


Eckart Haneke1,2,3,4; Nilton Di Chiacchio5
Received on: 18/02/2019
Approved on: 14/03/2019
This study was performed at the Hospital do Servidor Público Municipal de São Paulo - São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Onychomatricoma is a tumor of the nail matrix with well-known clinical features; however, sometimes underdiagnosed. It is often mistaken for onychomycosis due to thickening of the nail plate. dermoscopy of the plate and its free margin allows the visualization of important features for the diagnosis, many times not seen with the naked eye.
Keywords: Dermoscopy; Nail Diseases; Nails/Pathology; Neoplasms
Onychomatricoma is a specific benign neoplasia of the nail apparatus and the only tumor in which the alteration of the nail plate is actively produced by the lesion. It occurs in the nail matrix with digitiform projections, causing changes in the nail. Thickening of the nail plate, longitudinal striae, yellowish staining and splinter hemorrhages are the most frequent clinical features. Clinical diagnosis is difficult not only due to the lack of knowledge about the tumor, but also when the lesion is small. Usually the nail plate lesion is mistakenly diagnosed and treated as onychomycosis. 1-3 Nail plate dermoscopy, nail clipping, ultrasonography, and magnetic resonance imaging are of assistance in the diagnosis. The treatment is surgical with the complete removal of the tumor, and anatomopathological examination defines the diagnosis.
Case 1: A 61-year-old white female patient complaining of a lesion in the second right finger's nail that had emerged three years before. She underwent systemic and topical antifungal therapy for one year without improvement, and denied the presence of any symptom.
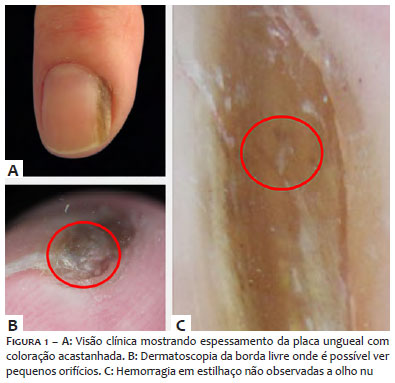
Clinical examination evidenced partial thickening of the nail plate on the outer side, as well as a yellowish coloration. Two points corresponding to hemorrhagic striae – which could not be seen with the naked eye – were observed by dermoscopy, as well as two small holes permeating the hyperkeratosis in the frontal view of the free part of the nail (Figure 1). In light of these findings, the hypothesis of onychomatricoma was raised. Ultrasonography was not performed due to financial constraints. The authors of the present study chose to surgically explore the lesion and perform an anatomopathological examination, which confirmed the clinical and dermoscopic hypothesis.
Case 2: A white, 54-year-old female patient presented a yellowish color in the right thumb's nail, with absence of subjective symptoms. It was treated as onychomycosis with topical ciclopirox, followed by 250mg terbinafine daily for four months without improvement.
Observation of the nail's free margin revealed circumscribed thickening with a few small holes. Dermoscopy (Figure 2) showed whitish shade of the lunula and long, stretched capillaries. This is characteristic of the tumor's digitiform projections and can reach the nail plate's holes (produced by the tumor) – and can be observed in the histological examination. Sometimes the capillaries reach the free end of the nail plate, with bleeding of the nail when it is cut.
The diagnosis of onychomatricoma is challenging for dermatologists.2
In addition to the clinical alterations, nail plate dermoscopy, nail clipping,4 ultrasonography,5 and magnetic resonance 3 provide assistance in the diagnosis. The dermoscope is already part of the dermatological examination routine and in many times avoids expensive – and often inaccessible – tests.
The tumor originated in the nail matrix has tufted appearance with digitiform projections forming and filling cavities extending from the proximal part to the free border of the nail. This explains the holes seen in the free part of the distal plate's border, as well as the presence of capillaries in the tunnels filled by the tumor's projections. The observed hemorrhagic striae occur due to punctual bleeding of nail capillaries.3 Dermoscopy of the nail plate provided assistance in the diagnosis in the described cases. The nail plate's yellowish coloration, hemorrhagic striae and orifices on the free border – not seen with the naked eye – became evident in Case 1. Changes in the color of the lunula and the presence of long capillaries running towards the plate's distal direction are characteristic and correspond to the tumor's digitiform projections, as observed in Case 2.
In face of the clinical findings and better visualization provided by the dermoscope, it was possible to diagnose onychomatricomas.
Eckart Haneke | ORCID 0000-0001-9957-1441
Case description, general review of the manuscript.l
Nilton Di Chiacchio | ORCID 0000-0001-9536-2263
Case description, preparation of the final version and review of the manuscript.
1. Di Chiacchio N, Tavares GT, Tosti A, Di Chiacchio NG, Di Santis E, Alvarenga L, et al. Onychomatricoma: epidemiological and clinical findings in a large series of 30 cases. Br J Dermatol. 2015;173(5):1305-7.
2. Di Chiacchio N, Tavares GT, Padoveze EH, Bet DL, Di Chiacchio NG. Onychomatricoma. Surg Cosmet Dermatol. 2013;5(1): 10-4.
3. Richert B, André J. L’onychomatricome. Ann Dermatol Venereol. 2011; 138(1):71-4.
4. Miteva M, Farias DC, Zaiac M, Romanelli P, Tosti A. Nail clipping diagnosis of onychomatricoma. Arch Dermatol. 2011;147(9): 1117-8.
5. Soto R, Wortsman X, Corredoira Y. Onychomatricoma: Clinical and Sonographic Findings. Arch Dermatol. 2009;145(12):1461-2.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}