


Marina Zoéga Hayashida; Mauro Yoshiaki Enokihara; Sérgio Henrique Hirata; Ival Peres Rosa
Received on: 03/10/2017
Approved on: 24/09/2018
This study was performed at the Escola Paulista de Medicina, Universidade Federal do Estado de São Paulo (UNIFESP) – São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Skin cancers in the head and neck region account for 70-75% of malignant cutaneous tumors, of which 80% are basal cell carcinomas. Between 3-6% of malignant cutaneous tumors occur in the auricular pavilion. The authors of the present paper report an alternative technique for reconstructing the ear helix after excision of tumors, without the use of the classic compensation triangle. This method allows that the scar be located in the helical sulcus, resulting in a better aesthetic result, without unaesthetic retractions or scars located transversely to the helix.
Keywords: Dermatologic surgical procedures; Ear, External; Ear neoplasms
Skin cancers of the head and neck account for 70-75% of malignant cutaneous tumors,1,2 of which 80% correspond to basal cell carcinomas.1 Ultraviolet radiation is the main risk factor,3,4 – especially in men – followed by phenotypic characteristics, such as eyes and fair skin (phototype 1), radiotherapy, iatrogenic immunosuppression, among others.
Malignant cutaneous tumors are located in the auricular pavilion in a percentage that varies from 3 to 6% of the cases.5 Carcinomas originating in this region are considered to be more aggressive and have a worse prognosis when compared to those located in the trunk and extremities.1 The auricular pavilion is basically composed of skin and cartilage; nevertheless it has a very complex anatomical structure. The ear’s helix is the main structure responsible for its shape.5 In this manner, knowing and understanding surgical techniques for the reconstruction of the helix after the excision of tumors is of paramount importance for the dermatologist physician.
The present article is aimed at describing a differentiated technique for the reconstruction of the helix after the excision of tumors, without the use of the classic compensation triangle, implying that the resulting scar is located along the ear’s helix fold, meaning a better aesthetic outcome.
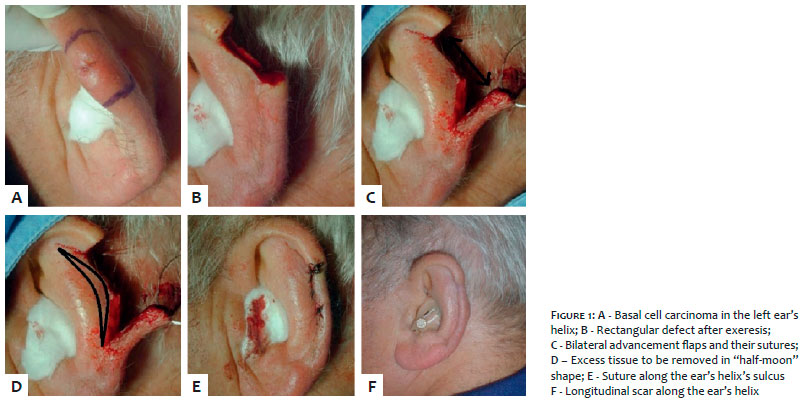
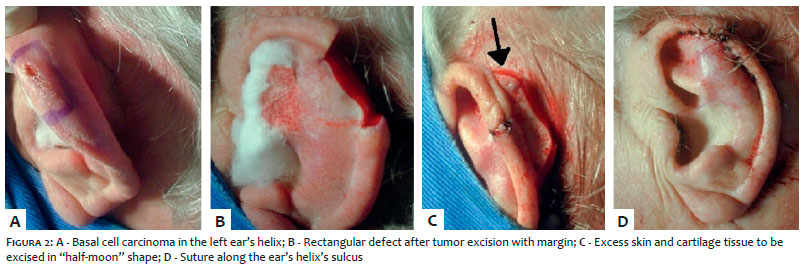
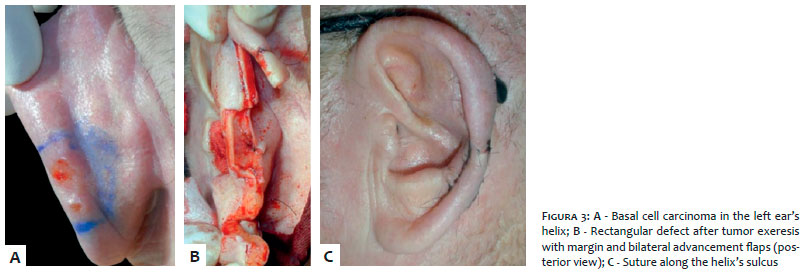
The authors of the present article illustrated the technique with 3 patients (Figures 1, 2 and 3), who presented diagnosis of basal cell carcinoma in the left ear’s helix (Figures 1A, 2A and 3A).
A rectangular defect in the ear’s helix is created after the excision of the malignant lesions (Figures 1B, 2B and 3B), with two advancement flaps being implemented horizontally on both sides of the defect (Figure 1C). The skin is then undermined and detached from the cartilage on both sides, with approximation and initial suture of the cartilage with nylon 4-0, followed by the suture of the skin with nylon 5-0. The sutures must be carried out in a staggered way, avoiding that their final positions coincide, meaning that the skin’s suture should be located slightly below or slightly above that of the cartilage, even if under minor initial tension (Figures 1C and 2C).
Next, the two advancement flaps should ideally be forced backwards, aiming at suturing them next to the cartilage that has also been projected backwards. When the sutured cartilage’s location exactly coincides with the sutured flaps’ plane, it is possible to perform the final suture directly without any compensation. When this is not possible and the cartilage is higher than the flaps (Figure 2C), the skin and cartilage of the anti-helix are removed, symmetrically and observing a “half-moon” shape, thus removing the initial tension of the flaps’ suture (Figures 1D and 2C - the arrow indicates the “half-moon” shape to be removed). Finally, the suture of the remaining anterior and posterior regions is carried out (Figures 1E, 2D and 3C).
This technique of reconstruction of the ear’s helix was performed on the three patients shown in the figures with success and complete recovery, without intercurrences. The results of the anatomopathological examination performed with the surgical specimens of all patients indicated the presence of basal cell carcinoma with free margins. The final scars are kept along the ear’s helix fold, meaning great esthetic and functional outcomes.
The auricular pavilion has a complex anatomy, which can be subdivided into ear’s helix, ear’s anti-helix, scaphoid fossa, concha, tragus, antitragus and lobe – with the ear’s helix being the main structure that lends its characteristic shape.5
When a tumor reaches the helix, there are two classic alternatives: “V” excision or rectangular removal, and advancement of two lateral flaps. However, if the flaps become very tense, both lead to the formation of a fold in the auricular pavilion, requiring the use of compensation triangles.5
In any technique of reconstruction of the ear’s helix in which two flaps are implemented, if they are directly approximated, the formation of a fold in the cartilage is inevitable. This fold is moved backwards during the surgical act and, aiming at correcting it, the traditional technique removes the excess fold with a vertical incision in triangular shape. Nonetheless, when this correction technique is used, the ear is invariably displaced anteriorly, becoming unaligned and asymmetrical when compared to the contralateral side.
In contrast, with the technique described in the present article, the two advancement flaps are forced backwards aiming at suturing them along the cartilage that was projected backwards. In some cases, it is possible to perform the suture directly, without any compensation and with better aesthetic outcome, since the ear is not projected anteriorly. In most cases, however, the position of the cartilage that has been forced backwards ends up being more elevated than that of the already sutured flaps, implying that its direct suture is unfeasible. In face of this situation, it is necessary to cut the excess in “half-moon” shape, symmetrically to the two flaps, up until it becomes possible to suture them. With this, the ear is not projected anteriorly and the suture is positioned longitudinally along the ear’s helix, thus avoiding the traditional transverse location, which is visible.
The staggered technique consists of suturing the ear’s helix’s skin and cartilage in not coinciding, diverse planes, which is crucial for a good aesthetic outcome. On the other hand, when cartilage and skin are sutured together, the healing process causes retraction, which is expressed by a visible transverse groove in the helix.
The authors of the present article exemplify an alternative technique to that of the compensation triangle. The main advantage of the proposed technique is the location of the final scar, which is positioned along the ear’s helix’s curve. It offers a better camouflage than that of the perpendicular scar resulting from the compensation triangle, in addition to decreased risk of forcing the auricular pavilion to bend forward, yielding better aesthetic outcomes.
Marina Zoéga Hayashida | ORCID 0000-0002-2960-3134
Planning, preparation, drafting and discussion of the manuscript. Monitoring of the patients
Mauro Yoshiaki Enokihara | ORCID 0000-0002-3815-7201
Supervision, guidance, discussion and editing of the manuscript. Monitoring of the patients
Sérgio Henrique Hirata | ORCID 000-0003-4026-9664
Supervision, guidance, discussion and editing of the manuscript. Monitoring of the patients
Ival Peres Rosa | ORCID 0000-0002-8463-007
Planning, drafting, supervision, guidance and discussion of the manuscript. Monitoring of the patients
1. Gallegos-Hernández JF, Martínez-Méndez MA, Ábrego-Vázquez JA, Hernández-Sanjuan M, Minauro-Munoz GG, Ortiz-Maldonado AL. Características clínicas de los tumores malignos originados en el pabellón auricular. Cir & Cir. 2015;83(6):473-7.
2. Kyrgidis A, Tzellos TG, Kechagias N, Patrikidou A, Xirou P, Bour-lidou E, et al. Cutaneous squamous cell carcinoma (SCC) ofthe head and neck: Risk factors of overall and recurrence-freesurvival. Eur J Cancer. 2010;46(9):1563-72.
3. Cannavó SP, Borgia F, Trifiró C, Aragona E. Skin and sun exposure. G Ital Med Lav Ergon. 2013;35(4):219-21.
4. Gandhi SA, Kampp J. Skin Cancer Epidemiology, Detection, and Management. Med Clin N Am. 2015;99(6):1323-35.
5. Rosa IP. Cirurgia das Orelhas. In: Gadelha AR, Costa IMC, editors. Cirurgia dermatológica em consultório. São Paulo:Ed Atheneu; 2009. p. 759-88.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}