure method should result in tension vectors with a predominant horizontal orientation. Furthermore, the alignment of the free margin and the canthal fixation should be preserved or restored. Each layer of the eyelid should be repaired, from the internal tarsoconjunctival layer to the external cutaneous layer. These basic principles are essential to achieve optimal cosmetic and functional results, preventing complications, such are ectropium, lagophthalmos, epiphora, chronic conjunctivitis and corneal dryness, and ulceration.
Reconstructive algorithms are generally considered useful tools in the clinical setting, helping the surgeon to decide which management strategy should be chosen. The aim of this work is to design decisional algorithms both for upper and lower eyelids repair.
The algorithms were based on a literature review about eyelid repair and also on the author personal experience. Therefore, despite the literature review supporting the proposed options, the algorithms' decisions were also influenced by some personal preferences. The algorithms have no intention to include an extensive review of all the possible reconstructive options reported in the literature. Under the same combination of criteria (personal experience and literature review), the most relevant techniques were considered as the most reliable and consistent.
The size and the thickness of the defect were identified as the two factors with more impact in the decision about the reconstructive method to be used for both lower and upper eyelid defects.2,3,4
The management of partial-thickness defects differs significantly from the management of full-thickness defects since the latter require restoration of the posterior lamella (tarsoconjunctival layer) in addition to the anterior lamella (myocutaneous layer)2,3,4. Therefore, the thickness was considered the first condition to be included in the algorithm.
The extent of the eyelid length affected by the defect is more relevant than the absolute diameter itself. Therefore, the size, expressed as a fraction of the eyelid length, was pointed out as the second condition of the algorithm.
The ability to close primarily a defect is mainly related to the size of the defect. However, it may be also influenced by individual factors (tissue elasticity, age, etc.). Therefore, in those situations in which individual variations were considered to have influence in the reconstructive strategy, the ability to primarily close a defect was included as a specific condition instead of the size itself.
Partial-thickness defects. The repair of skin-only defects on the eyelid should be performed avoiding vertical tension to prevent ectropion, scleral exposure or lagophthalmos, causing cosmetic impairment and functional abnormalities such as epiphora, chronic conjunctivitis, and dry eye. Upper eyelids admit some grade of vertical tension, but lower eyelids are unable to support any kind of vertical tension. Therefore, a horizontal approach should be always considered.5 If the primary closure leads to distortion or vertical tension over the eyelid margin, the need for special techniques is obvious. Patients with impaired snap-back test are more prone to the occurrence of ectropium.6
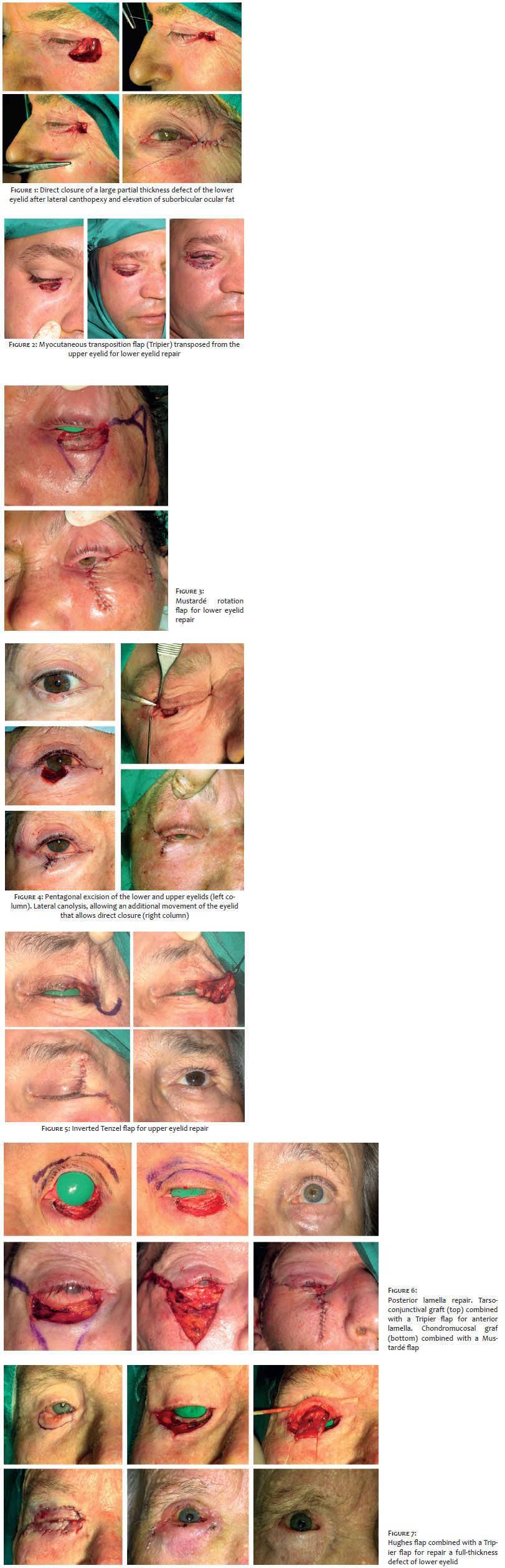
In large defects occurring in the lower eyelid, direct closure can be sometimes possible after stabilization of the eyelid through a lateral canthopexy and a lifting of the suborbicular oculi fascial tissue (SOOF)(Figure 1), anchoring this tissue to the periosteum of the orbital rim.7 Otherwise, a flap or a graft will be needed. Full-thickness skin grafts are efficient for repairing the anterior lamella on both eyelids.3,4 The most used donor area is the opposite upper eyelid.
The redundant skin of the upper eyelid can be recruited as advancement or rotation flaps for upper eyelid partial-thickness defects. Transposition flaps from the periocular region or from the supraciliary region can also be harvested for repairing bigger defects.
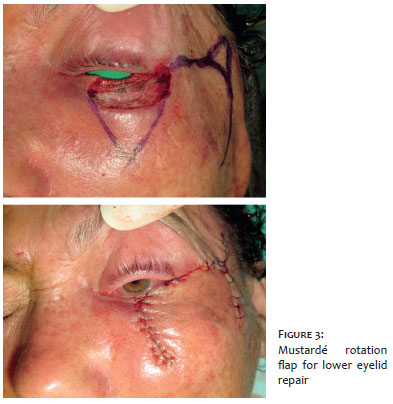
Several flaps were described for repairing lower eyelid partial-thickness defects. The Tripier flap8, which consists of a myocutaneous transposition flap from the homolateral upper eyelid is one of the most reliable techniques for this purpose (Figure 2). Other alternative transposition flaps are Fricke flap, Kreibig flap, and superiorly-based nasolabial flap. Advancement flaps (McGregor flap and Imre flap)8,9 from the periocular region are also a possibility. Mustardé rotation flap10 is a very good option to repair extensive defects of the lower eyelid anterior lamella (Figure 3).
Full-thickness defects. Small full-thickness defects can be repaired by direct closure. If the defect involves the eyelid margin, usually the closure is performed after planning the excision under a pentagonal shape (Figure 4, left column). This method results in a hipereversion of the lesion borders, leading to a correct alignment of the eyelid margin, crucial to achieve an optimal cosmetic and functional outcome.11 If there is too much tension and it is hard to join the lesion borders, the closure can be easily performed after the lateral canthal ligament have been cut (lateral cantholysis).4 This will allow an additional advancement of up to 5 mm (Figure 4, right column). After the suture, the lateral canthal ligament should be reattached to the periosteum of the orbital rim.
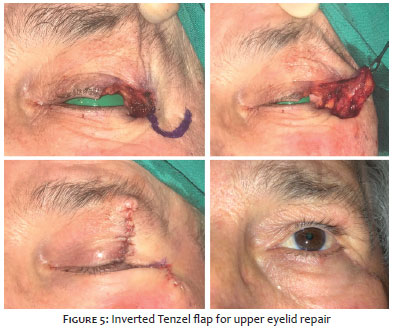
The Tenzel flap (semicircular advancement-rotation flap from the zygomatic region)4 is an excellent option for defects up to 1/3 of the eyelid length, despite this flap may be sufficient to repair defects up to 40-50% of the eyelid length in some older patients. The Tenzel flap has the advantage to repair both lamellas within a single procedure. The semicircular design of this flap is highly important to prevent ectropion. The convexity of the semicircle is superior for the lower eyelid; however, it is considered inferior for the upper eyelid (Figure 5).
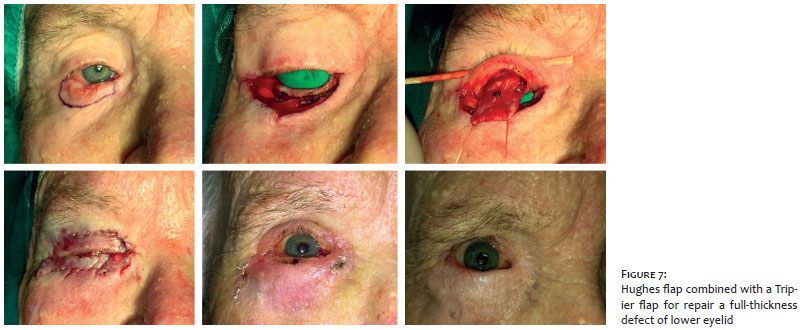
Defects bigger than 1/3 of the lower eyelid length commonly require multi-step procedures with sequential repair of posterior and anterior lamellas. Tarsoconjunctival grafts harvested in the upper eyelid (Figure 6, upper line) or flaps (Hughes flap)12 can repair defects up to 2/3 of the lower eyelid extent (Figure 7). From 2/3 to the totality of the eyelid, the nasal septum (alternatively, the oral mucosa and auricular cartilage can be used) is a good donor site to harvest chondromucosal grafts (Figure 6, bottom line), big enough for the entire posterior lamella restoration.13 When the posterior lamella is repaired with a graft, a flap should be performed to repair the anterior lamella,4 since a graft sutured over a graft will result in poor nutrition of both grafts, leading to necrosis. However, a full-thickness skin graft is a safe procedure to perform in addition to a Hughes tarsoconjuctival flap.
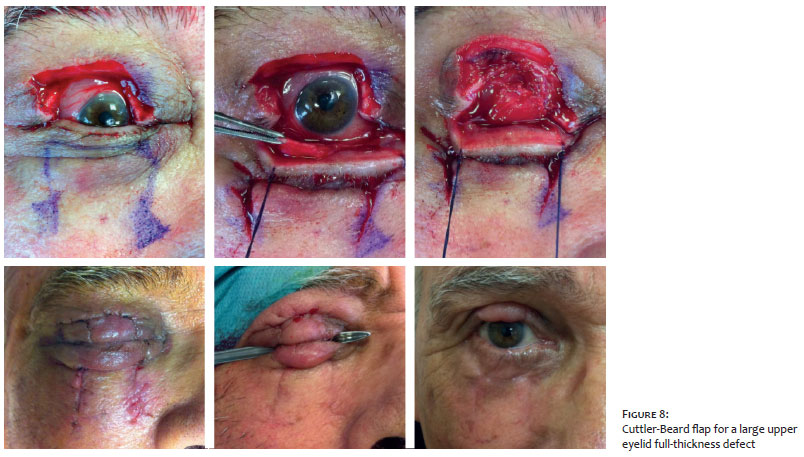
Defects larger than one half of the upper eyelid length are very difficult to repair and the options are very limited. The most reliable and safe procedure is the Cuttler-Beard flap,14 which consists of an advancement full-thickness flap harvested in the lower eyelid. Like the Hughes flap, it is an interpolated flap with a 4-6 weeks period before pedicle division. Since the Cuttler-Beard flap should not affect the lower eyelid margin, it is tunneled to achieve its final position over the upper eyelid defect.
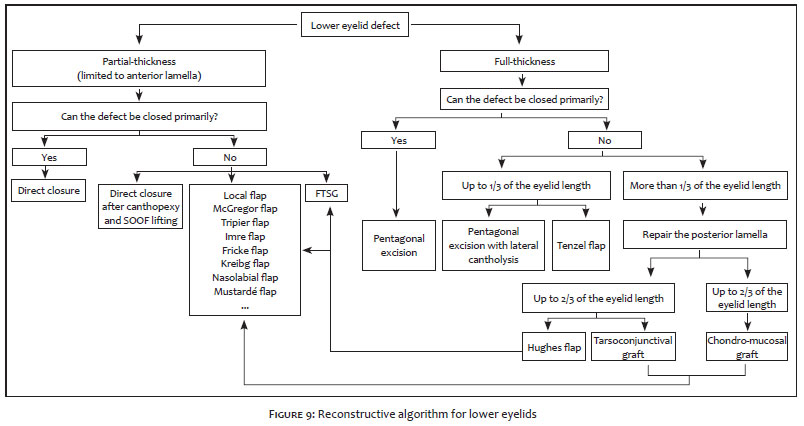
Algorithms. The final algorithms can be analyzed in the Figures 9 and 10.
Eyelid reconstruction is challenging due to the anatomic and physiologic particularities of the eyelids. The multiplicity of surgical techniques available, differences in defects thickness and size, and individual variations in skin mobility and elasticity make the reconstructive strategy difficult to establish.
The proposed algorithms summarize the most common reconstructive procedures for upper and lower eyelids defects, sequentially categorized under a dichotomic decision tree aiming to assist the dermatologic surgeon during the reconstructive decision-making process.
Ricardo Vieira | ORCID 0000-0002-5914-9171
Preparation and writing of the manuscript, author of figures 1 to 7, coauthor of the flowcharts of figures 9 and 10.
João Goulão | ORCID 0000-0001-8378-9569
Critical review of the original, author of Figure 8, coauthor of the flowcharts of of figures 9 and 10.
1. Pe'er J. Pathology of eyelid tumors. Indian J Ophtalmol. 2016;64(3):117-90.
2. Lo Torto F, Losco L, Bernardini N, Greco M, Scuderi G, Ribuffo D. Surgical treatmemnt with locoregional flaps for the eyelid: a review. BioMed Res Int. 2017;2017:6742537.
3. Hayano SM, Whipple KM, Korn BS, Kikkawa DO. Principles of periocular reconstruction following excision of cutaneous malignancy. J Skin Cancer 2012;2012:438502.
4. Subramanian N. Reconstructions of eyelid defects. Indian J Plast Surg. 2011;44(1):5-13.
5. Amici JM, Bailly JY, Taieb A. Horizontal stretching concept in oncologic dermatologic surgey of the face. J Eur Acad Dermatol Venereol. 2010;24(3): 308-16.
6. Scawn R, Gore S, Joshi N. Blepharoplasty basics for the dermatologist. J Cutan Aesthet Surg. 2016;9(2):80-4.
7. Vieira R, Brinca A, Pinho A. Repair of the lower eyelid with primary closure with lateral canthopexy and elevation of the suborbicularis oculi fascia: a simple technique to avoid post-operatory ectropion. Surg Cosmet Dermatol. 2018;10(4):346-8.
8. Machado WL, Gurfinkel PC, Gualberto GV, Sampaio FM, Melo ML, Treu CM. Modified Tripier flap in reconstruction of the lower eyelid. An Bras Dermatol. 2015;90(1):108–10.
9. Neto GH, Sebastia R, Viana GA, Machado F. Reconstrução palpebral com retalho de Fricke: relato de dois casos. Arq Bras Oftalmol. 2006;69(1):123-6.
10. Cogrel O. Mustarde flap lower eyelid reconstruction following lentigo maligna excisiom. Ann Dermatol Venereol. 2016;143(2):167-8.
11. Garcia GA, Nguyen CV, Vo TA, Yonkers MA, Minckler DS, Tao JP. Lazy pentagonal wedge resection of eyelid margin lesions. JAMA Facial Plas Surg. 2018;20(3):251-2.
12. Hawes MJ, Grove AS, Mink EM. Comparison of free tarsoconjunctival grafts and Hughes tarsoconjunctival grafts for lower eyelid reconstruction. Ophtalmic Plast Reconstruc Surg. 2011;27(3):219-23.
13. Yamamoto N, Ogi H, Yanagibayashi S, Yoshida R, Takikawa M, Nishijima A, et al. Eyelid Reconstruction Using Oral Mucosa and Ear Cartilage Strips as Sandwich Grafting. Plast Reconstr Surg Glob Open. 2017;5(4): e1301.
14. Mandal SK, Fleming JC, Reddy SG, Fowler BT. Total Upper Eyelid Reconstruction with Modified Cutler-Beard Procedure Using Autogenous Auricular Cartilage. J Clin Diagn Res. 2016;10(8):NC01–4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}