


Luciana Pereira Paes Gomes Saraiva; Mayara Brito de Nascimento; Alexandre de Almeida Filippo; Paula Regazzi de Gusmão
Received on: 25/09/2018
Approved on: 26/12/2018
This study was performed at the Instituto de Dermatologia Professor Rubem David Azulay, Santa Casa de Misericórdia do Rio de Janeiro, Rio de Janeiro, Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Despite all the existing therapeutic tools, melasma continues to be a dermatological challenge. Therefore, the search for new treatment modalities aims to optimize results and reduce systemic side effects.
OBJECTIVE: Evaluate the clinical improvement of patients with melasma treated with robotic micro-needling associated to drug delivery of tranexamic acid.
MATERIAL AND METHODS: Seventeen women with melasma were selected to be treated during eight weeks with four fortnightly sessions of robotic microneedling associated to drug delivery of 1.0ml of 4mg/ml tranexamic acid. The group was evaluated before and after the treatment with the following parameters: photographic evolution evaluated by three examiners, self-evaluation with Melasma QoL and MASI improvement.
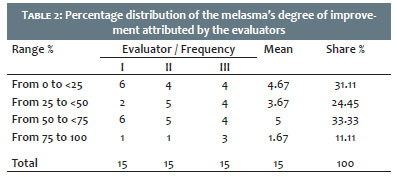
RESULTS: Fifteen Fitzpatrick phototype II to VI patients completed the study. Of those, 31.11% showed little or no improvement; 24.45% moderate to intermediate improvement; 33.33% significant improvement and 11.11% improved almost to resolution. In regards to MASI, there was a significant improvement, with a reduction from 21.33% to 11.19%.
CONCLUSIONS: The proposed association showed satisfactory results, constituting an innovative, replicable and safe therapeutic modality for the treatment of melasma.
Keywords: Combined modality therapy; Hyperpigmentation; Tranexamic acid
Melasma is an acquired chronic hyperpigmentation that affects areas of the skin that are exposed to the sun. It occurs in all ethnicities and in both genders, predominating in women of childbearing age and higher skin phototypes.1 Its prevalence in the population is of 1% to 50% and the explanation for this variation lies in the ethnicity and the ultraviolet radiation index of each of the geographic locations studied.2
It is clinically manifested by brownish, asymptomatic, generally symmetrical macules, distributed on the face in three main clinical patterns: centrofacial, malar and mandibular. The centrofacial pattern is the most prevalent, affecting approximately 50% to 80% of cases.3
Its etiology is multifactorial and the exact pathogenesis remains unknown, however it is known that ultraviolet radiation is a major factor. Other conditions are the use of oral contraceptives, hormonal treatment, pregnancy 4 and family history1. Recent studies indicate that 55%-64% of the cases have a positive family history, suggesting the existence of genetic predisposition to melasma.4 Less commonly observed factors are thyroid dysfunction, phototoxic medications, anticonvulsants and contact dermatitis due to the use of cosmetics.5 Nevertheless, most of the cases in men and a third of cases in women are idiopathic.6
The following therapies are used in the treatments of melasma: topical and oral depigmenting and antioxidant agents, chemical peels, and technologies such as robotic microneedling and 1,064nm Q-Swchited laser. More recently, studies have demonstrated that pulsed dye laser can be an option for melasma with predominance of vascular component.7
The most used drug delivery method in dermatology is the topical route. It has many advantages when compared to systemic pathways regarding side effects and patient adherence. However, the epidermis’ barrier function is ensured by the stratum corneums lipid bilayer, which is the main limiting factor for the delivery of drugs that have to be applied to the skin. The drug delivery technique consists of optimizing this penetration into the skin, using chemical, physical and mechanical methods.8
In spite of all existing therapeutic armamentarium, controlling melasma still remains a dermatological challenge, mainly due to its recurrence, refractoriness and aesthetic impairment to the patient. In this manner, the search for new therapeutic modalities — and even combinations of them — are aimed at potentiating the beneficial effects and minimize undesirable systemic effects, maintaining efficacy and safety.
In this context, robotic microneedling combined with drug delivery arises as a minimally invasive method that is safe in all skin types, and can be performed at a medical practice under topical anesthesia. Its main objective is to induce the process of dermal remodeling, including neocollagenesis and neoelas-togenesis, leaving the epidermal layer virtually untouched. It is effective in reducing epidermal melanic pigmentation,9 as well as allowing the delivery of depigmenting skin agents.
As a depigmenting agent, the authors of the present study propose the use of tranexamic acid, since it is a compound approved by the US FDA for the treatment of hypermenorrhea, epistaxis, hematuria, hereditary angioedema and bleeding prevention in major surgeries.10 In addition it has been used in the treatment of melasma since Nijor first reported its effectiveness in Japan, in 1979.11
It is a systemic analogue of lysine and an antifibrinolytic agent, since it blocks the conversion of plasminogen (present in the epidermal basal cells) into plasmin by inhibiting the plasminogen activator.1,4 It also acts by blocking the interaction between melanocytes and keratinocytes, resulting in inhibition of melanin synthesis.6
Plasmin activates the secretion of phospholipase A2 precursors, which act in the production of arachidonic acid and induce the release of fibroblast growth factor (bFGF) .12
It is a potent melanocyte growth factor.13 On the other hand, arachidonic acid is the precursor of melanogenic factors, such as prostaglandins and leukotrienes.14
The plasminogen activator is generated by keratinocytes and increases the in vitro activity of melanocytes. Its serum levels increase with the use of oral contraceptive and during pregnancy. The blocking of this substance may be the paracrine mechanism by which tranexamic acid reduces hyperpigmentation of melasma.14
It is already widely used clinically, through oral and par-aenteral routes, in tablets and injectable solution. A safe dose is deemed to be that of 25 to 50 mg/kg/day — generally 1,000 mg three times a day.10,15 Allowed pediatric use is 10 mg/kg, three times a day. In melasma, 250 mg twice a day is used, corresponding to one-sixth of the conventional hemostatic dose. The most commonly reported adverse effects in the literature are dizziness, tinnitus, headache, menstrual irregularity, hypotension, abdominal distension and pain, heartburn, nausea, vomiting and diarrhea.3,6 Thromboembolism, pulmonary embolism and acute myocardial infarction are rarely reported.13 Therefore, concern about prescribing tranexamic oral acid for patients is indisputable. It is considered as Category B in pregnancy and ofvery low risk during lactation.
In order to maintain and possibly improve the therapeutic efficacy with the decrease of the side effects of the systemic treatment, the authors of the present study used for drug delivery sterile vials of 4mg/ml tranexamic acid — a dose that is well below the one recommended for antifibrinolytic effect.
The objective of the authors of the present study was to evaluate the effectiveness of the robotic microneedling technology associated to drug delivery of tranexamic acid, a compound that has already been studied and established as a depigmenting agent and a safe alternative, with a low complication rate, and which can be applied in all skin types with a minimum period of downtime.
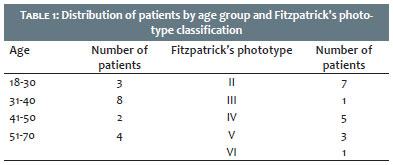
An interventionist, open-ended, prospective study was carried out at the Laser Sector of Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia do Rio de Janeiro (RJ, Brazil), where seventeen volunteer patients bearers of facial melasma in the age group from 18 to 70 years, with all skin phototypes, were selected (Table 1).
The selection process was based on the referral of specialist physicians from the Cosmiatry and General Dermatology Sector and the Laser Sector of Instituto de Dermatologia Professor Rubem David Azulay. The study was approved by the Research Ethics Committee (90268418600005239).
Inclusion criteria were: patients of both genders and all races, aged over 18 years, presence of clinical diagnosis of facial melasma; not to be in use of topical or oral treatment for melasma for a minimum of one month from the start of the study and no use of other medications for melasma during the proposed treatment.
Exclusion criteria were: pregnancy or lactancy; allergy to topical anesthetics; previous personal history of hypersensitivity to the study medication; patients with thromboembolic disease, active intravascular coagulation and acute occlusive vasculopathy; recent exposure to sunlight; previous use of tetracycline or other photosensitizing medication; use of oral tranexamic acid or oral anticoagulant; and presence of active dermatological lesion.
Patients underwent photographic documentation, MASI (Melasma Area and Severity Index) calculation, and Melasma QUOL (Melasma Quality of Life Scale) questioning before and four weeks after the end of the study protocol.
The procedure was carried out with patients under topical anesthesia with 4% lidocaine fro at least 30 minutes before the session. Robotic microneedling was performed (Eletroderme, Solon, LMG, ANVISA 80520090012) with a 2mm tip, without using radiofrequency, up until the end point was reached (light pinpoint bleeding on the skin). Subsequently, 1ml of 4mg/ml tranexamic acid was dripped (0.5 ml on each hemiface), in the area affected by melasma, with contact maintained for 6 hours. The interval between each of the 8 proposed sessions was 15 days.
An objective clinical evaluation was performed at the end of the study period by three “blind / hidden” dermatologist physicians who assessed the photographs taken in chronological order using an improvement scale graded with quartiles: Grade 1 (<25% = minimum improvement / absence of improvement); Grade 2 (26-50% = (moderate-intermediate improvement); Grade 3 (51-75% = important / marked improvement); Grade 4 (> 75% = improvement close to resolution).
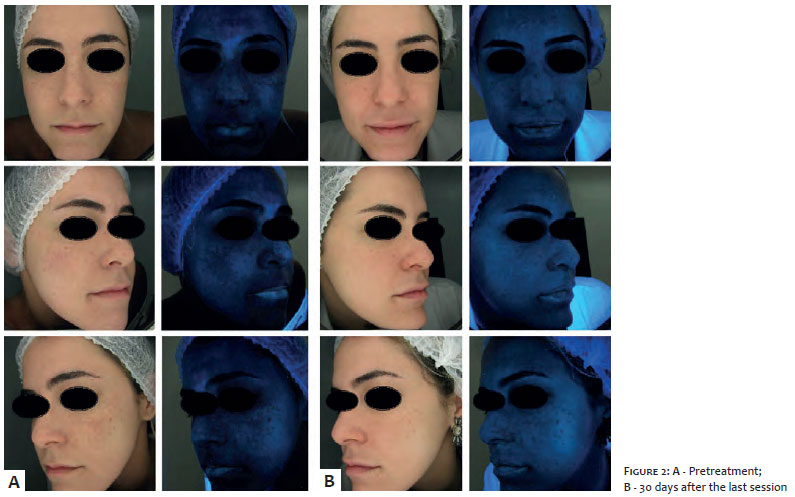
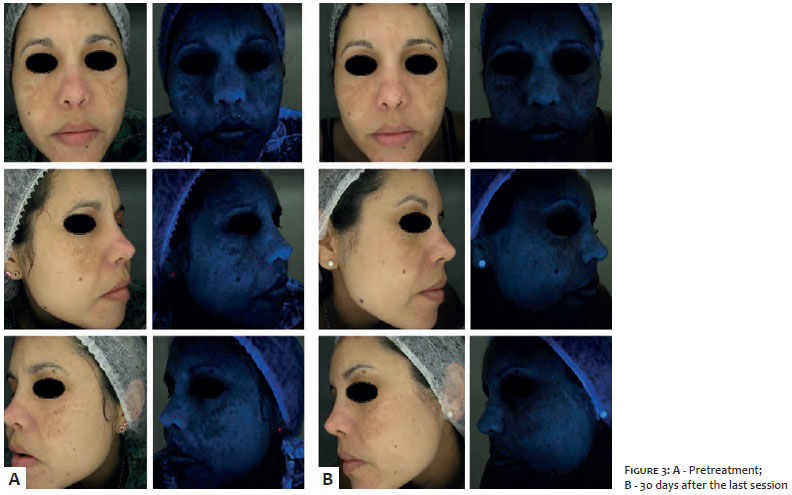
In order to obtain comparative images, the photographs were standardized using the Magic Mirror softwares camera under conventional and UV lighting — a valuable tool that heightens pigmentation visualization.
Of the seventeen patients selected for the study, 2 lost continuity, therefore, only fifteen reached the end of the treatment. They were all female, with a mean age of 42 years and mean duration of melasma development of 8.65 years.
Table 2 shows the distribution of results and percentage participations according to the photographic analysis carried out by the “blind / hidden” evaluators (I, II and III) on the 15 patients.
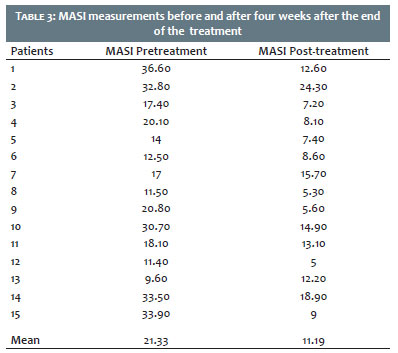
Regarding the MASI index, there was significant improvement (on average from 21.33 to 11.9) (Table 3).
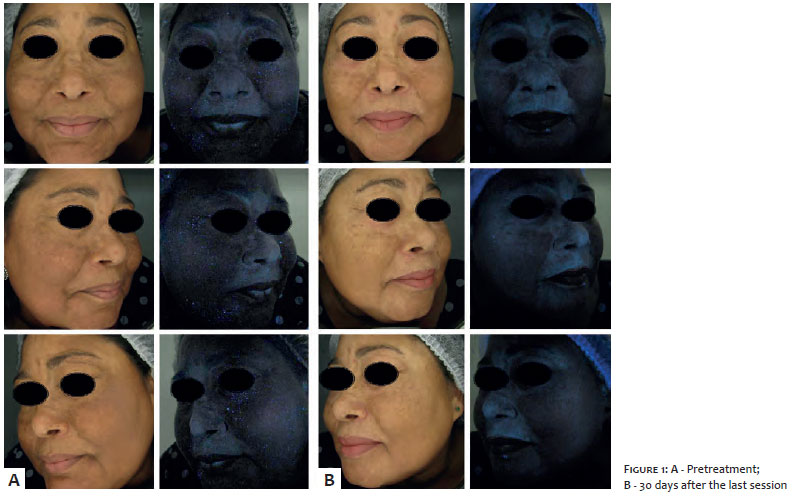
In most patients, the clinical response was already perceptible from the third session, nevertheless photographic documentation was performed only 30 days after the end of the last session (Fig 1, 2 and 3).
Tranexamic acid has been used in dermatology since 1979, when Nijor first reported its efficacy in the treatment of melasma.11 Since then, some studies have compared its efficacy across different routes of administration. Oral, intravenous, topical and intradermal (by microinjection and microneedling) uses have been described in the literature.
Its oral use has been widely reported in the literature. A study carried out by Na et al. demonstrated improvement in 22 women treated for eight weeks with 250 mg, three times per day, in combination with topical medication. In addition to the clinical improvement, there was evidence of reversal of the histological findings of melasma; reduction of epidermal pigmentation, and reduction of vascular proliferation, which correspond to the antiangiogenic effect of tranexamic acid.16 A Chinese study with 74 patients under oral treatment (twice per day for six months) observed improvement in 82.4% of patients, with responses observed in the first two months, and no significant side effects.6 In another Pakistani clinical trial carried out with 65 patients, 86% experienced clinical improvement (at the 6-month follow up 87% did not present recurrence), with absence of significant side effects.17 Another retrospective analysis carried out from January 2010 to June 2014, studied 561 patients using tranexamic acid as an adjuvant to the use of lasers or topical therapy, with improvement in 89.7% of patients, and first clinical signs appearing at 2 months. In this series, however, one patient had deep venous thrombosis 6 weeks after starting treatment.13
These and other studies prove the effectiveness of the oral use of tranexamic acid for the treatment of melasma. Not-withstanding, in a recent 2017 study by Sharm et al., 100 patients were divided into two groups: one group used oral 250mg tranexamic acid twice a day for 12 weeks, while the other used 4 mg/ml intradermal tranexamic acid monthly. The results showed that the difference between the two methods was not significant, however, the oral treatment took longer to yield perceivable clinical results. It was concluded, therefore, that the administration of tranexamic acid is effective and safe, independently of the route of administration.12 For this reason, the authors of the present study chose not to use the systemic route.
In addition, in 2009, Steiner et al. have demonstrated that tranexamic acid is a promising depigmenting agent in the treatment of melasma, even if it is not administered orally. Seventeen women were selected and treated for 12 weeks. One group used topical 3% tranexamic acid twice a day while another under-went weekly intradermal injections of 0.05 ml. The groups were compared before and after the treatment based on photographs, the MASI index, self-assessment and colorimetry. The MASI evaluation showed that the group using topical treatment saw improvement in only 12.5% of patients, while in the group un-dergoing injections that percentage was 66.7%, meaning that the therapeutic effect of tranexamic acid is enhanced when it crosses the bilipidic layer barrier of the cell membrane.1,18 Furthermore, in another study with the isolated use of topical treatment with tranexamic acid, twice a day for 12 weeks, in 21 patients with epidermal and mixed melasma, led to results similar to those of the placebo group, with worsening of erythema on the treated side.19
The first pilot study using pure microneedling in melasma was published in 2011, on the International Journal of Plastic Surgery. It assessed 20 patients whose one of the hemifaces was treated with an isolated whitening formulation, while the other underwent microneedling associated with the same substance. The photographic comparison showed that the hemiface with microneedling had an expressive improvement as compared with that was isolatedly treated with the whitening formulation (MASI: from 19.1 to 9.2 vs. from 20.4 to 13.3),5 demonstrating the importance of the drug delivery method. Aligned with this view, Budamakuntha et al. compared the efficacies of intradermal and microneedling based administration of tranexamic acid in a group of 30 patients. Although the results were not statistically significant, MASI improvement was greater in the microneedling group (44.41% vs. 35.72%),20 which is in line with the expressive results that the authors of the present study obtained with this treatment technique (also evidenced by the reduction of the MASI indices).
According to the studied literature, the results obtained do not show significant differences in the degree of improvement of melasma when comparing the oral and intradermal routes of administration.
Therefore, the authors of the present studys proposal to combine the depigmenting effect of tranexamic acid with robotic microneedling in order to minimize undesirable systemic effects led to results similar to those of the reviewed literature, since this technology allows to potentiate the local effect of the medication, given that it is delivered at a 2mm depth in the skin.
The side effects verified in the present study were minimal. Two patients noticed an initial worsening after the second session — especially of the vascular component, which improved with subsequent sessions.
One patient observed the emergence of erythematous papules, which were linked to the use of the healing cream and have been resolved after the product was replaced by a diverse one.
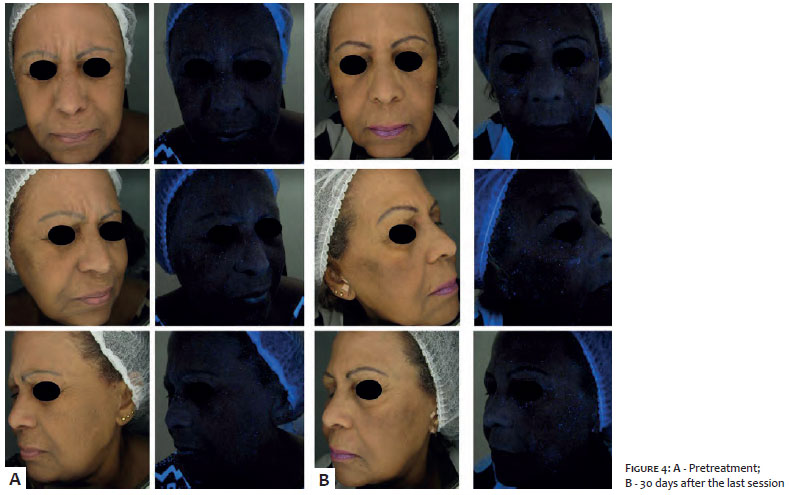
There was only one patient who had an increase in MASI after the end of treatment, with the worsening of the clinical picture having been observed and attributed to a trip to Bahia (Northeast Brazilian State), with frequent exposure to the sunlight for 14 days (Fig. 4).
Despite the algic component during the procedure, all patients found it tolerable and none decided to drop out of the study for this reason.
It should be noted that the study was limited to a small number of patients, with no control group, with a short duration and possible evaluation bias, given the MASI index is a subjective method of analysis of results. On the other hand, it is the most widely used, thus contributing to validate the results obtained.
The therapeutic response was considered very satisfactory, since the patients did not use any other treatment during the period of the clinical trial and obtained results that were already visible on the forty-fifth day of treatment, with good tolerability and absence of adverse effects, even when carried out in high skin phototypes.
The present study can be deemed as promising and the analyzed association can become a new therapeutic modality for melasma, especially in difficult-to-control cases, when there are contraindications to the use of the medication by systemic route and in high skin phototypes.
Although additional studies involving a greater number of participants are necessary to define optimal dosage, frequency of sessions, benefits and maintenance of the outcomes, the absence of adverse effects and degree of satisfaction obtained in the present study allow the authors to conclude that the association of robotic microneedling with drug delivery of tranexamic acid is a innovative, reproducible, safe and relatively cost-effective proposal.
Luciana Pereira Paes Gomes Saraiva | ORCID 0000-0003-1138-6255
Study design and planning; preparation and drafting of the manuscript, data collection, analysis and interpretation; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the literature; critical review of the manuscript.
Mayara Brito de Nascimento | ORCID 0000-0001-7991-1058
Study design and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; intellectual participation in the propaedeutic and / or treatment of the cases studied; critical review of the literature; critical review of the manuscript.
Alexandre de Almeida Filippo | ORCID 0000-0001-9550-5156
Approval of the final version of the manuscript; study design and planning; effective participation in the research guidance; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the manuscript.
Paula Regazzi de Gusmão | ORCID 0000-0002-7060-6062
Approval of the final version of the manuscript; study design and planning; effective participation in the research guidance; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the manuscript.
1. Steiner D, Feola C, Bialeski N, Silva FAM, Antiori ACP, Addor FAS, et al. Estudo da avaliação da eficácia do ácido tranexâmico tópico e injetável no tratamento do melasma. Surg Cosmet Dermatol. 2009;1(4):174-7.
2. Miot LD, Miot HA, Silva MG, Marques ME. Physiopathology of melasma. An Bras Dermatol. 2009;84(6):623-35.
3. Ogbechie-Godec OA, Elbuluk N. Melasma:an up-to-date comprehensive review. Dermatol Ther. 2017;7(3):305-18.
4. Hsiao CY, Sung HC, Hu S, Huang CH. Skin Pretreatment with conventional non-fractional ablative lasers promote the transdermal delivery of tranexamic acid. Dermatol Surg. 2016;42(7):867-74.
5. Fabbrocini G, De Vita V, Fardella N, Pastore F, Annunziata MC, Mauriello MC, et al. Skin Needling to Enhance Depigmenting Serum Penetration in the treatment of Melasma. Plast Surg Int. 2011;2011:1-7.
6. Li JY, Geddes ER, Robinson DM, Friedman PM. A review of melasma treatment focusing on laser and light devices. Semin Cutan Med Surg. 2016;35(4):223-32.
7. Hsiao CY, Sung H, Hu S, Huang C. Fractional CO2 Laser treatment to Enhance Skin Permeation of Tranexamic Acid with Minimal Skin Disrup-tion. Dermatology. 2015; 230(3):269-75.
8. Célia K, Valéria C, Clarissa PHR, Christine RPC. Drug delevery assistido por lasers: revisão. Surg Cosmet Dermatol. 2016;8(3):193-203.
9. Lima EA. Microagulhamento em melasma facial recalcitrante: uma série de 22 casos. An Bras Dermatol. 2015;90(6):917-9.
10. Puri N. Oral Tranexamic Acid Versus Triple Combination for The Treatment of Melasma. J J Expt Derm Res. 2015;1(4):018.
11. Nijor T. Treatment of melasma with tranexamic acid. Clin Res. 1979; 13:3129-31.
12. Sharma R, Mahajan VK, Mehta KS, Chauhan PS, Rawat R, Shiny TN. Therapeutic efficacy and safety of oral tranexamic acid and that of tranexamic acid local infiltration wich microinjections in patients with melasma: a comparative study. Clin Exp Dermatol. 2017;42(7):728-34.
13. Lee JH, Park JG, Lim SH, Kim JY, Ahn KY, Kim MY, Park YM. Localized Intradermal Microinjection of Tranexamic Acid for Treatment of Melasma in Asian Patients: A Preliminary ClinicalTrial. Dermatol Surg 2006;32(5):626-31.
14. Maeda K, Tomita Y. Mechanism of the inhibitory effect of tranexamic acido n melanogenesis in cultured human melanocytes in the presence of keratinocyte-conditionedmédium. J Health Sci. 2007;53(4):389-96.
15. Wu S, Shi H, Wu H, Yan S, Guo J, Sun Y, et al. Treatment of melasma with oral administration of tranexamic acid. Aesthetic Plast Surg. 2012;36(4):964-70.
16. Na JI, Choi SY, Yang SH, Choi HR, Kang HY, Park KC. Effect of tranexamic acid on melasma: a clinical trial with histological evaluation. J Eur Acad DermatolVenereol 2013;27(8):1035-9.
17. Aamir S, Naseem R. Oral tranexamic acid in treatment of melasma in Pakistani population: a pilot study. J Pakistan Assoc Dermatol 2014;24(3):198-203.
18. Bagherani N, Smoller BR. Efficacy of topical tranexamic acid in the treatment of melasma. DermatolTher. 2016;29(6):389-90.
19. Ayuthaya PKN, Niumphradit N, Manosroi A, Nakakes A. Topical 5% tranexamic acid for the treatment of melasma in Asians: A double-blind randomized controlled clinical trial. J Cosmetic Laser Ther. 2012;14(3):150-4.
20. Budamakuntla L, Loganathan E, Suresh DH, Shanmugams S, Suryanarayan S, Dongare A, et al. Microinjections and mecroneedling in patients with melasma. J Cutan Aesthet Surg. 2013;6(3):139-43.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}