


Larissa Magoga Biselli1; Lara Fileti Arruda1; Maisa Fabri Mazza1; Maria Cristina Jacomette Maldonado1; Domingos Jordão Neto1; Maria Isabel Pereira Soares Takemoto2
Received on: 24/11/2017
Approved on: 24/09/2018
This study was performed at the Complexo Hospitalar Heliópolis - São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Alopecia areata is a chronic condition of hair follicles and nails with unknown etiology, which causes hair loss. It emerges in several clinical types, with the diffuse form, where there is acute and diffuse hair loss, being atypical. It is generally accepted that there is a T-cell mediated, organ-specific autoimmune base in alopecia areata and studies indicate that the autoantigen is associated with melanocytes. The authors of the present paper report the case of a patient who had the diffuse form of alopecia areata, with preservation of the gray hair strands
Keywords: Alopecia Areata; Alopecia; Autoantigens; Hair
Alopecia areata (AA) is a chronic condition of hair follicles and nails, with unknown etiology, possible multifactorial with evident autoimmune and genetic components. It determines hair and / or hair loss by interrupting its synthesis, without destruction or atrophy of the follicles, meaning it can be reversible.1
It can arise under several clinical forms, the diffuse form being an atypical type of AA, in which there is acute and diffuse hair loss, in most cases developing into more severe forms of total or universal AA.1
In addition, it is universally accepted that AA has a T cell-mediated organ-specific autoimmune base. Studies suggest that the autoantigen of AA is associated with melanocytes.2
Aiming at contributing to the study of the autoimmunity theory and the role of melanocytes as autoantigens, the authors of the present paper describe the case of a patient who developed the diffuse form of AA with preservation of gray hairs.
A 74-year-old male patient sought medical care with complaints of rapid graying of his hair, with the condition developing into abrupt and intense fall of black hair after two months. According to the patient, his hair was previously mixed, with a greater number of more dark strands.
He had a personal history of hypertension and benign prostatic hyperplasia, and was in continuous use of hydrochlorothiazide and doxasozine for approximately 20 and 10 years, respectively. He had been using ciprofloxacin and diclofenac sodium for six months due to an uncomplicated urinary tract infection.
The dermatological examination revealed diffuse hair rarefaction predominantly in the parietal region (Figure 1), with an intensely positive traction test for black and negative for gray strands. Eyebrows, eyelashes and hairs on the rest of the body showed no changes and no skin or nail changes were observed.
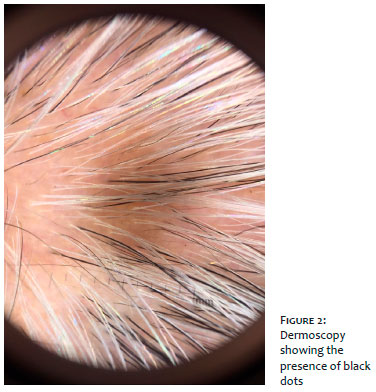
Dermoscopy, an important diagnostic test, revealed black dots and exclamation points in the areas of alopecia (Figure 2).
In light of the medical history, clinical and dermoscopic findings typical of alopecia areata, it was decided not to perform a biopsy, to start the treatment and to carry out a laboratory investigation.
Laboratory tests were within the limits of normality, including: blood count, electrolytes, iron, ferritin, zinc, copper, ANA, VDRL, and renal, hepatic and thyroid functions. Vitamin B12 (166) and vitamin D deficiency was evidenced (13).
Treatment consisted of the use of clobetasol emulsion once daily during the first month, and on alternate days in the second month, 5% minoxidil sulfate once daily, as well as replacement of deficient vitamins (50,000,000 IU of oral cholecalciferol and 5,000mcg vitamin B12 intramuscularly, in weekly doses, for three months).
The patient coursed with the end of hair loss and repilation in three months, with the growth of gray strands, without recurrence during the following six months of follow-up.
Alopecia areata (AA) is a disease that affects men and women, especially young people. It is characterized by the loss of hair in one or several areas of the scalp, and can also compromise the beard, eyebrows and perineum. It clinically arises as circular alopecic plaques without inflammatory signs, and may develop into favorable conditions of spontaneous repilation, or to more severe cases of total alopecia (extensive progression on the scalp) or universal alopecia (whole body surface).3
The approximate prevalence of AA in the world population is 0.1%. Both genders, all ages and ethnic groups can be affected by the disease. The peak incidence of AA takes place between 20 and 25 years of age, although the disease may occur at any time in life. The first episode of the disease may occur before the age of 20 years in approximately 60% of patients.3
It is believed that the pathogenesis of AA is linked to genetic and autoimmune factors, and emotional stress. 3 There is a possible action of the biochemical pathways in the manifestation of this dermatosis, with the influence of emotional phenomena occurring through the action of neuromediators.4 Based on studies, including clinical observations and psychological assessments, the strong influence of anxiety and depression was identified for skin disorders.
Regarding the micronutrient dosage in patients with AA, the literature demonstrates that serum levels of vitamin D, zinc and folic acid tend to be lower in AA patients when compared to controls. There is insufficient evidence to suggest differences in levels of selenium, vitamin B12, copper and magnesium.5
An immune infiltrate surrounding the hair follicles is present in AA, consisting of activated T-helper cells, cytotoxic T cells and natural killer cells, characterizing an inflammatory response of the TH1 type.6 Evidence of immune activation includes the expression of HLA-DR, HLA-A, B, C, and ICAM-1 in the follicular epithelium. The follicular expression of HLA-DR and ICAM-1 is possible under induction by interferon-gamma produced by T cells. Antibodies to the follicular epithelium are often present, however their significance is still unclear. All these factors would contribute to the collapse of the immune privilege of the hair follicle.2
There is a hypothesis that an antigen linked to follicular melanocytes can explain sudden poliosis (Marie Antoinette syndrome).7 Antigens associated with melanocytes are able to activate T cells, inducing hair loss, which suggests that they are capable of acting as autoantigens in AA.2 Studies conducted in rats have shown that these melanocytes can act as epitopes for T cells, causing AA in the animals studied.8 Gilhar et al. have demonstrated that melanocyte-associated T cell epitopes are able to function as autoantigens and result in AA in human scalp grafts. HLA-A2-restricted melanocyte peptides can activate T cells to transfer AA to autologous scalp skin grafts in rats, indicating that melanocyte-associated autoantigens may be pathogenic.8
Yet several studies suggest that peptides associated with melanogenesis, expressed by hair follicles in anagenesis, correspond to autoantigens capable of activating cytotoxic T cells (CD8 +) when immune privilege is lost.9 This theory is well supported by the facts that white or gray hair follicles are spared in AA lesions and that, after alopecia, during the recovery phase, growing hairs are initially depigmented, with repigmentation taking place later on. There is histological evidence that, in patients with AA, follicular melanocytes have structural irregularities.10
The diffuse variant is atypical in AA and causes acute and diffuse hair loss. It may represent the initial form, especially in children and adolescents, or it may occur as a development of variants in which it arises in plaques. In this variant, there is acute and diffuse hair loss, and most cases progress to more severe forms of total or universal AA. Its diagnosis is the most difficult among those of AA subtypes, requiring differential diagnosis with acute telogen effluvium, androgenetic alopecia and syphilitic alopecia. In general, it requires complementary tests and biopsy based histological examination.1
The case reported in the present paper clearly illustrates the theory of autoantigens associated with melanogenesis, since the great hair loss occurred with pigmented strands, a fact that was noticed by the patient in light of its important relevance.
Although the physiopathology has not yet been completely elucidated, the careful observation of the onset and appearance of the clinical picture corroborates the autoimmune and melanocyte autoantigen theories currently valid, which are aimed at clarifying the pathophysiology of AA.
We would like to thank Coloproctologist physician Dr. Paulo Boarini for the referral of the patient to the Dermatology Clinic of the Hospital Heliópolis, and to Dr. Isabel Takemoto for the brilliant diagnosis and follow-up of the case.
Larissa Magoga Biselli | ORCID 000-003-1043-9896
Elaboration and drafting of the manuscript, critical review of the literature, critical revision of the manuscript
Lara Fileti Arruda | ORCID 0000-0002-3176-7840
Elaboration and drafting of the manuscript, critical review of the literature
Maisa Fabri Mazza | ORCID 0000-0002-0513-3078
Elaboration and drafting of the manuscript, critical review of the literature
Maria Cristina Jacomette Maldonado | ORCID 0000-0002-5806-9508
Intellectual participation in propaedeutic and / or therapeutic approach of the cases studied, critical review of the manuscript
Domingos Jordão Neto | ORCID 0000-0001-7752-6789
Critical review of the manuscript
Maria Isabel Pereira Soares Takemoto | ORCID 0000-0002-4343-8702
Approval of the final version of the manuscript, preparation and writing of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied, critical revision of the manuscript
1. Rivitti EA. Alopecia areata: a revision and update. An Bras Dermatol. 2005;80(1):57-68.
2. Kalish RS, Gilhar A. Alopecia areata: autoimmunity - evidence is compelling. J Investig Dermatol Symp Proc. 2003;8(2):164-7.
3. Alzolibani AA. Epidemiologic and genetic characteristics of alopecia areata (part 1). Acta Dermatovenerol Alp Panonica Adriat. 2011;20(4):191-8.
4. Prado RBR, Neme CMB. Experiências afetivo-familiares de mulheres com alopecia areata. Estud Psicol. 2008;25(4):487-97.
5. Thompson JM, Mirza MA, Park MK, Qureshi AA, Cho E. The role of micronutrients in Alopecia Areata: A Review. Am J Clin Dermatol. 2017;18(5):663-79.
6. Petukhova L, Duvic M, Hordinsky M, Norris D, Price V, Shimomura Y, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature 2010;466(7302):113-7.
7. Navarini AA, Nobbe S, Trüeb RM. Marie Antoinette syndrome. Arch Dermatol. 2009;145(6):656.
8. Gilhar A, Landau M, Assy B, Shalaginov R, Serafimovich S, Kalish RS, Melanocyte-associated T cell epitopes can function as autoantigens for transfer of alopecia areata to human scalp explants on Prkdcscid mice. J Invest Dermatol. 2001;117(6):1357-62.
9. Islam N, Leung PS, Huntley AC, Gershwin ME. The autoimmune basis of alopecia areata: a comprehensive review. Autoimmun Rev. 2015;14(2):81-9.
10. Ito T. Recent advances in the pathogenesis of autoimmune hair loss disease Alopecia Areata. Clin Develop Immunol. 2013; 2013:348546.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}