


Caroline de Freitas Barbosa; Tatiana Villas Boas Gabbi
Received on: 11/08/2018
Approved on: 24/09/2018
This study was performed at the Hospital das Clinics, Faculdade de Medicina, Universidade de São Paulo – São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Onychocryptosis is a common condition in adolescents and young adults. Many conservative and clinical treatments have already been described. The authors of the present paper describe the standardization of the onychocryptosis surgical technique using 88% phenol, which is performed at a university hospital’s dermatology outpatient clinic since 2009.
Keywords: Dermatologic surgical procedures; Dermatology; Phenol; Nails, Ingrown; Research and new techniques; Technical aspects
Onychocryptosis mainly affects the hallux in teenagers and young adults, jeopardizing the daily and social activities of patients. Several triggering factors, such as incorrect trimming of the nails, use of inadequate shoes, local trauma and anatomical changes are described.1,2
The disorder can be classified according to three stages: Stage 1) presence of inflammation, edema and local pain; Stage 2) presence of inflammation, pain and formation of granulation tissue; and Stage 3) previous symptoms in addition to the formation of abscess and chronic induration of the nail’s lateral edge.3
In addition to conservative therapies, several surgical treatments were described for the disease, among them: matricectomy, phenolization, resection of soft tissues with matricectomy, and partial matricectomy with cryotherapy.4-8
The authors of the present article will describe the standardized ungual matrix phenolization surgical technique for onychocryptosis carried out at the Dermatologic Ambulatory of the Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo (HC-FMUSP), Brazil.
The onychocryptosis surgical technique was standardized at the HC-FMUSP, and has been carried out since 2009.
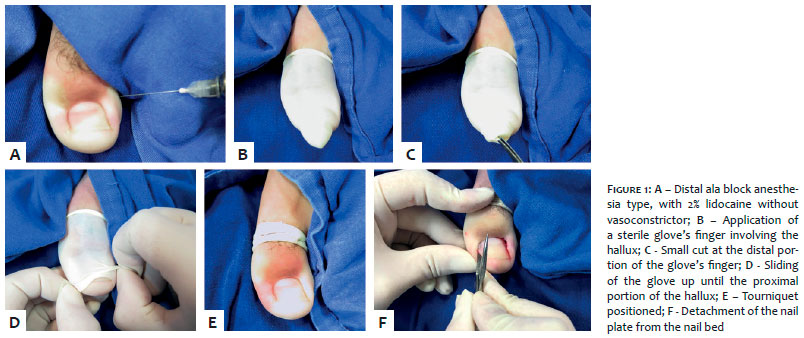
After vigorous asepsis of the region with chlorhexidine, surgical fields are put in place, with subsequent distal block anesthesia with 2% lidocaine, without vasoconstrictor (Figure 1a). Next, the tourniquet is applied to the affected toe (Figure 1b), a sterile glove finger with one small cut in its distal portion (Figure 1c), with the exsanguination of the toe taking place by means of sliding the glove towards its proximal portion (Figures 1d, 1e). The procedure begins with the detachment of the nail plate’s affected region from the respective nail fold, cuticle and nail bed (Figure 1f).
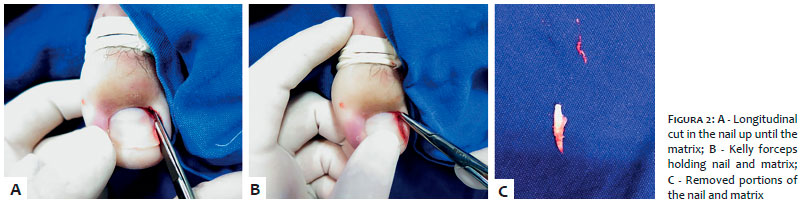
Then, a longitudinal cut of the nail blade is performed with a straight scissors, from the nail’s distal portion up until the matrix (Figure 2a). This fragment is then fastened with a kelly forceps (Figure 2b), with the subsequent removal of nail and matrix with a twisting movement around the longitudinal axis, along the nail’s direction (Figure 2c).
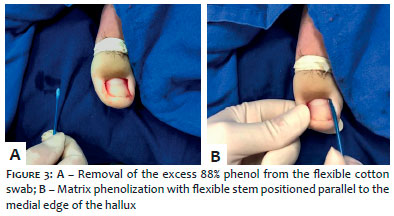
The phenolization procedure is performed with a flexible sterile cotton swab moistened in 88% phenol (Figure 3a). After removing excess phenol, the procedure is carried out in the matrix (Figure 3b) by positioning the flexible swab longitudinally and rotating it during 60 seconds in the nail’s direction.
Lastly, the tourniquet is removed (Figure 4a), and the compressive dressing is applied with gauze and 10cm orthopedic bandage (Figure 4b).
After the procedure, the patients are kept under observation for roughly 30 minutes, with the operated limb elevated, at a higher position than his or her trunk, for later evaluation of local bleeding. Patients are discharged after being instructed on resting requirements, elevation of the limb, and the necessity to keep the dressing clean and closed up until the next day. In this Dermatology Service, a decision was made for antibiotic therapy with 500mg cephalexin every six hours, based on a directive issued by the Hospital Infection Control Commission, in the absence of contraindication. Typically, reasonable pain control is obtained with common analgesics, such as dipyrone.
At the first postoperative return visit (PO), the dressing is removed and the surgical site evaluated. The patient is instructed on how to cleanse the wound, apply local dressing and stimulate the motion of the operated toe.
At the 7th and 14th POs, evaluations of the surgical site and possible complications, such as infection in soft parts and pyogenic granuloma formation, are carried out. Two weeks after the surgical procedure, the patient is released to use closed shoes and is educated on how to trim the nails and use adequate shoes aiming at avoiding recurrences.
At the 30th PO there is an evaluation of the procedure’s final outcome. The patients are followed up at the onychopathies ambulatory each two or three months, for one year.
Pain and bleeding are expected in the immediate postoperative, with improvement from the 1st PO. Patients are instructed and encouraged to perform local cleansing starting from the 1st PO, in order to avoid local secondary infection.
The formation of pyogenic granuloma and infection of soft parts are little common complications at this Service. The majority of patients typically succeed in returning to their daily activities, including the use of closed shoes, two weeks after the procedure. It is at this point that they are instructed on how to correctly trim their nails.
At the 30th PO, the total closure of the wound has already occurred, with significant improvement of the local inflammation and pain, as seen in Figure 5d.
The patients are followed up for one year, for the evaluation of recurrences – which are uncommon.
Onychocryptosis is a disease that jeopardizes the patients’ daily lives, in special those of teenagers and young adults, and can to be triggered by several factors, such as the inappropriate trim of the nails, use of inadequate shoes, local trauma, and anatomical changes. It mainly affects the hallux, as described by the literature and evidenced in the authors’ practical experience.1-3
Several treatments – both conservative and surgical – have already been described. At the HC-FMUSP, the authors of the present article have made a decision for the onychocryptosis surgery with the use of 88% phenol, which was standardized and has been performed at the Institution’s Dermatology Service since 2009, with good results.
The follow-up of patients occurs during the first year after the procedure, aimed at evaluating possible recurrences.
Caroline de Freitas Barbosa | ORCID 0000-0002-5786-5350
Contribution: Literature review, Free and Informed term of Consent preparation, participation in the surgical procedure, preparation and drafting of the manuscript
Tatiana Villas Boas Gabbi | ORCID 0000-0003-2337-1448
Preparation, drafting and approval of the final version of the manuscript, key participation and guidance in the research process, conceptual participation in the propaedeutic and/or therapeutic approach in the studied cases
1. Bryant A, Knox A. Ingrown toenails: the role of the GP. Australian Family Physician. 2015;44(3):102-5.
2. Yilmaz A, Çenesizoglu E. Partial matricectomy with cryotherapy in treatment of ingrown toenails. Acta Orthop Traumatol Turc. 2016;50(3): 262-268
3. Haneke E. Controversies in the Treatment of Ingrown Nails. Dermatology Research and Practice. 2012;2012: 783924
4. Cocunubo-Blanco HA, González-Sixto B, Pérez-paredes G, Rodríquez-Prieto MÁ. Partial nail matricectomy with carbon dioxide laser. Actas Dermosifilioqr. 2014;105(4):418-9.
5. Grover C, Khurana A, Bhattacharya SN, Sharma A. Controlled trial comparing the efficacy of 88% phenol versus 10% sodium hydroxide for chemical matricectomy in the management of ingrown toenail. Indian J Dermatol Venereol Leprol. 2015;81(5):472-7.
6. Di Chiacchio N, Di Chiacchio NG. Best way to treat an ingrown toenail. Dermatol Clin. 2015;33(2):277-82.
7. Gualdi G, Monari P, Crotti S, Calzavara-Pinton PG. Surgical treatment of ingrown toe nail: the Monaldi technique, a new simple proposal. Dermatol Surg. 2014;40(2):208-10.
8. Rosa IP, Di Chiacchio N, Di Chiacchio NG, Caetano L. "Super U"-a technique for the treatment of ingrown nail. Dermatol Surg. 2015;41(5):652-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}