


Cintia Santos Braghiroli; Luciana Archetti Conrado
Received on: 01/10/2018
Approved on: 08/12/2018
This study was performed at Clínica Integra Dermatologia, São Paulo (SP), Brazil
Financial support: None
Conflict of interests: None
Microneedling or Percutaneous Collagen Induction is a minimally invasive dermatological procedure that utilizes needles to create orifices or in the skin. Its aim is to induce collagen formation, neovascularization and production of growth factors. There is increased demand because it is a relatively simple procedure, cost-effective, safe and that yields satisfactory results. It treats localized areas and studies are being done to evaluate its role in inflammation, dyspigmentation, and photodamage. The therapeutic use includes the treatment of acne scars, stretch marks, wrinkles, melasma, hyperhidrosis, alopecia. Lately, it has been used for the transepidermal distribution of active compounds and vaccines.
Keywords: Acne vulgaris; Alopecia; Collagen rejuvenation; Dermatologic surgical procedures; Percutaneous collagen induction; Treatment outcome; Wound healing
Microneedling (MN), also known as Percutaneous Collagen Induction Therapy (PCIT), involves performing repeated punctures on the skin using sterilized microneedles.1,2 Its original conception dates from 1995, when Orentreich et al. developed the concept of subincision with the use of hypodermic needles for the breaking of fibrotic bands in the treatment of depressed scars.3 Three years later, Camirand and Doucet reported significant improvement in the clinical appearance and texture of surgical scars through dermabrasion with needles by using a tattoo machine.4 In 2000, the first MN device was used to treat facial rhytids and cutaneous flaccidity. In 2006, Desmond Fernandes developed the first MN device called Dermaroller® 5 (Environ, South Africa).
The studies in this review were selected by searching on PubMed database. The following key words were used on the search: microneedling, review, percutaneous collagen induction therapy, microagulhamento. Articles published in English and Portuguese were included in the review. In vivo studies were considered, and priority was given to controlled, prospective and retrospective clinical studies as well as review articles.
There is a wide variety of cylindrical mechanical devices available, what differentiates them are the length, amount, diameter and material of the needles. They act by rolling perpendicularly over the skin’s surface up until the emergence of superficial bleeding.1,3
The standard MN device, Dermaroller®, has 192 needles that are 2mm long and 0.07mm in diameter, and when applied 15 times on the skin inflicts approximately 250 punctures per cm2 towards the papillary dermis depending on the applied pressure, without causing injury to the epidermis.6,7
- Dermaroller® for home use: it has needles measuring less than 0.15mm in length and are used to reduce pore size, fine lines and sebum production. They can be used from two to three times per week.
- Derma-stamp: miniature version of the Dermaroller. Application is carried out pressuring the device against the skin. It is available in different sizes and its needles measure 0.2 to 3 mm in length. Used for treatment of localized scars, such as those of varicella.
- Dermapen®: pen-like instrument with needle adjustment capability. Used for mechanical resurfacing, with disposable needles.
- DermaFrac®: A technique that combines MN with microdermabrasion, LED therapy and infusion of active ingredients.
- Delivery systems with microneedles: minimally invasive and painless method of transepidermal drug administration, used for vaccines.
- Fractional radiofrequency: needles that penetrate the skin and release — or not — electric current, producing thermal damage to the epidermis or dermis and consequent neocollagenesis.
Micropunctures caused by MN result in controlled mechanical trauma and stimulate the production of collagen by activation of the post inflammatory cascade and release of growth factors, without causing damage to the epidermis. With the recruitment of neutrophils and platelets, the normal cascade of repair and healing begins with the release of growth factors such as TGF-α,TGF-β, as well as platelet derivatives (PDGF), resulting in fibroblast deposition of collagen.2,10
In a study conducted by Lima et al. (2013),11 whose objective was to establish the correlation between needle length and damage depth, a classification based on the histological analysis of fragments of pig skin was proposed:
- Mild injury (0.5mm long needles): mainly used for transepidermal drug delivery (DD) and fine wrinkles (RHYT-IDS);
- Moderate injury (1 and 1.5mm long needles): used for medium-sized wrinkles (RHYTIDS);
- Deep injury (2 and 2.5mm long needles): used for depressed scars and stretch marks.11
There are three phases in the healing process that, predictably, follow the sequence described by Falabella and Falan-ga:12
1. Release of connective tissue growth factors, TGF-beta, PDGF, and connective tissue activating protein, by platelets and neutrophils. These factors increase the production of intracellular matrix.
2. Monocytes also release growth factors that increase the production of collagen, elastin and glycosaminoglycan (GAGs). After five days, fibronectin matrix formation occurs, with aligned fibroblasts, which determines the deposition of collagen.
3. Increased expression of the gene(s) and protein(s) linked to the production of collagen, glycosaminoglycans and growth factors (endothelial and epidermal fibroblasts), crucial for improving clinical aspects of aging. It is possible to observe a quantitative and qualitative increase of the collagen fibers in the papillary and reticular dermis that are distributed in interlaced pattern — which is diverse from the parallel pattern found in cicatricial tissues. Neovascularization and neocollagenesis result in improvement of the scars and their appearance.
Studies show that fibronectin matrix formation occurs within five days, followed by the deposition of type III collagen, which persists for a period ranging from five to seven years.1 Six months after four MN sessions with 30-day intervals, there was a 400% increase in collagen and elastin deposition, with increased thickness of the spinous layer.6,13
Microneedling (MN) combined with Drug Delivery (DD) is a method for administering substances by transepidermal route in which each needle penetrates the skin, with the ensuing application of topical active ingredients.2,14
Promising results have been shown in the treatment of atrophic scars, alopecia, actinic keratoses and pigmentation disorders such as melasma.14 Evidence of efficacy in the treatment of vitiligo remains limited.
Among the numerous studies, stands out the one by Aust et al. (2008), which showed a 140% increase in the thickness of the epidermis after eight weeks with the use of MN followed by the application of a product containing vitamins A and C.1,13 When compared to the use of the isolated antioxidant, the increase in thickness of the epidermis was of 22%.
Bal et al. (2008) used laser scanning microscopy to analyze the dynamics of passive absorption of fluorescein in the depth of microchannels created after MN. The absorption peak of the substance occurred after five minutes, declining within the following ten minutes, and returning to baseline after 15 minutes.15,16
The study carried out by Gordon et al. showed that the time interval of 5 to 30 minutes seems to be the best to apply and massage substances or platelet rich plasma (PRP) into the microchannels created by MN.17 These findings have influence on the time and maximum absorption that the topical agent will exert if applied immediately after MN.
The use of Laser Assisted Drug Delivery (LADD) was first described in 1987, with ablative lasers.18,19 The fractional ablative laser (FAL) produces small ablation channels, with density of the channels and the depth of the microscopic ablation zones (MAZ) serving as the main control parameters.20,21 Density corresponds to the area of surface that underwent ablation, and is determined by the laser device tip’s diameter (spot size) and the number of channels inflicted per unit of skin. The depth of the channels is controlled by the lasers fluence (pulse energy) and corresponds to the extent of the MAZ.20,21 Modifications in the parameters can influence the amount and biodistribution of the active substance, thus favoring the increase of the clinical efficacy and treatment objectives.18
Haedersdal et al. evaluated 16 preclinical studies and evidenced an increase in the absorption of substances after treatment with FAL.18 In the literature, the use of aminolevulinic acid (ALA) for the treatment of actinic keratoses seems to offer the best level of evidence.22 Although no adverse effects have been observed in these studies, DD following FAL carries the risk of systemic absorption of the drugs, in special when performed in large areas.
Microneedling leads to a significant improvement in scarring, stretch marks and rhytids, with a short recovery period and limited adverse effects.6 The clinical results obtained are a consequence of the stimulation of the tissular repair cascade, with an increase in collagen production.2 A number ofpublished studies have demonstrated the histological changes induced by this treatment and its clinical effectiveness. Its best indications include acne scars, periorbital and perioral rhytids, sagging, hypertrophic scars, melasma and alopecias.1
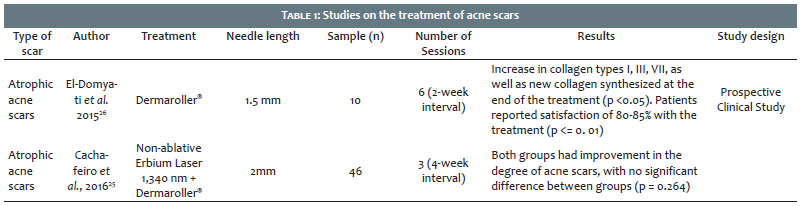
Histological changes resulting from the use of MN for the treatment of acne scars were studied by El-Domyati et al. (2018) in 10 patients with atrophic acne scars on the face using before and after biopsies.23 They showed a significant increase in the production of collagens type I, III and VII, as well as a decrease of elastin at the end of the treatment (p <0.05). Patients reported pain of moderate intensity and edema that subsided within 24 hours, with absence of other adverse symptoms.2,23 Patients also reported improvements in scar appearance (51-60% of patients) and skin texture (40-50%) 90 days (six sessions) after, describing satisfaction with the procedure (80-85%).7 Box-type scars showed improvement (50-70%) after three to five sessions at intervals of two to four weeks. Likewise, stretch marks, atrophic scars and contractures due to burns also showed good results with MN (Table 1).1,23
Although still with few and inconclusive studies, the use of plateletrich plasma (PRP) associated with MN for acne scars has been described. It is believed that activated platelets, applied after the procedure, stimulate the release of growth factors such as VEGF, PDGF and IGF. Promising results with this association were observed in a study by El-Domyati et al. in 2018, when compared to the treatment of acne scars with MN isolatedly (p = 0.015).23 Fabrocini et al. (2011) proposed that PRP could improve the response to wound healing due to the presence of autologous growth factors.24 These authors demonstrated that their use in association with MN was more effective than that of isolated MN.
Some studies compared results between laser and MN. Cachafeiro et al. compared the use of non-ablative erbium laser (1,340nm) with MN in atrophic acne scars.25 Patients (n = 46) were randomized into two groups that received three monthly sessions. Both groups experienced improvement, without significant difference between them.25 Nevertheless, the group treated with laser reported prolonged erythema (averaging three days) and post inflammatory hyperpigmentation (PIH), effects that had not been seen in the MN group, who reported erythema for only one day, with absence of PIH.25
The treatment of hypertrophic scars has been associating MN to DD in deep layers of the skin. A significant improvement of post-burn hypertrophic scars was demonstrated by Aust et al. in patients (n = 16) who used vitamins A and C for 30 days prior to treatment in order to increase collagen production.2,13
The pre-treatment average VAS score (Visual Analog Scale) was 4.5. This scale has values that range from 1 to 10, where 10 corresponds to the highest degree of satisfaction regarding the appearance of the scar. After the treatment with one to four MN sessions followed by topical application of vitamins A and C twice a day yielded an improvement of 3.5 points in the VAS scale, which corresponds to an average VAS score of 8.5. Histological analysis (employing 3mm punches and Van-Gieson’s and Hematoxylineosin Staining) after one year showed a quantitative increase in the deposition of collagen and elastin as well as qualitative improvement of the fibers.
The use of MN for the treatment of facial rhytids has been demonstrated in some studies. Fabbrocini et al. obtained a two-point improvement in the Rhytids Intensity Scale after MN.27 El-Domyati et al. reported a significant increase in type I, III and VII collagen, and tropoelastin levels after six MN sessions.23 Improvement in sagging, resulting in skin tightening caused by MN, possibly occurs due to the reorganization of existing collagen fibers and the simultaneous increase in the production of new structural components of the dermis.23 The increase in dermal collagen and elastic fibers explains the mechanism that leads to the decrease and smoothing of rhytids after the MN.
The treatment consists in the use of a cylindrical device with needles varying in length from 0.5 to 1.5 mm, repeatedly applied over the area to be treated in several directions (vertical, horizontal and diagonal), for approximately 15 to 20 times, producing in average 250 channels per one square centimeter.2,17 The treatment’s goal is to achieve pin-point bleeding or moderate erythema (Table 2).
More recently, the use of MN in the treatment of hair diseases has become frequent, with a number of published studies. Microneedling is believed to stimulate dermal papillae’s stem cells, increase the blood flow to the hair follicles inducing the recruitment of growth factors, and intensify the signaling of pathways that induce hair restoration.3 Studies show that after the procedure, there is release of PDGF, EGF and bulge activation, in addition to increased expression of Wnt3a and Wnt10b,28,29 geneencoding proteins involved in signaling pathways. All these factors stimulate the stem cells of the dermal papilla and induce hair growth.
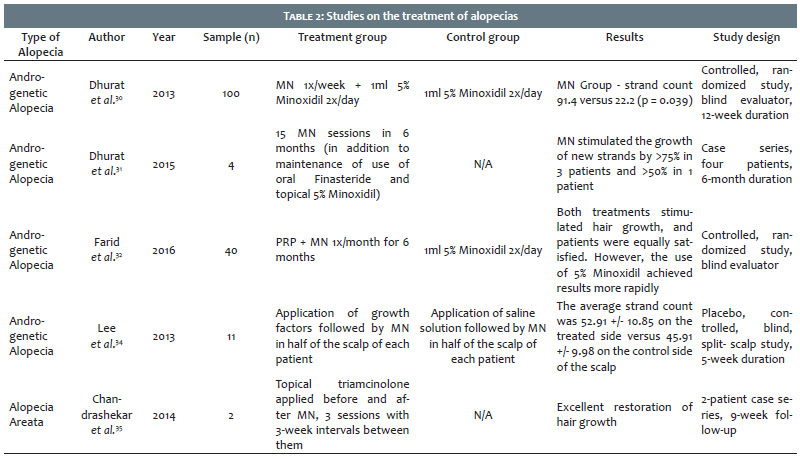
In the first controlled, randomized, clinical trial, in which the evaluator had no information on the groups (blind evaluator) and that was performed in patients with mild to moderate androgenic alopecia (AGA) (n = 100), aged 20-35 years, Dhuran et al. randomly distributed the sample into two groups of 50 individuals.30 One group was treated with weekly MN sessions associated with 5% minoxidil solution twice daily, starting 24 hours after of the procedure, while the other group made use of minoxidil exclusively. Twelve weeks after, the MN group showed a significant increase in strand count (91.4 strands per cm2) as compared to the control group (22.2 strands per cm2) (P = 0.039). There was agreement between evaluator and participants regarding the superiority of the treatment with MN and minoxidil when compared to the control group, a result maintained for eight months after the last MN session. Strand growth was evidenced 6 weeks after the MN procedure, as compared to the 10 weeks in the group where minoxidil was used as the sole treatment.
This same author followed up four male patients with AGA (ages 28, 30, 35, 40) who were resistant to finasteride and Minoxidil. In the six months of treatment, they underwent MN sessions associated with the use of Minoxidil and finasteride, receiving four weekly sessions, followed by two sessions every 15 days (15 sessions in total). The evaluation of results showed that approximately 50% of the patients reported improvement in comparison to the maximum grade of the score system that was used.
The study by Kim et al. of MN in hairless mice resulted in better strand growth as compared to the control group.28,29 There was increase in the regulation of Wnt-3, Beta-catenin, endothelial growth factors, Wnt10b and mRNA, in addition to protein expression. Wnt/p-catenin encourages morphogenesis and hair growth.
Farid et al. (2016) followed up 40 female patients with AGA and comparing the use of MN associated to mesotherapy with PRP and the use of 5% minoxidil as monotherapy. In the first group, the use of PRP in the scalp was aimed at stimulating the release of growth factors such as VEGF, PDGF, IGF, leading to increased vascularization and growth of cells of the dermal papillae, hair follicle and production of new hair strands. After the application of a device with needles of 0.5 mm long up until obtaining moderate erythema, PRP solution (1 ml) was instilled followed by reapplication of the device. The control group used 5% Minoxidil twice daily for six months. Strand growth was observed within 12 to 28 weeks after the beginning of the treatment. Both groups showed increased strand count. The authors concluded that Minoxidil monotherapy was effective and should remain the first treatment option based on improved strand count and faster growth time. These findings led the authors to recommend MN with PRP as the second treatment option in patients with absence of response to topical Minoxidil.33
A pilot study by Lee et al. (2013) evaluated women (n = 11) with a mean age of 41.4, bearing female pattern alopecia (FAGA).34 Half of the scalp was treated with five weekly sessions of topical application of a product (composed of fibroblast, endothelium, insulin-like, keratinocyte, stem cell and superoxide dismutase growth factors) followed by MN with a 0.5mm long needle. The other half of the scalp was used as a control (application of saline solution followed by MN). The half treated with the combination of MN associated and the topical product showed more than a 10% increase in capillary growth starting from the fifth week as compared to the control group.
Chandrashekar et al. (2014) described successful treatments in patients with alopecia areata using MN and topical application of triamcinolone.35 These patients had not responded to previous treatments with triamcinolone injection in the scalp, steroids and topical 5% minoxidil. The topical triamcinolone solution (0.1ml) was applied to the affected areas, followed by MN with 1.5mm long needles and a new application of triamcinolone — three applications with three-week intervals. Patients had improvement in hair strand growth after each session.
Microneedling seems to lead to good results in the whitening of recalcitrant melasma, however the mechanism of action has not yet been clarified.
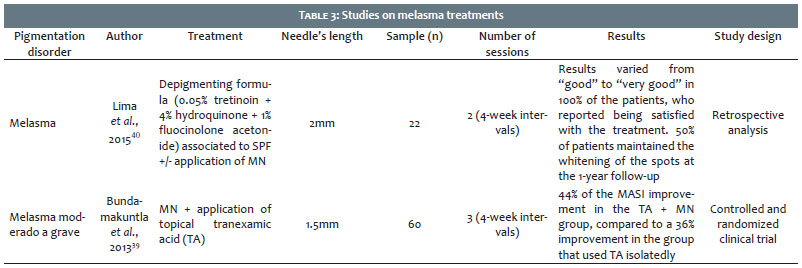
Lima et al. (2017) studied patients bearers of melasma who had undergone two sessions of MN, with 1.5 mm long needles and a 0-day interval between sessions.36 Twenty-four hours after the MN session, there was an application of Kligmans Triple Formula (Triluma®) and broad spectrum sunscreen. There was a perceptible improvement of melasma in all participants and a subjective description of improvement in softness, texture and brightness of the skin, in addition to the maintenance of the results in the sixmonth follow-up. All patients showed increased epithelial thickness, decreased melanin in the epidermis and increased collagen density in the superficial dermis (p = 0.03) (Table 3).
In a previous histological study on the use of the triple combination in melasma, it was not possible to observe thickening of the epidermis or changes in the upper dermis after six months of treatment.36,37 These data corroborate the results described above, indicating that dermal thickening was induced by MN. Furthermore, there was an increase in transepidermal DD for at least 72 hours after the procedure, which can also increase the effect of the triple combination on melanogenesis.38
In addition to the classic treatment (triple combination and broad spectrum sunscreen), MN promoted clinical and histological improvement of recalcitrant facial melasma. Additional randomized and controlled trials are needed to investigate MN treatment schemes in order to maximize their effectiveness and maintain long-term outcomes.36
Regarding the use of whitening agents, MN with DD showed better results than the topical treatment alone. Budamakuntla et al. (2013) observed better results in patients with moderate to severe melasma (n = 60) with the use of MN associated with tranexamic acid as compared to microinjections of tranexamic acid. Patients were observed after three months (three sessions) with a 35% MASI improvement in the microinjection group (p <0.01) compared to 44% in the MN group (p <0.001). Notably, only 26% of the patients who underwent microinjections had a 50% improvement, as compared to 41% in the MN group. None of the two groups reported severe side effects, however some patients reported moderate discomfort, burning sensation, and erythema.
The combination of therapies with MN led to more favorable results in the treatment of melasma when associated with daily use of sunscreen.2
In a retrospective study of patients with recalcitrant melasma (n = 22) who did not respond to whitening and sunscreen, MN was applied followed by a depigmentation formula (0.05% tretinoin + 4% hydroquinone + 1% fluocinolone acetonide), with daily use of SPF 60 sunscreen.40 The procedure was repeated after 30 days. All 22 patients reported satisfactory results after two months of follow-up, with the 24-month photograph follow-up demonstrating maintenance of skin whitening — already observed in the second month of treatment — in 11 patients.40
One study showed good results in the association of MN with topical bleomycin (0.2 -0.5 ml) in the treatment of plantar warts.41 There was good tolerance to pain and absence of reports of tissue necrosis, which is observed when intralesional bleomycin is used.
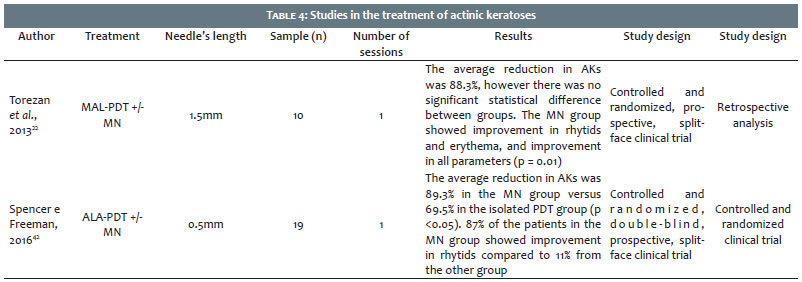
The use of MN in the treatment of field cancerization and actinic keratoses was evaluated by Torezan et al. (2013) in a split-face study (n = 10).22 Microneedling was applied in one of the hemifaces after photodynamic therapy combined with Methylamino levulinate (MAL-PDT) and compared with the use of isolated MAL-PDT in the other hemiface. Methylamino levulinate-PDT combined with MN led to superior results in all parameters studied22 (including facial erythema and photoaging) when compared to the isolated use of MAL-PDT (p = 0.01).
Spencer and Freeman (2016) performed a split-face randomized study (n = 20) in two groups.42 One of the groups used MN followed by the application of delta-aminolevulinic acid (ALA-PDT), and the other group underwent application of ALA-PDT as monotherapy. There was a significant difference (p <0.05) between the groups, with improvement of 89% of actinic keratoses in the ALA-PDT and MN group, as compared to 69% in the monotherapy group.
Contraindications to MN are limited and include inflammatory acne, active labial herpes or another infection in the area being treated, predisposition to keloid formation and immunosuppression. In addition, care must be taken with the concomitant application of MN near the areas of botulinum toxin injection with a view to preventing its undesired diffusion.
Microneedling is deemed as a minimally invasive procedure with few associated adverse effects, with moderate erythema and localized edema that usually resolve within 48 to 72 hours being the most common and expected. Pin-point-type bleeding is limited to the minutes after the procedure, and should be treated with the application of gentle manual pressure and gauze with cold saline solution. Transient erythema is the most common adverse event.
Depigmentation events used to be a worrying complication in higher phototypes. However, it is rarely observed when there is no exposure to the sun after the treatment. In addition, histological analysis of melanocytes 24 hours after MN evidenced absence of changes in the epidermis or in the number of melanocytes, suggesting that the risk of undesirable depigmentation is possibly minimal.
In a series of cases (2014) three patients developed granulomatous reaction caused by the topical use of vitamin C serum after MN.43 Drug delivery (DD) during or immediately after MN should be carried out with caution since the formation of channels in the epidermis and dermis are a gateway for microorganisms to occur and may also increase the incidence of adverse effects, thus enabling the development of an immune response to potentially immunogenic particles. Nonetheless, adverse reactions are rare and systemic toxicity reactions have not been reported. Patients should be instructed not to use products that have not been prescribed by physicians within the first week after MN, as they may potentially induce a local or systemic hypersensitivity reaction. It is recommended that DD associated with MN be performed with caution, as nonsterile substances may contain particles that penetrate the layers of the skin possibly leading to future complications. In addition, the application of topical agents to the skin immediately after MN should be performed with extreme caution aimed at avoiding the above described complications. Further studies are necessary on transepidermal substances and vehicles for DD, aimed at minimizing the risks of unwanted absorption, allergic reactions, infections and others.
In recent years there has been a significant increase in the demand for minimally invasive procedures, which suggests that MN will be of special interest for patients who wish clinical results without a prolonged recovery time. In general, the procedure is efficacious, cost effective, has few adverse effects and stands as a viable option in the rejuvenation of patients with higher phototypes.44 It is generally well tolerated with only the application of topical anesthetics when using needles of up to 1 mm in length. Greater needle lengths demand that the extent of the area to be treated be evaluated, meaning that block and/or infiltration anesthesia are often required.11
Since the introduction of the subincision concept by Orentreich et al., which evolved with the help of Camirand et Doucet and Desmond Fernandez, MN quickly became a dynamic procedure with the use of electrical and manual equipment.1,4,5 Microneedling is safe, minimally invasive and effective in the treatment of many dermatological conditions such as acne, scars, rhytids and stretch marks. With rapid postoperative recovery, limited side effects and significant clinical outcomes, MN is an alternative to more invasive procedures such as laser resurfacing and deep chemical peels.
This review article highlights scientific evidence related to the use of MN in various dermatological conditions. In addition to its cosmetic use (e.g. in pigmentation disorders), it also has excellent indication for the treatment of premalignant lesions (actinic keratoses), acne scars and scalp disorders.
The advantages of this procedure include good patient tolerability, the possibility of increasing transepidermal drug delivery (DD), and practicality and safety of use in higher phototypes.
Further controlled clinical trials are required in order to verify the use of MN as a scientific evidence-based procedure in the treatment of various dermatological diseases, as well as for aesthetic purposes. Moreover, the required number of sessions, the ideal devices, including needle length and depth to be reached, should be better studied. Finally, studies elucidating the details of the mechanism of action of MN, especially in the treatment of alopecia and pigmentation disorders, are required.
Cintia Santos Braghiroli | ORCID 0000-0002-6254-552X
Study conception and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; criticai review of the literature
Luciana Archetti Conrado | ORCID 0000-0002-5934-9720
Approval of the final version of the manuscript; study conception and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; effective participation in research guidance; critical review of the literature, critical review of the manuscript
1. Alster TS, Graham PM. Microneedling: A Review and Practical Guide. Dermatol Surg. 2018;44(3):397-404.
2. Iriarte C, Awosika O, Rengifo-Pardo M, Ehrlich A. Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol. 2017;10:289-298.
3. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543-9.
4. Camirand A, Doucet J. Needle dermabrasion. Aesth Plast Surg. 1997;21(1):48-51.
5. Fernandes D. Percutaneous collagen induction: an alternative to laser resurfacing. Aesth Surg J. 2002;22(3):307-9.
6. Singh A, Yadav S. Microneedling: Advances and widening horizons. Indian Dermatol Online J. 2016;7(4):244-54.
7. Bhardwaj D. Collagen induction therapy with dermaroller. Community Based Med J. 2013;1:35-7.(não pude verificar a existência de numero, o site está fora do ar)
8. Doddaballapur S. Microneedling with dermaroller. J Cutan Aesthet Surg. 2009;2(2):110-1.
9. McCrudden MT, McAlister E, Courtenay AJ, González-Vázquez P, Singh TR, Donnelly RF. Microneedle applications in improving skin appearance. Exp Dermatol. 2015;24(8):561-6.
10. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
11. Lima EVA, Lima MA, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol 2013;5(2):110-4.
12. Falabella AF, Falanga V. Wound healing. In: Freinkel RK, Woodley DT, editors. The Biology of the Skin. New York: Parthenon; 2001. p. 281-99
13. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg. 2008;121(4):1421-9.
14. Bariya SH, Gohel MC, Mehta TA, Sharma OP. Microneedles: an emerging transdermal drug delivery system. J Pharm Pharmacol. 2012;64(1):11-29.
15. Sasaki GH. Micro-Needling Depth Penetration, Presence of Pigment Particles, and Fluorescein-StainedPlatelets: Clinical Usage for Aesthetic Concerns. Aesthet Surg J. 2017;37(1):71-83.
16. Bal SM, Caussin J, Pavel S, Bouwstra JA. In vivo assessment of safety of microneedle arrays in human skin. Eur J Pharm Sci. 2008;35(3):193-202.
17. Strazzulla LC, Avila L, Lo Sicco K, Shapiro J. An Overview of the Biology of Platelet-Rich Plasma and Microneedling as Potential Treatments for Alopecia Areata. J Investig Dermatol Symp Proc. 2018;19(suppl 1):S21-S24.
18. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
19. Jacques SL, McAuliffe DJ, Blank IH, Parrish JA. Controlled removal of human stratum corneum by pulsed laser. J Invest Dermatol. 1987;88(1):88-93.
20. Hantash BM, Bedi VP, Chan KF, Zachary CB. Ex vivo histological characerization of a novel ablative fractional resurfacing device. Lasers Surg Med. 2007;39(2):87-95.
21. Haedersdal M, Sakamoto FH, Farinelli WA, Doukas AG, Tam J, Anderson RR. Fractional CO(2) laser-assisted drug delivery. Lasers Surg Med. 2010;42(2):113-122.
22. Torezan L, Chaves Y, Niwa A, Sanches JA Jr, Festa-Neto C, Szeimies RM. A pilot split-face study comparing conventional methyl aminolevuli-nate-photodynamic therapy (PDT) with microneedling-assisted PDT on actinically damaged skin. Dermatol Surg. 2013;39(8):1197-201.
23. El-Domyati M, Abdel-Wahab H, Hossam A. Microneedling combined with platelet-rich plasma or trichloroacetic acid peeling for manage-mentof acne scarring: A split-face clinical and histologic comparison. J Cosmet Dermatol. 2018;17(1):73-83.
24. Fabbrocini G, Valerio DV, Francesco P, Panariello L, Fardella N, Sepulveres R, et al. Combined use of skin needling and platelet-rich plasma in acne scarring treatment. Cosmet Dermatol. 2011;24(4):177-83.
25. Cachafeiro T, Escobar G, Maldonado G, Cestari T, Corleta O. Comparison of Nonablative Fractional Erbium Laser 1,340 nm and Microneedling for the Treatment of Atrophic Acne Scars: A Randomized Clinical Trial. Dermatol Surg. 2016;42(2):232-41.
26. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Microneedling therapy for atrophic acne scars: an objective evalu- ation. J Clin Aesthet Dermatol. 2015;8(7):36-42.
27. Fabbrocini G, De Vita V, Di Costanzo L, Pastore F, Mauriello MC, Ambra M, et al. Skin needling in the treatment of the aging neck. Skinmed. 2011;9(6):347-51.
28. Kim HM, Lim YY, An JH, Kim MN, Kim BJ. Transdermal drug delivery using disk microneedle rollers in a hairless rat model. Int J Dermatol. 2012;51(7):859-63.
29. Kim YS, Jeong KH, Kim JE, Woo YJ, Kim BJ, Kang H. Repeated microneedle stimulation induces enhanced hair growth in a murine model. Ann Dermatol. 2016;28(5):586-92.
30. Dhurat R, Sukesh MS, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect of microneedling in androgenetic alope- cia: a pilot study. Int J Trichology. 2013;5(1):6-11.
31. Dhurat R, Mathapati S. Response to microneedling treatment in men with androgenetic alopecia who failed to respond to conventional therapy. Indian J Dermatol. 2015;60(3):260-3.
32. Farid CI, Abdelmaksoud RA. Platelet-rich plasma microneedling versus 5% topical minoxidil in the treatment of patterned hair loss. J Egypt Womens Dermatologic Soc. 2016;13:29-36.
33. Fertig RM, Gamret AC, Cervantes J, Tosti A. Microneedling for the treatment of hair loss? J Eur Acad Dermatol Venereol. 2018;32(4):564-9.
34. Lee YB, Eun YS, Lee JH,Cheon MS, Park YG, Cho BK, et al. Effects of topical application of growth factors followed by microneedle therapy in women with female pattern hair loss: a pilot study. J Dermatol. 2013;40(1):81-3.
35. Chandrashekar B, Yepuri V, Mysore V. Alopecia areata-successful outcome with microneedling and triamcinolone acetonide. J Cutan Aes-thet Surg. 2014;7(1):63-4.
36. Lima EVA, Lima MMDA, Paixão MP, Miot HA. Assessment of the effects of skin microneedling as adjuvant therapy for facial melasma: a pilot study. BMC Dermatol. 2017;17(1):14.
37. Bhawan J, Grimes P, Pandya AG, Keady M, Byers HR, Guevara IL, et al. A histological examination for skin atrophy after 6 months of treatment with fluocinolone acetonide 0.01%, hydroquinone 4%, and tretinoin 0.05% cream. Am J Dermatopathol. 2009;31(8):794-8.
38. Lev-Tov H, Larsen L, Zackria R, Chahal H, Eisen DB, Sivamani RK. Microneedle-assisted incubation during aminolaevulinic acid photody-namic therapy of actinic keratoses: a randomized controlled evalua-torblind trial. Br J Dermatol. 2017;176(2):543-5.
39. Budamakuntla L, Loganathan E, Suresh DH, Shanmugam S, Suryanarayan S, Dongare A,et al. A randomised, open-label, comparative study of tranexamic acid microinjections and tranexamic acid with microneedling in patients with melasma. J Cutan Aesthet Surg. 2013;6(3):139-43.
40. Lima EA. Microneedling in facial recalcitrant melasma: report of a series of 22 cases. An Bras Dermatol. 2015;90(6):919-21.
41. Konicke K, Olasz E. Successful treatment of recalcitrant plantar warts with bleomycin and microneedling. Dermatol Surg. 2016;42(8):1007-8.
42. Spencer JM, Freeman SA. Microneedling prior to Levulan PDT for the treatment of actinic keratoses: a split-face, blinded trial. J Drugs Dermatol. 2016;15(9):1072-1074.
43. Soltani-Arabshahi R, Wong JW, Duff KL, Powell DL. Facial allergic granulomatous reaction and systemic hypersensitivity associated with microneedle therapy for skin rejuvenation. JAMA Dermatol. 2014:150(1):68-72.
44. Al Qarqaz F, Al-Yousef A. Skin microneedling for acne scars associated with pigmentation in patients with dark skin. J Cosmet Dermatol. 2018;17(3):390-395.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}