


Eliandre Costa Palermo1; Ana Claudia Esposito2
Received on: 10/10/2018
Approved on: 11/12/2018
This study was performed at Eliandre Palermo's dermatological practice, São Paulo (SP), Brazil.
Financial support: None.
Conflict of interests: None.
Scar formation is the natural healing response of the skin to reestablish dermal integrity after an injury. Besides being unsightly, the scars can also be hypertrophic or keloids, which makes treatment challenging and many times unsatisfactory. Ethnicity and site of the lesion have an important role in the formation of scar types, but it is not always possible to predict the final result. The use of topical silicone has been an option for scar management and the target of many publications over the years. It is believed that its early use can prevent the development of abnormal scars and treat existing scars.
Keywords: Scars, prevention & control; Silicone gels; Treatment
In addition to being unsightly, most scars can lead to severe psychosocial distress, especially when they become hypertrophic or develop into keloids resulting from trauma, burns, and infections.
Even scars considered of excellent quality by physicians can be extremely overvalued by some patients who, unfortunately, do not have the correct understanding of the healing process, thus being vulnerable to psychological discomfort and distress. 1 The dissatisfaction becomes even greater if the scar originates from a surgical procedure carried out for cosmetic purposes. A recent survey indicated that 91% of patients who underwent a routine surgical procedure would appreciate any improvement in their scars.2
Several invasive and non-invasive options can be used for the prevention and treatment of these scars. One of them is the use of silicone in topical sheets or gel. The use of silicone aimed at preventing and treat hypertrophic scars saw its onset in the 1980s for the treatment of burn scars, and has become increasingly studied.3 The application of silicon sheets is one of the most common methods, and their efficacy has been proven in several clinicai studies.4 However, they may be more difficult to camouflage or adapt. Silicone gel, which has been introduced more recently, has gained popularity for being of straightforward application on all types of wound surfaces and easy to camouflage.5
To better understand how silicone based products can act on scars; the present study offers a brief summary of the healing process and its phases.
Wound healing consists of a seamless, coordinated cascade of cellular and molecular events that interact to allow the reconstitution of injured cutaneous tissue. It can be divided into three phases: inflammation, proliferation and contraction and maturation, which take several months to complete.6
The first stage of healing (inflammatory phase) initially involves local hemostasis, in which the platelet aggregation process occurs, with fibrin deposition on the lesion and release of granules by platelets, which contain beta transforming growth factor (TGF-β) in addition to platelet-derived growth factor (PDGF), fibroblast derived growth factor (FGF), epidermal growth factor (EGF), prostaglandins and thromboxanes that attract neutrophils to the wound.7-8
Subsequently, more inflammatory cells reach the lesions site, macrophages phagocyte dead tissue and debris; lymphocytes secrete cytokines; and fibroblasts produce collagen starting restoration and reepithelialization of the skin. This first stage lasts between 48 and 72 hours.8
The second stage (proliferation phase) comprises four basic moments: epithelization, angiogenesis, formation of granulation tissue, and deposition of collagen.
This phase begins around the fourth day after the injury has been inflicted and extends approximately up until the end of the second week. After the fibrin clot formed during hemostasis has been replaced with a new granulation tissue, the new tissue that will form the final healing starts to be produced. Angiogenesis is stimulated by tumor necrosis factor alpha (TNF-α) and is characterized by the migration of endothelial cells and the formation of capillaries, critical for a proper healing and that lend a purplish coloration to the newly formed scar. The final part of the proliferative stage is the formation of granulation tissue. Fibroblasts and endothelial cells are this phase’s most important cells. Dermal fibroblasts adjacent to the wound are activated and referred to as myofibroblasts. The most important growth factor for the proliferation and activation of fibroblasts is PDGF. 7-8 Beta transforming growth factor (TGF-β) is then released, stimulating fibroblasts to produce type I collagen and to become myofibroblasts, which promote wound contraction.8
These cells migrate to the granulation tissue where they produce the new collagen, causing the contraction of the dermis, whose remodeling replaces the granulation tissue with a mature collagen matrix to strengthen the repaired tissues site. This process of remodeling involves the formation and maturation of cicatricial tissue, and may take weeks to months to complete.
Type III collagen produced at the beginning is replaced by type I collagen, thus increasing the scars resistance. It is this balance between the formation and destruction of collagen that will provide the scars final outcome, defining the quality (good or poor) of the scar.7-8
Although healing variations occur among different individuals, healing in surgical wounds generally tends to develop rapidly and with good aesthetical appearance when the final scar is aligned with the skin’s tension lines. However, traumas and burns, as well as some surgical cases more commonly can develop into keloids and hypertrophic scars. In susceptible people, keloids can also emerge after minor injuries, including piercing, acne lesions and injections.
Processes that influence healing may be local, physical, general and systemic: such as age, body site, skin type / ethnicity, hormonal changes (e.g. pregnancy), linked to the existence of associated diseases (e.g. diabetes), smoking habits and alcoholism, vitamins, drugs, and nutritional status. High risk populations, such as Asians, Afro-descendants and patients with a history of keloid formation, are more likely to develop scars, especially in high-risk anatomical areas such as the lower third of the face, presternal region, chest area, upper dorsum, ears, neck and deltoid region.9
A scientific paper by Bond et al. was published in 2008 comparing patients with less than 30 years of age and over 55 years of age, having observed a better healing in older people.10
Strategies to minimize the risk of scarring are indicated before, during, and immediately after surgery. In addition to the ideal surgical management, which includes a good technique, ideal positioning of the incision line and good coaptation of the wounds borders in the suture, crucial measures must be taken (i.e. minimizing the risk of hematoma and infection, reducing the tension of the borders of the wound in the post-operative and maintaining the use of appropriate dressings).
The hydration, protection of the initial scar tissue from ultraviolet (UV) radiation, immobilization of the wound, and the use of silicone in gel or sheets have been considered as prophylactic in the control of undesired scars.1
The wound closes in the first 48 hours after infliction of the injury, and normal scars lessen in around three months, however the full process is only complete in six months. The epidermis takes about one to two weeks to regenerate following a fullthickness wound. During this time, therapeutic prevention against scarring will have little effect because elevated collagen levels are important for thorough wound healing.11
After this period, the new, immature stratum corneum allows abnormally high levels of transepidermal water loss. This dehydration of the stratum corneum stimulates the production of cytokines, which signals the fibroblasts to synthesize and release higher levels of collagen, which can increase the volume of the scar.12
Therefore, it is important to regularly monitor the patients to indicate — if necessary — the preventive use of dressings with silicone. Currently, there is a great aesthetic concern with the appearance of any scar, which may lead the patient to question about the use of preventive measures.13
Studies show that scars tend to have a better development under hydration and use of silicone gel already at this stage of the process, which promotes relief for the patient who often complains of sensation of irritation and itching during the healing process. The application of silicone gel immediately after the removal of the suture replicates the occlusion properties of the stratum corneum, normalizing hydration at the scars site and decreasing the signal sent to fibroblasts to produce excess collagen cells.14
Silicone based products in both plaques and tapes, and gel are considered by many authors as the first line in the management of scars and would act both prophylactically (to ensure a better aesthetic result) and as a therapeutic option against hypertrophic or keloid scars.15
As early as in 1983, the silicone tape or sheet was considered an effective treatment for the management of burn scars.3 They must be used on the scar for 12-24 hours a day for three to six months. The sheets can be reused, however need to be washed daily with neutral soap and water to avoid side effects such as skin irritations or infections. It is important to maintain full coaptation with the scar, which may be more difficult in flexor areas.
Silicon gels have been made available more recently and contain long chain silicone polymers, silicon dioxide and volatile components. They have self-drying technology that is activated in four to five minutes.16 They should be applied as a thin layer on the scar, twice a day, forming a transparent film that is flexible and impermeable to water. They should not be used on open wounds.
Treatment should be maintained for as long as there is aesthetic improvement of the scar. In general, a minimum of three months of use is required.16-17
Both the plaque and the gel can be indicated early on for high-risk patients, after the suture stitches have been removed. Studies show that a reduction of up to 86% of the texture, 84% of the color and 68% of the elevation of the scars can be achieved.18-19
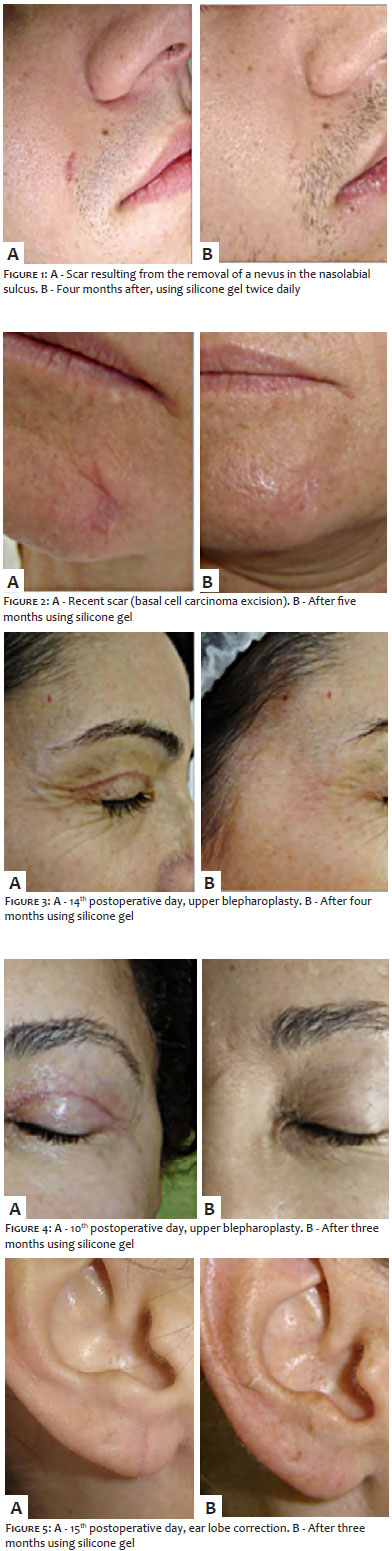
Figures 1 to 5 show excellent esthetic outcomes in surgical scars after the use of silicone gel for a minimum period of three months.
Comparative studies with silicone gels and plaques show equivalence in the treatment and prevention of scars, nevertheless gel products are more straightforward to use.20-21
In addition, gels can be applied to scars with irregular surface, of any size and in moving anatomical regions (like joints). They also do not cause aesthetic compromise as they are transparent and do not need fixation (curative).22 They can be used in children as well as areas with sensitive skin, such as the eyelid region.17 Also, they provide local cooling sensation, which may relieve the itching sensation typical of the first postoperative month.22
Silicone gel can also be used following cauterizations, ablative or non-ablative lasers, intense pulsed light, chemical peels (superficial, medium or deep), as well as after dermabrasion and aesthetic and oncological surgeries.
The gel version usually causes fewer side effects than sheets. On the other hand, gels need to be applied more than once a day and do not offer compression or occlusion. Local irritation, skin fissure and pruritus might occur, however these are rare events.23
A randomized, double blind clinical trial was carried out involving 50 Asian patients with surgical scars. Silicone gel and a placebo gel were used each on one of the sides of the scar for three months. Silicone gel was associated with a significant reduction in cicatricial pigmentation, vascularity, flexibility, elevation, pain and pruritus scores when compared to the placebo.24
The literature shows that silicone sheets and gels are effective in the treatment and prevention of hypertrophic and keloid scars.25-27
There is evidence pointing to action on the stratum corneum, reducing transepidermal water loss and raising skin surface temperature, which may increase collagenase activity.28 In addition, a negative static electric field between the silicone product and the skin could cause the realignment of collagen, resulting in shrinkage of the scars.13 However, occlusion and hydration of the stratum corneum are currently the most accepted as the main mechanisms responsible for the action of silicone. Hypertrophic and keloid scars are associated with abnormal levels of growth factors and this may be directly related to scar dehydration, which might take in excess of one year to return to normal levels.13, 29
Transepidermal water loss in scars dehydrates keratinocytes, releasing cytokines that activate dermal fibroblasts to increase collagen levels, which increases the scar.
The use of silicone improves the hydration of the stratum corneum due to the fact that it reduces the loss of water; with this, a reduction in the stimulation of the fibroblasts occurs, which in turn controls the production of cytokines that regulate the production of collagen.30
Transforming growth factor beta (TGF-β) promotes the proliferation of fibroblasts in the site of the operative wound and stimulates the production of collagen and elastin, while inhibiting the degradation of the extracellular matrix.31,32 On turn, FGF-β normalizes the synthesis of collagen in an abnormal scar and increases the level of collagenases that degrade excess collagen. Platelet derived growth factor (PDGF), an important factor in the proliferation and activation of fibroblasts, was found to be increased in the 3 to 12 postoperative months in comparative studies of hypertrophic scars and normal scars. Recent scars treated with silicone gel film showed significantly less PDGF than untreated scars.35
According studies, the use of topical silicone improves wound hydration, leading to a decrease in the hyperactivity of the cells related to the healing process, being capable of modulating the expression of TGF-β, PDGF and FGF-β. There is a reduction in the expression of TGF-β1 and PDGF when compared to untreated scars, while there is an increase in FGF-β expression in the dermis of treated lesions.36-38
Unsightly scars are associated with psychosocial distress and lower levels of quality of life. Although results of systematic literature reviews point to the existence of bias in some studies, topical silicone is still the first line treatment both in the prevention of unsightly scars and, in special, in the treatment of keloid and scars, with improvement in the texture, color and elevation of the lesions. Statistically, there appear to be no significant differences between effectiveness of silicone plaques and gels; nevertheless some patients report more comfort and improvement of pruritus with gel.
Eliandre Costa Palermo | ORCID 0000-0002-9320-9967
Study conception and design, literature data analysis and interpretation, drafting and final review of the manuscript.
Ana Claudia Esposito | ORCID 0000-0001-9283-2354 Subject discussion, literature data analysis, drafting of the manuscript
1. Monstrey S, Middelkoop E, Vranckx JJ, Bassetto F, Ziegler UE, Meaume S, et al. Updated scar management practical guidelines: non-invasive and invasive measures. J Plast Reconstr Aesthet Surg. 2014;67(8):1017-25.
2. Young VL, Hutchison J. Insights into patient and clinician concerns about scar appearance: semiquantitative structured surveys. Plast Reconstr Surg. 2009;124(1):256-65.
3. Perkins K, Davey RB, Wallis KA. Silicone gel: a new treatment for burn scars and contractures. Burns Incl Therm Inj. 1983;9(3):201-4.
4. O'Brien L, Jones DJ. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database Syst Rev. 2013;2013(9):CD003826.
5. Ahn ST, Monafo WW, Mustoe TA. Topical silicone gel for the prevention and treatment of hypertrophic scar. Arch Surg. 1991;126(4):499-504.
6. Clark RAF: Wound repair. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia, PA: Saunders/Elsevier; 2005. p.112.
7. Broughton G 2nd, Janis JE, Attinger CE. The basic science of wound hea-ling. Plast Reconstr Surg. 2006;117(7 Suppl):12S-34S.
8. Campos ACL, Borges-Branco A, Groth AK. Wound healing. ABCD Arq Bras Cir Dig. 2007;20(1):51-8.
9. Hsu KC, Luan CW, Tsai YW. Review of Silicone Gel Sheeting and Silicone Gel for the Prevention of Hypertrophic Scars and Keloids. Wounds. 2017;29(5):154-158.
10. Bond JS, Duncan JA, Sattar A, Boanas A, Mason T, O'Kane S, et al. Maturation of the human scar: an observational study. Plast Reconstr Surg. 2008;121(5):1650-8.
11. Bleasdale B, Finnegan S, Murray K, Kelly S, Percival SL. The Use of Silicone Adhesives for Scar Reduction. Adv Wound Care (New Rochelle). 2015;4(7):422-430.
12. Gallant-Behm CL, Mustoe TA. Occlusion regulates epidermal cytokine production and inhibits scar formation. Wound Repair Regen. 2010;18(2):235-44.
13. Meaume S, Le Pillouer-Prost A, Richert B, Roseeuw D, Vadoud J. Management of scars: updated practical guidelines and use of silicones. Eur J Dermatol. 2014;24(4):435-43.
14. Mustoe TA. Evolution of silicone therapy and mechanism of action in scar management. Aesthetic Plast Surg. 2008;32(1):82-92.
15. Middelkoop E, Monstrey S, Téot L, Vranckx J-J, editors. Scar management: practical guidelines. Elsene, Belgium: Maca-Cloetens; 2011.
16. Quinn KJ. Silicone gel in scar treatment. Burns Incl Therm Inj. 1987;13 (Suppl):s33-40.
17. Sawada Y, Sone K. Treatment of scars and keloids with a cream containing silicone oil. Br J Plast Surg. 1990;43(6):683-8.
18. Poston J. The use of silicone gel sheeting in the management of hypertrophic and keloid scars. J Wound Care. 2000;9(1):10-6.
19. Suetake T, Sasai S, Zhen YX,Tagami H. Effects of silicone gel sheet on the stratum corneum hydration. Br J Plast Surg. 2000;53(6):503-7.
20. Chernoff WG, Cramer H, Su-Huang S. The efficacy of topical silicone gel elastomers in the treatment of hypertrophic scars, keloid scars, and post-laser exfoliation erythema. Aesthetic Plast Surg. 2007;31(5):495-500.
21. Karagoz H, Yuksel F, Ulkur E, Evinc R. Comparison of efficacy of silicone gel, silicone gel sheeting, and topical onion extract including heparin and allantoin for the treatment of postburn hypertrophic scars. Burns. 2009;35(8):1097-103.
22. Lin YS, Ting PS, Hsu KC. Does the form of dressings matter? A comparison of the efficacy in the management of postoperative scars between silicone sheets and silicone gel: a randomized controlled trial. Medicine (Baltimore). 2018;97(32):e11767.
23. Nikkonen MM, Pitkanen JM, Al-Qattan MM. Problems associated with the use of silicone gel sheeting for hypertrophic scars in the hot climate of Saudi Arabia. Burns. 2001;27(5):498-501.
24. Chan KY, Lau CL, Adeeb SM, Somasundaram S, Nasir-Zahari M. A randomized, placebo-controlled, double-blind, prospective clinical trial of silicone gel in prevention of hypertrophic scar development in median sternotomy wound. Plast Reconstr Surg. 2005;116(4):1013-20.
25. Puri N, Talwar A. The efficacy of silicone gel for the treatment of hypertrophic scars and keloidis. J Cutan Aesthet Surg. 2009;2(2):104-6.
26. Hoeksema H, De Vos M, Verbelen J, Pirayesh A, Monstrey S. Scar management by means of occlusion and hydration: a comparative study of silicones versus a hydrating gel-cream. Burns. 2013;39(7):1437-48.
27. Nedelec B, Carter A, Forbes L, Hsu SC, McMahon M, Parry I, et al. Practice guidelines for the application of nonsilicone or silicone gels and gel sheets after burn injury. J Burn Care Res. 2015;36(3):345-74.
28. Musgrave MA, Umraw N, Fish JS, Gomez M, Cartotto RC. The effect of silicone gel sheets on perfusion of hypertrophic burn scars. J Burn Care Rehabil. 2002;23(3):208-14.
29. Tandara AA, Kloeters O, Mogford JE, Mustoe TA. Hydrated keratinocytes reduce collagen synthesis by fibroblasts via paracrine mechanisms. Wound Repair Regen. 2007;15(4):497-504.
30. Hanasono MM, Lum J, Carroll LA, Mikulec AA, Koch RJ. The effect of silicone gel on basic fibroblast growth factor levels in fibroblast cell culture. Arch Facial Plast Surg. 2004;6(2):88-93.
31. Babu M, Diegelmann R, Oliver N. Keloid fibroblasts exhibit an altered response to TGF-beta. J Invest Dermatol. 1992;99(5):650-5.
32. Moulin V. Growth factors in skin wound healing. Eur J Cell Biol. 1995;68(1):1-7.
33. Ferguson MW, Duncan J, Bond J, Bush J, Durani P, So K, et al. Prophylactic administration of avotermin for improvement of skin scarring: three double-blind, placebo-controlled, phase I/II studies. Lancet. 2009;373(9671):1264-74.
34. Niessen FB, Andriessen MP, Schalkwijk J, Visser L, Timens W. Keratinocyte-derived growth factors play a role in the formation of hypertrophic scars. J Pathol. 2001;194(2):207-16.
35. Choi J, Lee EH, Park SW, Chang H. Regulation of Transforming Growth Factor p1, Platelet-Derived Growth Factor, and Basic Fibroblast Growth Factor by Silicone Gel Sheeting in Early-Stage Scarring. Arch Plast Surg. 2015;42(1):20-7.
36. Kuhn MA, Moffit MR, Smith PD, Lyle WG, Ko F, Meltzer DD, et al. Silicone sheeting decreases fibroblast activity and downregulates TGFbeta2 in hypertrophic scar model. Int J Surg Investig. 2001;2(6):467-74.
37. Tredget EE, Shupp JW, Schneider JC Scar Management Following Burn Injury. J Burn Care Res. 2017;38(3):146-7.
38. Hsu KC, Luan CW, Tsai YW. Review of Silicone Gel Sheeting and Silicone Gel for the Prevention of Hypertrophic Scars and Keloids. Wounds. 2017;29(5):154-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}