


Giseli Petrone de Souza1,2; Marcio Soares Serra3,4
Received on: 27/05/2018
Approved on: 08/12/2018
This study was performed at the Centro de Dermatologia e Laser Petrone e D’Avila - Rio de Janeiro (RJ), Brazil.
Financial support: None
Conflict of interests: Giseli Petrone de Souza is a speaker for Merz Brazil
Actinic purpura is characterized by dark purple patches, mainly on photoexposed areas of the extensor surfaces of the arms and hands of elderly individuals. Thus far, there is no satisfactory treatment. We report the case of an 80-year-old patient who underwent treatment with two sessions of calcium hydroxyapatite filler application in the forearms, with good results.
Keywords: Collagen; Therapeutics; Purpura
Actinic or senile purpura is a dermal connective tissue disorder due to chronic exposure to the sun. This condition was described in 1818 by Bateman — the reason for which it is also known as Batemans purpura. It affects elderly individuals and is characterized by darkened purple macules, located in photodamaged areas of the skin, mainly in the hands and forearms.1 More recently, in 2007, the term dermatoporosis was proposed to describe the syndrome of fragility or chronic cutaneous insufficiency, caused by the progressive reduction of important structures of the skin. Dermatoporosis encompasses cutaneous atrophy, actinic purpura and pseudocysts. By the age 70-80, changes caused by dermatoporosis and its complications begin to emerge.2 With the aging population, the authors of the present paper believe that dermatoporosis will become much more frequent, and prophylactic measures and new treatments need to be studied.
An 80-year old Caucasian male patient, phototype I, had cutaneous atrophy, dark purple macules and erosions with hematic crusting on both forearms, the most intense picture in the left forearm (Figure 1). The main complaint corresponded to purplish macules that emerged with minimal traumas and remained for a long time. The patient had tried topical treatments with moisturizers, cumarin and heparin derivatives, without significant improvement.
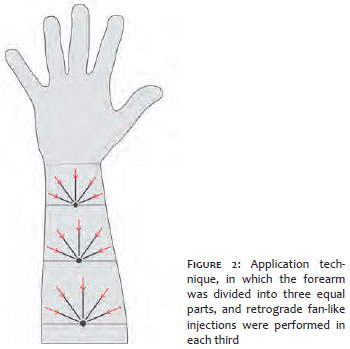
Two cutaneous filling sessions were performed using calcium hydroxyapatite (Radiesse®, Merz Aesthetics, São Paulo SP, Brazil). At each session, 1.5 ml calcium hydroxyapatite (CaHA) were diluted in 3 ml saline and 2% lidocaine in equal parts, amounting to the volume of 4.5 ml.3 The applications were performed by retrograde fan-like injections with a 22G x 2” cannula in the subdermal plane. The forearm was divided into three equal parts, with 1.5 ml of the diluted solution being used in each third (Figure 2). Two sessions were performed with an interval of 30 days. The patient chose to undergo treatment only in the left forearm on the justification that it was the most affected side. No additional topical treatment was prescribed, except for the use of SPF 30 sunscreen. Clinical improvement was observed shortly after the first session (Figure 3), with maintenance six months after the beginning of the treatment. Nonetheless, new lesions emerged in untreated areas, such as the back of the hand and the region close to the elbow (Figure 4).
Dermatoporosis can be a primary condition resulting from long exposure to the sun without the use of sunscreen, combined with advanced age. Alternatively, it can be iatrogenic and secondary to chronic topical or systemic use of corticosteroids, which induces cutaneous atrophy. Clinically, there are no differences between the primary and secondary iatrogenic forms; nevertheless, the secondary form can arise earlier and be more severe in patients with photodamage.4
It presents four clinical stages: Stage I - cutaneous atrophy, actinic purpura and pseudocysts; Stage IIa - superficial and localized small lacerations (< 3cm); stage IIb - large lacerations (> 3cm); Stage IlIa - superficial hematomas; Stage IlIb - deep hematomas without necrosis; Stage IV - large areas of necrosis without or with lethal complications.1,2
Actinic purpura results from an extravasation of blood into the dermis and even into the subcutaneous tissue after minimal trauma. It usually affects the extensor face of the forearms and hands, however legs, neck and face can also be affected. The surrounding skin is usually altered, becoming atrophic, pigmented and inelastic.1
Diagnosis is clinical, and histology shows thin epidermis on the dermis with decreased collagen fibers, which are progressively replaced by abnormal elastic fibers. The wall of the dermal vessels has normal tensile structure, however there is extravasation of red blood cells and hemosiderin deposition. In 10% of cases, there is neutrophilic infiltration, when differentiation with neutrophilic dermatoses and leukocytoclastic vasculitis becomes of importance.1
The use of sunscreen (UVA and UVB) with SPF greater than 50, which should be regularly used in photoexposed areas, remains the best treatment option. In theory, the use of 0.1% retinoic acid reverses serious skin damage caused by the sun, with regeneration of the dermis and reduction of abnormal elastic fibers. Nevertheless, some studies have not shown improvement of the actinic purpura plaques.1 On the other hand, the association of retinaldehydes and fragments of intermediate hyaluronates showed a greater synergistic effect on the proliferation of keratinocytes than if these substances were used separately.5,6 The use of cream containing epidermal growth factor led to increased skin thickness and decreased purpuric lesions when applied twice daily for six weeks.1,6,7 In turn, the use of oral citrus bioflavonoids mixtures showed an improvement of 50% of the purpuric plaques after six weeks in the studied group.1,6 Topical use of 1% dehydroepiandrosterone (DHEA) cream twice daily for four months improved epidermal atrophy associated with postmenopausal skin; while the oral use of DHEA for the prophylaxis of senile purpura needs further studies.6
The CaHA microspheres are uniform, have smooth surface and measure between 25 and 45 p. They have good biocompatibility and stimulate the production of collagen by means of an inflammatory process, leading to the formation of a fibrous capsule, being totally biodegraded after 14 months.8,9,10,11
The patient studied in the present paper was in Stage IIa (from a clinical point of view, Stages I and IIa are the most common).
CaHA was considered as a treatment option due to its biostimulating effect and its proven action in improving dermal thickness3,8,9,10 since in actinic purpura the lack of support and protection provided by the dermis around the vessels leads to the extravasation of red blood cells and hemosiderin in the dermis and in the subcutaneous and is not deemed a spontaneous rupture. Therefore, an increase in the thickness of the dermis can increase the protection of these dermal vessels. The authors of the present study also believe that this dermal thickening should compensate for the senile lipoatrophy that has been observed in several patients and that probably facilitates the increase of the trauma also due to the decrease of the subcutaneous cellular tissue — notwithstanding, these are observations that the authors of the present paper do not see reported in other articles published on the subject.
Histological and immunohistochemical studies show that CaHA increases the expression of collagens type I and III, as well as elastin and neovascularization, with peaks in the production of collagen between the fourth and seventh month.3 Using ultrasound imaging studies, it was possible to observe a significant increase in the dermal thickness in this period, however, with absence of change in the thickness of the epidermis.3
With aging, collagen becomes irregular and disorganized, leading to loss of the three-dimensional structure of the dermis, which adversely affects the fibroblasts’ function. The CaHA microspheres would act as a foundation for new tissue formation and fibroblast activation, with resulting formation of collagen and elastin. They are believed to promote a stable structure for fibroblast adhesion that is very similar to the one present in the young skin.3 As a result, it is possible to conclude that the production of new collagen within the extracellular matrix of the dermis results in better structural support, leading to greater firmness and elasticity of the skin. This in turn leads to fewer vascular ruptures resulting from minimal traumas, with less extravasation of red blood cells in the dermis, meaning there is clinical improvement of the actinic purpura.
The importance of the present case report is linked to the facts that it approached a pathology for which there is no effective treatment to date, and that the unprecedented use of CaHA as a therapy led to a satisfactory outcome, with a decrease in the severity of the clinical picture.
Giseli Petrone de Souza | ORCID 0000-0003-2853-2001
Evaluation, diagnosis and treatment of the patient, literature review, drafting of the manuscript, protocol implementation, bibliographical research.
Marcio Soares Serra | ORCID 0000-0002-0101-520X
Critical review and final drafting of the manuscript.
1. Karadag AS, Parish LC, Lambert WC. Senile Purpura as a stage of Dermatoporosis. Skinmed. 2017;15(2):91-2.
2. Kaya G. New therapeutic targets in Dermatoporosis. J Nutrit Health Aging. 2012;16(4):285-8.
3. Yutskovskaya Y, Kogan E. Improved neocollagenesis and skin mechanical properties of diluted calcium hydoxylapatite in the neck and décolletage: A pilot study. J Drugs Dermatol. 2017;16(1):68-74.
4. Kaya G, Saurat J-H. Dermatoporosis: a chronic cutaneous insufficiency/ fragility syndrome. Dermatology 2007;215(4):284-94.
5. Barnes L, Tran C, Sorg O, Hotz R, Grand D, Carraux P, et al. Synergistic effect of hyaluronate fragments in retinaldehyde-induced skin hiperplasia which is a Cd44-dependent phenomenon. PLoS One. 2010;5(12):e14372.
6. Dyer JM, Miller RA. Chronic Skin Fragility of Aging: current concepts in the pathogenesis, recognition, and management of dermatoporosis. J Clin Aesthet Dermatol. 2018;11(1):13-8.
7. McKnight B, Seidel R, Moy R. Topical human epidermal growth factor in the treatment of Senile Purpura and the prevention of Dermatoporosis. J Drugs Dermatol. 2015;14(10)1147-50.
8. Yutskovskaya Y, Kogan E, Leshunov E. A randomized, split-face, histomorphologic study comparing a volumetric calcium hydroxylapatite and a hialuronic acid-based dermal filler. J Drugs Dermatol. 2014;13(9):1047-52.
9. Pavicic T. Calcium hydroxylapatite filler: an overview of safety and tolerabity. J Drugs Dermatol. 2013;12(9):996-1002.
10. Van Loghem J, Yutskovskaya YA, Philip Werschler W. Calcium hydroxylapatite: over a decade of clinical experience. J Clin Aesthet Dermatol. 2015;8(1):38-49.
11. Berlin AL, Hussain M, Goldenberg DJ. Calcium Hydroxylapatite Filler for Facial Rejuvenation: A Histologic and Immunohistochemical Analysis. Dermatol Surg. 2008; 34(suppl 1):S64-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}