


Célia Luiza Petersen Vitello Kalil; Clarissa Prieto Herman Reinehr
Received on: 01/08/2018
Approved on: 20/11/2018
This study was performed at a private practice in Porto Alegre (RS), Brazil.
Financial support: None.
Conflict of interests: None.
INTRODUCTION: The treatment of unsightly hypertrophic scars secondary to surgeries in the thoracic region area challenging, particularly if associated to striae distensae. Surely, more than one therapy should be used, which will demand a long treatment time.
OBJECTIVES: To evaluate the effect of the association of fractional ablative and non-ablative lasers, microneedling and drug delivery in the management of hypertrophic scarring and striae distensae.
METHODS: Patient showing hypertrophic scars and striae on the anterior thoracic region was submitted to four monthly sessions of fractional ablative and non-ablative lasers, associated to microneedling and drug delivery.
RESULTS: At the end of the treatment protocol, the patient had improved mobility of the treated areas, quality of the skin and striae distensae in the treated region.
CONCLUSIONS: The associated treatment showed good results in the concurrent management of atrophic and hypertrophic scars.
Keywords: Cicatrix; Lasers; Needles
The treatment of unsightly scars secondary to skin grafts can be challenging — especially when the scars are associated with stretch marks. For this reason, the association of different techniques can be useful. The authors of the present paper describe the association of ablative fractional lasers (AFL) and non-ablative fractional lasers (NAFL), microneedling and drug delivery in the management of a clinical case.
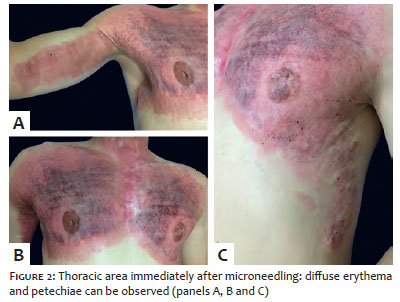
A 29-year-old male patient sought treatment for hypertrophic scarring in the anterior thoracic region, resulting from burns that happened in his childhood. The patient developed striae in the graft area during puberty, and hypertrophic scars emerged on the edges of this area (Figure 1). The proposed treatment consisted of NAFL and microneedling in the striae and AFL in the hypertrophic scars, followed by drug delivery throughout the region. Four sessions were performed observing monthly intervals. As a preparation, topical anesthetic cream with 4% lidocaine was applied 30 minutes before the procedure. The treatment protocol included the application of 1,340nm Er:YAG NAFL (Etherea MX®, Vydence Medical, São Paulo, Brazil): 8mm tip, 100-110mtz / cm2, 100mJ / mtz, 5ms, 3-4 passes, in the stretch marks area, followed by the application of rollers with 1.5mm microneedles (Dr. Roller®, Moohan Enterprise CO., Gyeonggido, South Korea) in back-and-forth motion, 10 to 15 times vertically, horizontally and diagonally, with up to 250-300 punctures / cm2, up until the emergence of punctiform bleeding on the cutaneous surface (Figure 2). The next step consisted of the application of 10,600nm CO2 AFL (Sculptor CO2®, Vydence Medical, São Paulo, Brazil), first pass: tip 300, random mode, 100mJ energy, density 100mtz / cm2; second pass: tip 800, brush mode, energy 26-80mJ, 125-200Hz, in the hypertrophic scars located at the edges of the graft areas. Immediately after the procedure, anhydrous serum for drug delivery containing 5% IGF + 1.5% EGF + 2% IDP + 1.5% Peptides + 2% Hyaxel + 1.5% Omega active + 4% Matrixil 3000 + 4% Hydroxyprolysilane. This formulation was also applied twice a day at home by the patient for the first three days after the procedure.
The evaluation performed three months after the last session showed improvement of the skin’s texture and reduction of the induration in the hypertrophic scars located laterally to the grafts. In addition, a reduction in the width of the stretch marks and overall improvement in the skin’s quality of the region were observed (Figure 3). The patient reported improved mobility of the thoracic region associated with the observed clinical improvement.
Microneedling and fractional lasers are options in the management of stretch marks and scars.1-3 In addition, they enable drug delivery after their implementation, increasing the permeation of the medications applied on the skin.4
The treatment of scars and stretch marks with microneedling results from the epidermal and dermal remodeling promoted by the procedure: the epidermis’ thickness can be increased up to 205%, while the dermis’ connective tissue reveals an increase in its density.3,5 In addition, microneedling increases the stratum corneums permeability during the first 48 hours after the procedure, and this time can be further increased by occlusion — which is why water-repellent anhydrous drug delivery was used.6 The used drug delivery formulations components contain active principles that stimulate neocollagenesis and elastin synthesis (such as Hydroxyprolisilane and Matrixil 3000), and others that inhibit collagenase (such as Omega active).
Regarding the use of lasers in the treatment of scars, NAFLs are described in isolation or associated with AFLs for the treatment of stretch marks and scars, with improvement in the skin’s texture, dyschromia and vascularization.1 Moreover, NAFL allows the treatment of all types of scars.1 Ablative fractional lasers can yield positive results in the reduction of the scars and cutaneous surfaces induration, especially in the case of hypertrophic scars.2
There are many unanswered questions regarding the association of the use of fractional lasers and microneedling. The authors’ perception regarding the present case is that this combination is synergistic and can lead to outcomes that are superior to those observed when the procedures are performed separately.
Based on the literature review, the present report is the first to describe the association between AFL, NAFL and microneedling, combined to the drug delivery technique, for the treatment of scarring and stretch marks. The authors chose the combination of these methods aimed at covering both the treatment of hypertrophic lesions and that of atrophic lesions, since the patient had both.7 The associated treatment of both pathologies has shown that it is possible to approach atrophic and hypertrophic cicatricial lesions concomitantly, with good results.
Although our patient had good clinical response, the main limitation of the present study stems from the peculiarity of the case — association of atrophic and hypertrophic lesions in the same body region — meaning it is an isolated case. In light of this fact, studies with larger sample sizes or comparing results obtained with each of the techniques, both in isolation and in association, will be welcome.
Célia Luiza Petersen Vitello Kalil | ORCID 0000-0002-1294-547X
Approval of the final version of the manuscript; study design and planning; preparation and drafting of the manuscript; research guidance; intellectual participation in the propaedeutic and / or therapeutic approach of studied cases; critical review of the literature; critical review of the manuscript
Clarissa Prieto Herman Reinehr | ORCID 0000-0003-1811-4519
Approval of the final version of the manuscript; study design and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; research guidance; intellectual participation in the propaedeutic and / or therapeutic approach of studied cases
1. Waibel J, Wulkan AJ, Lupo M, Beer K, Anderson RR. Treatment of burn scars with the 1,550 nm nonablative fractional Erbium Laser. Lasers Surg Med. 2012;44(6):441-6.
2. Poetschke J, Dornseifer U, Clementoni MT, Reinholz M, Schwaiger H, Steckmeier S, et al. Ultrapulsed fractional ablative carbon dioxide laser treatment of hypertrophic burn scars: evaluation of an in-patient controlled, standardized treatment approach. Lasers Med Sci. 2017;32(5):1031-1040.
3. Aust MC, Knobloch K, Reimers K, Redeker J, Ipaktchi R, Altintas MA, et al. Percutaneous collagen induction therapy: an alternative treatment for burn scars. Burns. 2010;36(6):836-43.
4. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
5. Zeitter S, Sikora Z, Jahn S, Stahl F, StrauB S, Lazaridis A, et al. Microneedling: matching the results of medical needling and repetitive treatments to maximize potential for skin regeneration. Burns. 2014;40(5):966-73.
6. Gupta J, Gill HS, Andrews SN, Prausnitz MR. Kinetics of skin resealing after insertion of microneedles in human subjects. J Control Release. 2011;154(2):148-55.
7. Khatri KA, Mahoney DL, McCartney MJ. Laser scar revision: A review. J Cosmet Laser Ther. 2011;13(2):54-62.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}