


Luciana Pereira Paes G. Saraiva; Mayara Brito do Nascimento; Alexandre de Almeida Filippo; Paula Regazzi de Gusmão
Received on: 30/10/2018
Approved on: 16/11/2018
This study was performed at the Instituto de Dermatologia Professor Rubem David Azulay, Santa Casa de Misericórdia do Rio de Janeiro, Rio de Janeiro (RJ), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Scars are very prevalent in the world’s population and can have a significant psychological impact in the patient’s life. There are already conventional clinical and surgical methods for their treatment. However, recurrence and existing side effects drive the search for new therapeutic modalities.
OBJECTIVE: To evaluate the clinical improvement of patients with hypertrophic scarring treated with fractional ablative laser associated to triamcinolone drug delivery.
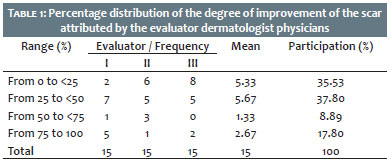
MATERIAL AND METHODS: Eighteen patients with scars to be treated were selected during eight weeks, with four fortnightly sessions of fractional ablative laser associated to 20mg/ml triamcinolone drug delivery. Before and after the treatment, the group was evaluated by three examiners, through the photographic evolution , considering the parameters appearance, dyschromia and degree of hypertrophy. Results: Fifteen patients completed the study. Of these, 35.53% had no or little improvement; 37.80%, moderate to intermediate improvement; 8.89%, expressive improvement and 17.80%, improvement near resolution.
CONCLUSIONS: The proposed association is a promising therapeutic option for the treatment of hypertrophic scars because it is quick to perform and to heal, with less side effects and better tolerated by the patient when compared to the therapies used alone, besides being easily replicable in the office.
Keywords: Cicatrix, hypertrophic; Lasers; Triamcinolone acetonide
Due to its extent and permanent contact with the externai environment, the skin is the human organ that is most often subject to impacts from external factors and resulting injury, healing without the complete reestablishment of its original architecture. Following each surgical intervention, trauma or burn, the process of skin restoration gives rise to the emergence of scars that, which although not completely restoring the normal structure of healthy skin, protect the body against infection and excessive water loss. Hypertrophic scars are characterized by their onset shortly after a trauma of the skin, for not surpassing the contours of the lesion and preferably arising in the articular zones — probably due to the constant pressures to which these regions are subject to.1
Sometimes scars can have a severe impact on the patients’ quality of life, leading to social and professional isolation, and interruption of daily activities. Occasionally, even physical rehabilitation is necessary due to contractures in the joints and function loss.
Hypertrophic scars are firm in consistency, and red, white or pink in color, being characterized by an increase in the expression of collagen. These scars develop as a result of excessive collagen synthesis associated with limited collagen lysis during the matrix remodeling phase. The result is the formation of thick and hyalinized collagen bundles, consisting of fibroblasts and fibrocytes. Unlike keloid scars, which may form weeks or years after the injury has been inflicted, hypertrophic scars usually form in the first month after the initial injury has been inflicted and may recede over time. 2 Several factors have been associated with the emergence of hypertrophic scars: skin color, with higher frequency of high phototypes; female gender; young age, being prevalent in the second decade of life; body sites that underwent of the trauma, with more common appearance in the cervical region and upper limbs.2
There are a variety of therapeutic options available for the treatment of hypertrophic scars, including surgical excision and non-surgical treatment.
Among non-surgical methods, are compressive treatments, silicone gel, cryosurgery, topical and intralesional steroids, beta-therapy and the use of lasers.
Penetration of drugs through untouched stratum corneum occurs by diffusion and, to a lesser extent, through the cutaneous adnexa. It can be performed by transcellular or intra-cellular route.3
Only lipophilic molecules below 500Da can penetrate the untouched stratum corneum. In addition, only 1% to 5% of the medicine applied to the skin is absorbed and becomes bio-available to exert its therapeutic effect.3
The technique termed drug delivery consists of finding methods to optimize cutaneous drug penetration, which can be achieved using chemical, mechanical and physical processes.3
The use of lasers for drug delivery was introduced as a new therapeutic method after Anderson described the concept of fractional photothermolysis in 2004. This method maintains areas with untouched skin between the areas of thermal damage caused by ablative fractional laser (called microthermal zones - MTZ),4 which allow the delivery of drugs in a even and controlled manner.
Lasers promote drug delivery in three ways:
1. Tissue ablation, which removes the stratum corneum and the more superficial layers of the epidermis; 2. Photomechanical waves, resulting from the conversion of light energy into mechanical energy; and 3. Non-ablative resurfacing, in which thermal and physical injuries cause ruptures in the skin barrier, promoting the delivery of medication.5
The main ablative fractional lasers are 2,940nm Er:YAG and 10,600nm CO2 laser, which operate in the infrared range and have water as their target chromophore. 2,940nm Er:YAG laser is absorbed by the epidermis’ water, allowing a more superficial penetration, with less production of heat. 10,600nm CO2 laser penetrates deeper and produces greater heat. Both lasers facilitate drug delivery through microthermal zones (MTZ) and the thermal effect on adjacent tissue.6 Ablative fractional lasers have the specific characteristic of acting by creating tissular ablation columns surrounded by coagulation tissue, that can be modulated according to the type and energy of the laser used. These columns act as canals, providing active principles with access to the lower layers of the epidermis, facilitating drug delivery.7 Microthermal zones can be manipulated by two parameters: density (i.e. the amount of micropores per given area) and depth (controlled by the fluence parameter). The wave type and pulse duration parameters of ablative fractional lasers allow modulating the degree of ablation and the thickness of the coagulation column adjacent to the MTZs. When the coagulation columns are too thick, they hamper the diffusion of the drug.8 In addition, the use of very high energy levels causes deeper lesions that may reach vessels, meaning that the active principle can enter the bloodstream — an undesired effect for drugs that should act only on the skin.
Currently, there are conventional clinical and surgical methods for the treatment of hypertrophic scars, however the use of laser is minimally invasive and very effective, contributing to the therapeutic armamentarium aimed at treating the disorder in question. That is especially true in cases of therapeutic failures and surgical limitations, avoiding the patients’ necessity to suspend their daily activities. In light of this, the authors of the present article will evaluate the viability and effectiveness of ablative fractional laser therapy combined with high-dose corticosteroid drug delivery. Potential benefits include the introduction of a simple and cost-effective strategy for combining two well-established therapies to treat hypertrophic scars, possibly creating a synergistic therapeutic response.
An open, prospective interventional study was carried out in which 18 volunteer patients had their hypertrophic scars (located at any location of the body) treated at the Laser Sector of the Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia de Rio de Janeiro. The patients were selected based on referrals of specialists from the Cosmetology and General Dermatology Sector, as well as from the institutes Laser Sector. The study was approved by the Research Ethics Committee (90998618600005239).
The inclusion criteria were: both genders; all races; older than 18 years; clinical diagnosis of hypertrophic scar at any body site; scars with more than six months of development; no use of other medications for the treatment of scarring during the proposed treatment.
The exclusion criteria were: pregnancy or lactancy; allergy to topical anesthetics; current use of oral isotretinoin; previous personal history of hypersensitivity to the study’s medication; active tuberculosis; herpetic keratitis; recent exposure to the sunlight; previous use of photosensitizing medications; active dermatological lesion in the region to be treated and / or suspicion of malignancy. Patients with keloid scar were not included.
Patients underwent photographic documentation prior to and four weeks after completion of the ablative fractional laser protocol with triamcinolone drug delivery. The procedure was carried out under prior topical anesthesia with 4% lidocaine for at least 30 minutes before the session. Etherea Platforms ablative fractional laser was applied with 2,940nm tip, 12.5mj 300ms (Vydence, Anvisa 80058580015), with subsequent application of drops of 20mg / ml of triamcinolone, enough to cover the entire scar. The contact was maintained for six hours. A total of four sessions were carried out, with 15-day intervals.
An objective clinical evaluation was performed by three “blind / hidden” evaluator dermatologists not related to the institutions laser sector, who examined the photographs taken chronologically, using a scale graded with quartiles: Grade 1 (<25% = minimum improvement / absence of improvement); Grade 2 (26-50% = (moderate-intermediate improvement); Grade 3 (51-75% = important / marked improvement); Grade 4 (> 75% = improvement close to resolution). This analysis was performed for three parameters: appearance, dyschromia and degree of hypertrophy.
Eighteen patients with hypertrophic scars were selected for the study; 3 of them lost continuity, meaning that 15 scars completed the treatment, with all patients being females, with a mean age of38.93 years, and mean duration of scar development of 2.67 years.
Regarding the location of the scars, 26.67% were located in the trunk; 26.67%, in the abdomen; 20% in the limbs; 13.33% in the face; and 13.33% in the ears.
Regarding their etiology, 73.33% of the scars resulted from surgical procedures, while 26.67% were traumatic. Table 1 shows the distribution of results and participation percentages verified in the photographic analysis performed by the blind evaluators (I, II and III) on the 15 scars.
According to the evaluators’ analysis, the patient in Figure 1 had the most expressive improvement in the overall appearance parameter of the scar.
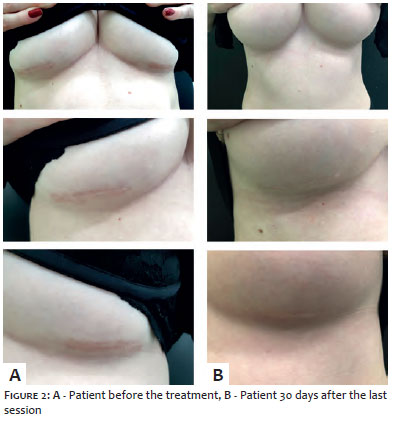
It is important to note that there was no need to complete the four sessions proposed by the protocol in 2 of the patients, given that after the third session, the scars were no longer hypertrophic and only showed a slight difference in texture as compared to the normal skin. One of these patients can be observed in Figure 2.
The patient in Figure 3 presented the best outcome regarding the degree of hypertrophy based on the evaluation of the photographs.
Most patients observed mild to moderate erythema and edema immediately after and within five days following the treatment.
Pain during the session was extremely tolerable, with not all patients needing prior topical anesthetic. There was no report of side effects. No patient experienced worsening of the lesion after the sessions. No recurrence was observed within a three-month follow-up period.
In their clinical practice, dermatologist physicians know that the treatment of cutaneous scars can be complex and often require a multimodal therapeutic approach. Yet, the patient can still remain dissatisfied. These techniques include the application of intralesional corticoid, topical retinoids, surgical excision, cryosurgery, radiotherapy, intralesional 5-fluorouracil, intralesional interferon, occlusion and use of silicone gel. Many of these therapies are painful, ineffective and with some side effects, including atrophy and dyschromia.
For some time, surgical excision associated with corticosteroid intralesional injection has been the treatment of choice. It is known that when surgical excision is performed in isolation, there is a high rate of recurrence (roughly 45% to 100%); nevertheless, when used in combination with corticosteroids, this rate falls to less than 50%.9
Intralesional corticosteroids have been one of the pillars in the treatment of hypertrophic scars for decades, leading to improvements via a variety of mechanisms, including decreased collagen synthesis and increased collagen degeneration. None-theless, injections of triamcinolone acetonide are often painful, and the therapeutic dose difficult to achieve throughout the scar. It is known to have a response of 50% to 100% and recurrence rates of 9% to 50%.9 In many cases, the consequences of applications in the incorrect plane leads to adverse effects, such as dyschromia and atrophy, which become more evident than the scar itself. In light of this, the authors of the present study observed that the application of triamcinolone acetonide following fractional resurfacing is painless, more uniform and reaches the correct plane as a result of the preprogramming of the laser’s parameters.
During the last decade, the advent of fractional laser technology has significantly increased potential treatment options for patients with disfiguring, disabling or only cosmetically scarring scars. Scientific studies demonstrate excellent and safe clinical results, even using lasers isolatedly.10,11,12
The use of these ablative lasers in their fractional mode represents a promising tool in the treatment of scars, with minimal pain and rapid healing, with the possibility of being concluded in a few days. In addition to the specific action of these lasers in scar remodeling, the canals they create in the lesion can be used to deliver active agents within the scar, thus enhancing their effectiveness.13
The use of ablative fractional laser technology aimed at creating pre-established depth canals in the cutaneous tissue, which can reach the target layer and thus be used to administer drugs and other bioactive agents, is undoubtedly the future of the technology, and can be applied both for aesthetic and therapeutic purposes. Optimizing results and reducing side effects will always be the main pursuit of treatments and current ablative fractional laser devices offer a significant benefit for being adjustable, thus allowing the creation of canals with predetermined depth and density.
In the present series of cases, the authors used low enrgies and low densities with the purpose of performing drug delivery (2,940nm Etherea, 12.5mj 300ms).
Previous histological studies on normal skin verified completion of re-epithelization 48 hours after ablative treatment with fractional CO2 laser.14 The authors of the present study then adopted a standard time of six hours for the cleansing of the scar region after the procedure. Their preference was to apply triamcinolone within two minutes of the fractional treatment with a view to allow them to act in the early stages of the inflammatory cascade.
The results of the present case series indicate that the association between laser technology and triamcinolone acetonide drug delivery is an efficient, safe and effective treatment for hypertrophic skin scars. Several important aspects of the evaluation of the scars, such as texture, hypertrophy and dyschromia, were all positively impacted by the combination therapy. The application of corticosteroids following the laser takes advantage of the newly formed canals to penetrate evenly and deeply into the scars.
This is the first Brazilian case series in the literature that evaluates the efficacy of this association in the treatment of hy-pertrophic scars.
The first report was published in the United States by Weibel et al.15 in 2013, with the evaluation of 15 scars and encouraging results, which motivated the its reproduction by the authors of the present study. Although the outcomes of the present case series are promising, there were limitations that must be considered. The authors of the present study used a standard dose of corticoid, without considering the area to be treated. Due to the short follow-up period after the end of the treatment, it was neither possible to evaluate the rate of recurrence nor a more evident clinical improvement resulting from the collagen stimulus. In addition, the lack of a control group made it impossible to assign the better results to the combined treatment as compared to the individual treatments. However, the results of the present series compare favorably with the authors’ experience, both in the speed and in the degree of improvement of the isolated modalities. Additional investigations, including controlled prospective studies, will certainly be required to determine whether the association of ablative fractional laser and topical corticosteroid therapy is more effective as compared to the isolated modalities, and to determine other variables, such as laser parameters and drug dosage.
The results found in the present case series and the great patient satisfaction make it clear that ablative fractional lasers can be an effective tool to optimize and standardize the delivery of triamcinolone acetonide in the treatment of hypertrophic scars.
Undoubtedly, this is a promising therapeutic option for the treatment of hypertrophic scars based on the facts that it can be performed rapidly, it demands a short time for the healing of the tissue, it yields better outcomes when compared to the isolated therapies, it has fewer side effects, it is more tolerable for the patient, and can be easily reproduced in medical practices.
Luciana Pereira Paes Gomes Saraiva | ORCID 0000-0003-1138-6255
Study design and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the literature; critical review of the manuscript.
Mayara Brito do Nascimento | ORCID 0000-0001-7991-1058
Study design and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the literature; critical review of the manuscript.
Alexandre de Almeida Filippo | ORCID 0000-0001-9550-5156
Approval of the final version of the manuscript; study design and planning; effective participation in the research guidance; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the manuscript.
Paula Regazzi de Gusmão | ORCID 0000-0002-7060-6062
Approval of the final version of the manuscript; study design and planning; effective participation in the research guidance; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the manuscript.
1. Wolfram D, Tzankov A, Pulzl P, Piza-Katzer H. Hypertrophic scars and keloids: a review of their pathophysiology, risk factors, and therapeutic management. Dermatol Surg. 2009;35(2):171-81.
2. Mahdavian Delavary B, Vander Veer WM, Ferreira JA, Niessen FB. Formation of hypertrophic scars: evolution and susceptibility. J Plast Surg Hand Surg. 2012;46(2):95-101.
3. Leite-Silva VR, Almeida MM, Fradin A, Grice JE, Roberts MS. Delivery of drugs applied topically to the skin. Expert Rev Dermatol. 2012;7(4):383-97.
4. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional Photothermolysis:A New Concept for Cutaneous Remodeling Using Microscopic Patterns of Thermal Injury. Lasers Surg Med. 2004;34(5):426-38.
5. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicinein the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
6. Sklar LR, Burnett CT, Waibel JS, Moy RL, Ozog DM. Laser assisted drug delivery: a review of an evolving technology. Lasers Surg Med. 2014;46(4):249-62.
7. Kalil C, Campos V, Reinehr CPH, Chaves CRP. Drug delivery assistido por lasers: revisão. Surg Cosmet Dermatol. 2016;8(3):193-203.
8. Haedersdal M, Sakamoto FH, Farinelli WA, Doukas AG, Tam J, Anderson RR. Fractional CO2 laser-assisted drug delivery. Lasers Surg Med.2010;42(2):113-22.
9. Khatri KA, Mahoney DL, Mccaartney MJ. Laser scar revision: A review. J Cosmet Laser Ther. 2011;13(2):54-62.
10. Kwon SD, Kye YC. Treatment of scars with a pulsed Er:Yag laser. J Cutan Laser Ther. 2000;2(1):27-31.
11. Sawcer D, Lee HR, Lowe NJ. Lasers and adjuntive treatment for facial scars: A review. J Cutan Laser Ther. 1999;1(2):77-85.
12. Bouzari N, Davi SC, Nouri K. Laser treatment of keloids and hypertrophic scars. Int J Dermatol. 2007;46(1):80-8.
13. Cavalie M, Sillard L, Montaudie H, Bahadoran P, Lacour JP, Passeron T. Treatment of keloids with laser-assisted topical steroid delivery: a retrospective study of 23 cases. Dermatol Ther. 2015;28(2):74-8.
14. Hantash B, Bedi VP, Kapadia B, Rahman Z, Jiang K, Tanner H, et al. In vivo histological evaluation of a novel ablative fractional resurfacing device. Lasers Surg Med. 2007;39(2):96-107.
15. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med 2013: 45: 135-140.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}