


Danielle Claudino de Oliveira Costa1; Ada Regina Trindade de Almeida2; Maria Victoria Suarez Restrepo3; Liliana Bechelli de Oliveira Torloni1
Received on: 22/10/2018
Approved on: 04/01/2019
Study conducted at the institution: Hospital do Servidor Público Municipal de São Paulo, São Paulo (SP), Brazil.
Financial support: None
Conflict of interestss: None
INTRODUCTION: Stretch marks are an everyday challenge to the dermatologist. In the search for alternative therapies, we find 5-fluorouracil (5-FU) and microneedling for associating the following properties: inhibition of fibrosis, stimulation of collagen renovation and induction of skin pigmentation. Objective: To evaluate the efficacy and safety of 5-FU, in isolation or associated to microneedling, for the treatment of white stretch marks (striae alba).
METHODS: Comparative, double-blind study over 180 days, between 3 groups: Group A: microneedling and 5-FU; Group B intralesional 5-FU and Group C microneedling without medication. We measured improvement through a numerical scale of skin coloration, considering positive results those with reduction of the discrepancy between the adjacent skin and the stretch mark. We also evaluated patient satisfaction and irritation with each technique.
RESULTS: Group A achieved 10% of excellent clinical improvement, 10% very good and 60% mild. In group B, none of the patients had excellent of very good improvement. In group C, there was 20% of very good clinical improvement and 70% of mild.
CONCLUSIONS: All techniques showed some degree of improvement of the lesions. Therefore, we propose new studies comparing all three techniques, with a larger sample, to evaluate if more treatments would result in better results.
Keywords: Cosmetic Techniques; Fluorouracil; Striae Distensae; Therapeutics
Stretch marks are linear dermal scars associated to epidermal atrophy.1 It is a common clinical condition, prevalent in up to 80% of the population, being 2.5 times more frequent in females.2 Despite the high prevalence, little attention is given to this condition due to the absence of clinical impact. However, it represents an important cause for cosmetic concern, psychological and social stress.1,2
The pathophysiology is still unknown, but endocrine and genetic factors, as well as stretching of the skin are reported as triggers.3 It is believed the mechanical skin distension generates rupture of dermal elastic fibers. Local fibroblasts cannot reestablish the components of the extracellular matrix and the disorganization of collagen and elastic fibers contributes to the atrophic appearance of striae.3,4
In face of the multiple etiologic factors involved, the literature is conflicting and broad regarding treatment. Among the therapies, the most used are topical medications (retinoic acid, moisturizing creams, daily application of glycolic acid and/or peels), combined UVB/UVA1 phototherapy, lasers, microdermabrasion, radiofrequency, intradermotherapy and microneedling.5,6 We highlight that all existing options are usually costly and require prolonged treatment times.5
Microneedling utilizes a system with microneedles applied to the skin, with the goal of creating multiple micro-punctures, deep enough to reach the dermis. The injury would stimulate the expression of different growth factors in the skin (endothelial vascular growth factor, fibroblast growth factor and epidermal growth factor) and the synthesis of type I and III collagen, that promote remodeling of the extracellular matrix.6,7 This way, microneedling has a broad spectrum of indications when the objective is to stimulate collagen production. Many studies demonstrated this technique to be effective for the treatment of fine and medium wrinkles, skin laxity, facial rejuvenation and correction of scars, as well as improvement of old and early stretch marks.6,7,8
5-fluorouracil (5-FU) is a pyrimidine analogue that acts inhibiting the activity of the enzyme thymidylate synthase, that catalyzes the methylation of deoxyurydilic acid into thymidylic acid, interfering in DNA synthesis. Based in this property, this medication is widely used for the topical treatment of actinic keratoses, basal cell carcinomas and plane warts, being the intralesional application indicated for the treatment of keloids, hypertrophic scars and contractures.9,10,11 Moreover, this drug reduces the risk of excessive cicatricial fibrosis because it inhibits fibroblast proliferation and, due to this feature, is used in many surgeries such as, for example, glaucoma and tendon repair.12
Besides, experimental studies obtained relevant information on the biologic impact of this medication in melanocytes. In the presence of a low concentration of 5-FU, keratinocytes are selectively destroyed within 3 weeks, whereas melanocytes continue to multiply and form pigment.13 Based on this and other studies, 5-FU is also used for the treatment of vitiligo.14
According to Fulton et al, hypopigmented scars can repigment after mechanical removal of the dermal fibrosis.15,16 Consequently, Arbache et al described repigmentation of idiopathic guttate hypomelanosis after treatment with microneedling associated to 5-FU. With the help of biopsies, it was also verified that, after the procedure, there was an increase in the number of melanocytes, eliminating the possibility of post-inflammatory hyperpigmentation.17
There are no previous studies mentioning intralesional 5-fluorouracil or associated to microneedling to treat striae alba. However, this medication is successfully used in the treatment of scars, that have similar anatomopathological features to stretch marks, besides stimulant the production of pigment by melanocytes. Therefore, based on these properties, we opted for this drug in an attempt to improve the clinical appearance of striae alba, reducing the contrast between the adjacent skin and the involved skin.
Thus, this pilot study was conducted to evaluate the efficacy and safety of the association between the two techniques for the treatment of striae alba, comparing it to each technique alone.
Design
It is a randomized, double-blind, controlled clinical trial. Eighteen patients, phototype III, IV and V with striae alba located on both buttocks, seen at the Dermatology Clinic of the Hospital do Servidor Público Municipal de São Paulo, in December 2016, who signed the consent form, were selected.
Patients who received previous treatment for stretch marks in the 6 months prior, those with malignancies, cutaneous infection and personal history of keloids, pregnant and breastfeeding, with a history of allergy or hypersensitivity to 5-fluorouracil and those using systemic retinoids, topical or systemic steroids and immunosuppressant medications were excluded.
The right and left buttock of the patients were randomized and allocated into three groups: group A (treatment with microneedling and 5-fluorouracil), group B (treatment with intralesional 5-fluorouracil) and group C (microneedling with no medication). The list of randomization was revealed only to the investigator responsible for the treatment, and improvement criteria were evaluated by a blinded observer.
An area of 10cm2 was selected on each buttock, with higher density of stretch marks for the implementation of the treatment methods. In the same patient, the area was symmetrical bilaterally; only the site varied between patients.
All techniques were performed only once with topical anesthetic. In the groups receiving 5-FU, a maximum dose of 150mg (3ml) was used per area.
In group A, an electrical pen with a multi-needle tip (five needles), Dermograph Dermo Mag (Anvisa record number 80815530001) was used, which was dipped into a sterile container with 5-FU, absorbing the product by capillarity, and used to create micropunctures along the stretch mark. The pen was dipped into the container and back to the stretch mark many times until the whole extension of the lesion showed pinpoint bleeding and purpuric appearance.
Group B was treated with the injection of 5-FU along the stretch mark, in the dermis, through multiple punctures (0.1ml per puncture) with a 1-cm distance, using insulin syringes (1ml) and 30G needles. The same pen was used in group C to create multiple micropunctures along the stretch mark, with no added local medication, with the same endpoint of the first group.
The study included five visits on days zero, 2, 30, 90 and 180. On day zero, the selected techniques were applied and the photographic record prior to the procedure was made, as well as on the intermediate visits. On day 180, the efficacy and patient satisfaction with the treatment were evaluated.
Clinical evaluation of the lesions regarding the adjacent skin:
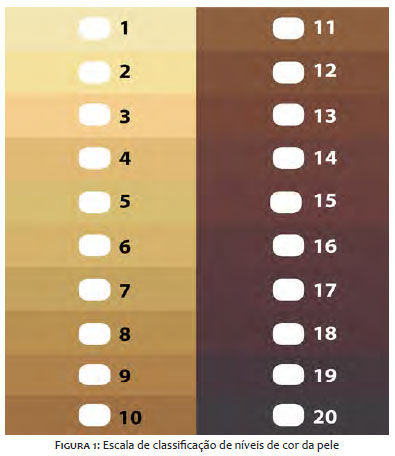
The stretch mark on the selected area, and the neighboring skin with no lesions were numbered separately, based on a numerical scale of skin color (Figure 1). The difference between the 2 numbers indicated one discrepancy between the healthy and injured skin (stria alba). Results were considered positive when there was a reduction in the difference between the 2 initial numbers, which were analyzed as follows:
Excellent: the stretch mark achieved the same skin tone as the adjacent normal skin.
Very good: the stretch mark achieved 1 point below the tone of the adjacent normal skin.
Good: the stretch mark achieved 2 points below the tone of the adjacent normal skin.
Mild: achieved less than 2 tones below the tone of the normal adjacent skin.
No improvement: it remained as in the beginning.
Worsening: achieved 1 or more skin tones below the initial color of the stretch mark (hypopigmentation).
Hyperpigmentation: achieved 1 or more tones above the tone of the normal adjacent skin.
The participant answered to the following question: how do you qualify the result of the treatment performed in each buttock? The patients could answer if it was very good, good, mild, no improvement or worse.
The parameters burning sensation, pruritus and erythema were evaluated by the participant of the study together with the investigator through a scale ranging from zero to three, considering the lowest score as absence of symptom and the highest as severe symptom.
An exploratory analysis was performed through means, frequencies and percentages. Results were compared with the chi-square test or the nonparametric test of Kruskal-Wallis, followed by the procedure of multiple comparisons of Dunn. The level of significance of 5% was considered.
In this study, 15 patients finalized the protocol and were evaluated according to the treatment received. The three excluded participants did not attend the scheduled visits. The incomplete balanced block design was used, i.e., each treatment was applied in 10 buttocks (right or left).
The age group of the participants ranged from 18 to 50 years, with a mean of 35 years. The main cause for the appearance of the stretch marks was weight gain (53.3%), followed by weight loss (13.3%). Other causes reported were steroid use and pregnancy.
Regarding the tone difference between the adjacent skin and the stretch mark in the first visit, it was at least 6 tones in 24 buttocks and at least 3 in 6 buttocks.
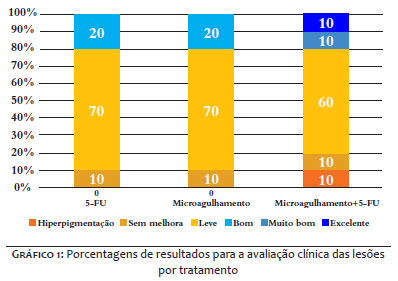
Of the 10 buttocks treated with microneedling+5-FU, an excellent improvement was seen in 10% (one buttock) and very good in 10% (one buttock). The group treated with microneedling alone achieved 20% (two buttocks) very good response and none with excellent improvement. Regarding 5-FU alone, 20% (two buttocks) showed good response, but none was excellent or very good. However, most buttocks treated with the different techniques showed mild improvement, with 60% (six buttocks) with microneedling+5-FU; 70% (seven buttocks) with microneedling; and 70% (seven buttocks) with 5-FU alone (Graph 1).
The percentage of patients with therapeutic failure was 20% (two buttocks) for the treatment of microneedling +5-FU, due to the absence of clinical improvement and the presence of hyperpigmentation maintained after 6 months of follow up. With the other techniques, there was 10% (one buttock) of therapeutic failure due to lack of clinical improvement.
A significant association between clinical improvement (defined as excellent of very good response) and the treatments evaluated (chi-square; p-value=0.315) was not found.
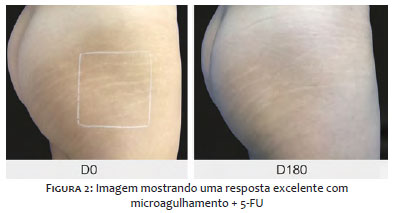
Figures 2, 3 and 4 illustrate the best results obtained with each technique applied in this study.
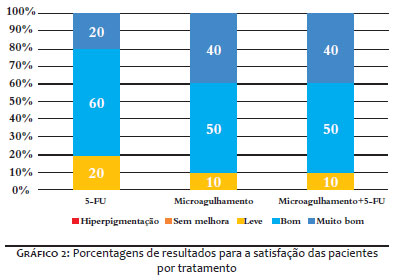
We observed that patient satisfaction for treatments with microneedling with or without 5-FU was considered very good for 40% (four), good for 50% (five) and mild for 10% (one). As for treatment with 5-FU alone, 20% (two) considered it very good, 60% (six) good and 20% (two) mild (Graph 2). A significant association between patient satisfaction and the treatments evaluated (chi-square; p=0.840) was not found.
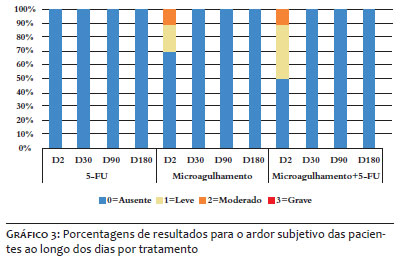
A significant difference between treatments regarding burning sensation on day two was found (Kruskal-Wallis; p=0.049). Burning sensation with treatment with microneedling+5- FU was significantly superior to the treatment with 5-FU alone. The difference for the treatment of microneedling alone in comparison to the others was not significant. On days 30, 90 and 180 there was no burning sensation for any of the treatments evaluated (Graph 3).
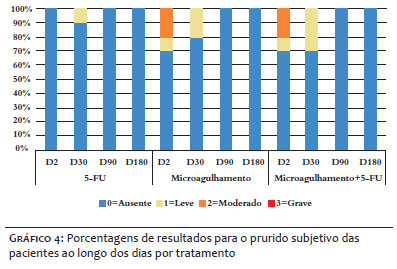
No statistically significant difference was seen between treatments regarding pruritus on day 2 (Kruskal-Wallis; p=0.167) and on day 30 (Kruskal-Wallis; p=0.547). On days 90 and 180, there was no pruritus for any of the treatments evaluated (Graph 4).
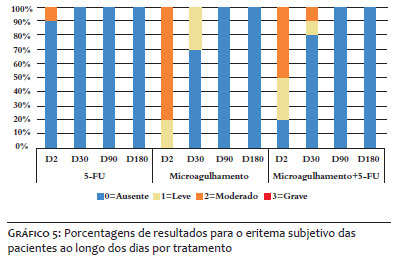
A significant difference was seen between treatments regarding erythema
On day 2 (Kruskal-Wallis; p<0.001). The erythema of the treatments with microneedling (microneedling and microneedling+5-FU) was significantly superior to the treatment with 5-FU alone. On day 30, there was no significant difference between treatment (Kruskal- l-Wallis; p=0.212). On days 90 and 180, there was no erythema for any of the treatments evaluated (Graph 5).
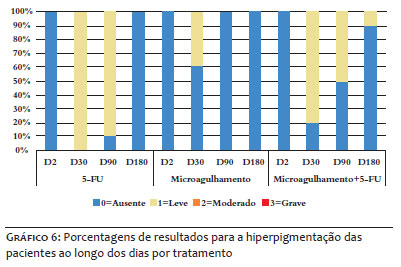
In the group treated with 5-FU, we observed that on day 30, all patients (100%) showed hyperpigmentation, with complete resolution of this adverse effect before the end of the study (day 180). Regarding microneedling alone, only 40% (four buttocks) of the cases showed hyperpigmentation on day 30, absent in the following visits. In patients treated with microneedling+5-FU, 80% (eight buttocks) showed hyperpigmentation on day 30, 50% (five buttocks) on day 90 and 10% (one buttock) maintained this adverse effect until the end of the study (Graph 6).
In this study, 20% of the buttocks treated with microneedling alone or associated to 5-FU had excellent or very good response. Despite the absence of statistical difference regarding the degree of improvement between the three techniques, it is worth highlighting that in the group of 5-FU alone, no buttock achieved an excellent or very good result. However, most buttocks treated with any one of the modalities achieved, at least, mild improvement of the lesions. The lack of statistical significance can be explained by the sample with reduced number participants or due to the single treatment application.
Nassar et al compared microneedling and microdermabrasion with sonophoresis for the treatment of stretch marks on the thighs and legs. In this study, they included 40 patients, 20 Treated with three sessions of microneedling and the remaining with 10 sessions of the other technique. They observed that, with microneedling, six (30%) showed excellent results and eight (40%) very good, against two patients (10%) with excellent response and six (30%) very good with the other technique.18 In a similar study, Park et al treated 16 patients with stretch marks in different locations with three sessions of microneedling without comparing it to other techniques. They observed an excellent improvement in seven (43.8%) patients and minimal to moderate improvement in nine (56.2%).7 In this protocol, we obtained 20% success with microneedling alone or associated to 5-FU with only one session.
In the study by El-Samad et al, 60 patients with vitiligo were treated with intralesional 5-FU associated to NB-UVB. As a result, there was increased global repigmentation on the side treated with 5-FU when compared to the one treated with NB-UVB alone, on all parts of the body (p <0.001).14 The study by Kalil et al suggests that the association of one medication or cosmetic formulation with microneedling could enhance the result in 28%.8 In this study, the group of 5-FU alone demonstrated a mild response in 70% of cases and good in 20%. In the group of microneedling with 5-FU, 10% achieved an excellent response; 10%, very good; and 60%, mild. Despite the difference between the techniques not being statistically significant, we believe that 5-FU associated to microneedling can be more effective.
Regarding patient satisfaction, the three treatments had good evaluations. The techniques of microneedling alone or associated to 5-FU were considered very good and good by 40% and 50% of the participants, respectively. In the group treated with 5-FU alone, we observed that 20% and 60% of patients considered the technique as very good and good, in this sequence. We concluded that, despite not having a statistical difference between the treatments, the level of satisfaction was higher in those patients submitted to the techniques with microneedling. This finding is positively correlated to the degree of improvement obtained with these techniques.
Regarding the subjective parameter of irritation, burning sensation was higher with microneedling and microneedling with 5-FU on day 2 (visit 2) when compared to burning sensation caused by the treatment with 5-FU alone. In the following visits, there was no burning sensation for any of the patients. This initial discomfort is explained by the use of needling, causing trauma to the skin, associated to the effect of burning sensation generated after 5-FU application, as reported in the literature.6,7,18
Pruritus from treatments with microneedling on day 2 (visit 2) and day 30 (visit 3) was also slightly worse when compared to the treatment with 5-FU alone. However, there was no statistically significant difference between the treatments. We verified that there are no publications reporting pruritus after these treatments, however, in this study, pruritus was mild and transient in most cases.
The erythema of treatments with needling was much more pronounced when compared to treatment with 5-FU alone on day 2 (visit 2). On day 30, the erythema was still slightly more intense in the treatments with microneedling. In 2013, Lima et al described that, after injury caused by microneedles in the skin, vascular ectasia and leakage of red blood cells take place in the dermis. Thus, erythema is explained by the presence of traumas with vascular involvement, being a desired effect in the removal of damaged subepidermal collagen followed by replacement by new collagen and elastin fibers.6
In this study, we determined that hyperpigmentation was present in the three treatment groups, however, it was more prevalent in patients treated with 5-FU alone on the visits of days 30 and 90 when compared to the other techniques. We observed that this effect disappeared before the end of this protocol, except for a patient treated with microneedling plus 5-FU, in which the stretch mark maintained the coloration of three tones above the color of the adjacent skin up until the last visit.
In all studies evaluated on the treatment of stretch marks with microneedling alone, we find only the citation of post-inflammatory hyperpigmentation, but transient in nature.7,18
The main limitations of this study were the small size of the sample and the restriction to one treatment session, whereas in the literature the final result was assessed after three sessions, as in the studies by Nassar and Park.7,18
In this study, there was excellent (10%) and very good (10%) clinical improvement in the cases treated with microneedling + 5-FU. Microneedling alone obtained a very good response in 20% of cases, while no patient showed excellent or very good responses with 5-FU alone. However, all techniques showed mild degree of improvement of the lesions.
This way, we verified that the groups treated with microneedling with or without 5-FU obtained excellent and very good results, not observed in those treated with 5-FU alone. These results correlated positively to the degree of patient satisfaction, that was higher among those being treated with needling therapies. However, there was no statistical difference in the two parameters evaluated.
We observed with all three techniques the presence of pain, burning sensation, pruritis and erythema, but predominantly mild and transient in nature. Of the 15 patients treated, residual hyperpigmentation persisted in only one. Thus, we conclude that the therapies are safe and well tolerated.
With this study we noticed that the application of more sessions would probably yield better clinical results. Therefore, we propose new studies comparing the three techniques, with a larger sample, to evaluate if more sessions would result in more expressive results.
To Doctor Ada Regina Trindade de Almeida for the support and encouragement given. I would also like to thank the trust of this spectacular teacher. To Doctor Maria Victoria Suarez Restrepo for the valuable guidance offered and to Doctor Liliana Bechelli de Oliveira Torloni, for the availability and for helping me in the execution of this study. To the friends: Jaqueline Guerra, Patrícia de Jesus Resende de Morais and Lelia Barbosa Freire for the invaluable collaboration. To the patients that participated in this project for believing in what was proposed.
Danielle Claudino de Oliveira Costa | ORCID 0000-0002-3238-6898
Design and planning of the study; preparation and writing of the manuscript; data collection, analysis and interpretation; intellectual participation in propaedeutics and/or therapeutics of the studied cases; critical literature review.
Ada Regina Trindade de Almeida | ORCID 0000-0002-4054-2344
Design and planning of the study; preparation and writing of the manuscript; hands-on participation in mentoring the research; intellectual participation in propaedeutics and/or therapeutics of the studied cases; critical literature review; critical review of the manuscript.
Maria Victoria Suarez Restrepo | ORCID 0000-0002-2614-6011
Statistical analysis; design and planning of the study; preparation and writing of the manuscript; data collection, analysis and interpretation; intellectual participation in propaedeutics and/or therapeutics of the studied cases; hands-on participation in mentoring the research; critical review of the manuscript.
Liliana Bechelli de Oliveira Torloni | ORCID 0000-0002-3876-3148
Data collection, analysis and interpretation; critical review of the manuscript.
1. Fatemi Naeini F, Behfar S, Abtahi-Naeini B, Keyvan S, Pourazizi M. Promising Option for Treatment of Striae Alba: Fractionated Microneedle Radiofrequency in Combination with Fractional Carbon Dioxide Laser. Dermatol Res Pract. 2016; Mar; 21 (2): 70-76.
2. Bertin C, Lopes-Da Cunha A, Nkengne A, Roure R, Stamatas GN. Striae distensae are characterized by distinct microstructural features as measured by non-invasive methods in vivo. Skin Res Technol. 2014 Feb; 20(1):81-6.
3. Mitts TF, Jimenez F, Hinek A. Skin biopsy analysis reveals predisposition to stretch mark formation. Aesthet Surg J. 2005 Nov-Dec; 25(6):593-600.
4. Cordeiro RCT, Moraes AM. Striae distensae: fisiopatologia. Surg Cosmet Dermatol.2009;1(3):137-140.
5. Crocco EI, Mantovani PA, Volpini BMF. Em busca dos tratamentos para Striae Rubra e Striae Alba: o desafio do dermatologista. Surg Cosmet Dermatol.2012;4(4):332-7.
6. Lima EVA, Lima MA, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol 2013;5(2):1104.
7. Park KY, Kim HK, Kim SE, Kim BJ, Kim MN.Treatment of striae distensae using needling therapy: a pilot study. Dermatol Surg. 2012 Nov;38(11):1823-8.
8. Kalil C, Campos V, Reinehr CPH, Chaves CRPC. Microagulhamento: série de casos associados drug delivery. Surg Cosmet Dermatol 2017;9(1):96-9.
9. Bijlard E, Steltenpool S, Niessen FB. Intralesional 5-Fluorouracil in Keloid Treatment: A Systematic Review. Acta Derm Venereol. 2015 Oct;95(7):778-82
10. Apikian M, Goodman G. Intralesional 5-fluorouracil in the treatment of keloid scars. Australas. J Dermatol 2004;45:140-3
11. Gupta S, Kalra A. Efficacy and safety of intralesional 5-fluorouracil in the treatment of keloids. Dermatology. 2002;204(2):130-2.
12. Metsavaht LD, Garcia CAR. Infiltrações intralesionais de 5-FU no tratamento de queloides, cicatrizes hipertróficas e contraturas. Surg Cosmet Dermatol 2015;7(1):17-24.
13. Gauthier Y, Anbar T, Lepreux S, Cario-André M, Benzekri L. Possible mechanisms by which topical 5-Fluorouracil and dermabrasion could induce pigment spread in vitiligo skin: an experimental study. ISRN Dermatol. 2013 Apr9;2013:852497.
14. Abd El-Samad Z, Shaaban D. Treatment of localized non-segmental vitiligo with intradermal 5-flurouracil injection combined with narrow-band ultraviolet B: a preliminary study. J Dermatolog Treat. 2012 ;23(6):443-8.
15. Fulton JEJ, Rahimi AD, Mansoor S, et al. The treatente of hypopigmentation after skin resurfacing. Dermatol Surg.2004;30:95-101.
16. Arbache S, Godoy C E. Microinfusão de medicamentos na pele através de máquina de tatuagem. Surg Cosmet Dermatol 2013;5(1):704
17. Arbache S, Roth D, Steiner D, Breunig J, Michalany NS, Arbache ST, de Souza LG, Hirata SH. Activation of melanocytes in idiopathic guttate hypomelanosis after 5-fluorouracil infusion using a tattoo machine: Preliminary analysis of a randomized, split-body, single blinded, placebo controlled clinical trial. J Am Acad Dermatol. 2018;78(1):212-215
18. Nassar A, Ghomey S, El Gohary Y, El-Desoky F. Treatment of striae distensae with needling therapy versus microdermabrasion with sonophoresis. J Cosmet Laser Ther. 2016 ;18(6):330-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}