


André Ricardo Adriano; Dâmia Leal Vendramini; Carlos Daniel Quiroz; Leonardo Pereira Quintella
Received on: 27/08/2018
Approved on: 27/09/2018
Instituto de Dermatologia Professor Rubem David Azulay, Santa Casa da Misericórdia do Rio de Janeiro (IDPRDA / SCMRJ) - Rio de Janeiro (RJ), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Photoaging results from the action of external agents, the main being ultraviolet radiation. It is clinically characterized by yellowish skin with irregular pigmentation, presence of wrinkles, atrophy, telangiectasias, decreased elasticity, and premalignant and malignant lesions. It corresponds to one of the most common dermatological complaints, requiring that dermatologist physicians keep up-to-date regarding treatments.
OBJECTIVE: To evaluate the effect of imiquimod in the treatment of photoaging.
METHODS: A prospective intervention study was carried out involving 12 female patients. The response was clinically assessed by the patient and examiner physician, and in light of histological parameters.
RESULTS: Six of the 12 patients, experienced side effects – three of which dropped out of the study. Of the 9 patients who completed the treatment, 8 perceived an overall improvement in the appearance of the skin. The examiner physician could observe improvement in 8 patients – slight in 6, and significant in 2 of them. Regarding histological aspects, there were decreases in solar elastosis (4 patients), melanin amount (5 patients) and fibrosis (4 patients).
CONCLUSIONS: Imiquimod can be an option for the treatment of photoaging, and should be evaluated in subsequent, controlled studies with larger samples.
Keywords: Skin; Skin aging; Administration, Topical
Aging comprises a number of physiological changes leading to the degradation of the human body as a whole, characterized by the decline of biological functions, structural changes and loss of adaptability to external agents. It is a progressive, time-dependent deterioration of the body as an adaptive response to environmental changes. Over time, molecular changes occur, triggering organic changes that lead to aging.1,2
Skin aging can be intrinsic and extrinsic. Intrinsic – or chronological – aging is a regular event, genetically related to the telomeres’ length, which are located at the end of the chromosomes’ arms and shorten with each cell cycle. This is due to the inability of DNA polymerase to transcribe the final sequence of the DNA strand’s bases. Ethnicity, anatomical variations and hormonal changes contribute to this phenomenon.3 On the other hand, extrinsic aging results from the action of external agents, of which ultraviolet radiation (UVR) is the main factor. The particular phenomenon caused by UVR is called photoaging.1-3
Photoaging is a cumulative process characterized by the formation of photoproducts – that cause direct damage to DNA – and reactive oxygen species (ROS) – that causes indirect damage to DNA, changes in the extracellular matrix and an increase in the inflammatory infiltrate. Reactive oxygen species activates nuclear transcription factor kappa β (NF-κβ), which induces the expression of proinflammatory cytokines, tumor necrosis factor (TNF) and endothelial growth factor (VEGF).1,2
Melanin plays a protective role for the skin regarding the action of UVR, with not only the amount, but also its distribution pattern being important parameters.1 In this manner, skin color has a fundamental influence on the photoaging process. The most widely used system to differentiate skin colors is the Fitzpatrick’s classification,4 which classifies patients’ skin into six phototypes: I. white skin that always burns and never tans; II. white skin that easily burns and tans minimally; III. pale brown skin that suffers mild burns and tans moderately; IV. brown skin that rarely burns and easily tans; V. dark brown skin that burns very rarely and easily tans; VI. black skin that never burns and easily tans.4,5
Photoaged skin is clinically characterized by a yellowish tonality, irregular pigmentation, wrinkles, atrophy, telangiectasias, with diminished elasticity, and pre-malignant and malignant lesions.6,7 In the context of photoaging, pre-malignant lesions correspond to actinic keratoses (AKs).
Actinic keratoses are benign intraepithelial neoplasias formed by the proliferation of atypical keratinocytes, which affect photoexposed areas of adults. They are mainly determined by exposure to UVR and may, throughout their development, turn into squamous cell carcinomas.8 Photoexposed areas of the tegument with clear actinic damage, sometimes clinically exhibiting AK lesions – or even non-melanoma skin cancer lesions – are termed areas of field cancerization.9-11
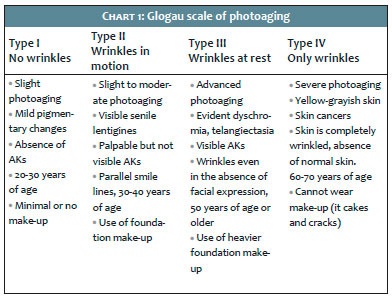
There are several proposed classifications for the gradation of photoaging. Among them, stands out the Glogau scale,12 which arranged in four stages based on clinical findings of photoaging and its diverse intensities (Chart 1).
Histologically, the photodamaged skin’s epidermis has loss of polarity, cellular atypia, increased thickness, and flattening of the dermoepidermal junction, which can lead to the appearance of atrophy. In the dermis, it is possible to observe an increase in cellularity (especially of fibroblasts), chronic inflammatory infiltrate and dilated blood vessels. The amount of elastin increases and accumulates in areas previously occupied by collagen. Photodamage is characterized by the disorganization of collagen fibers and accumulation of abnormal amorphous basophilic material, which contains elastin. This accumulation of elastotic material associated with prolonged exposure to the sun is termed solar elastosis, and characterizes photoaging. There is still little understanding on the wrinkle formation process. The development of wrinkles depends on collagen alteration, especially in the upper dermis and dermoepidermal junction. Elastosis seems to be a crucial factor.1,7
Sunscreen is still the most efficacious and cost-effective measure to fight photoaging1,13 Retinoids and 5-fluoracil are reported as topical treatment possibilities.13
Topical retinoids are classically used in pharmacological treatment of photoaging and are quoted in the literature as the first option, tretinoin being indicated with IA evidence level.1
Despite the fact that oral 5-fluoracil is not approved by the FDA and the Brazilian counterpart ANVISA as a treatment to photoaging, it was approached by Sachs et al. in 2009 open, non-randomized clinical and molecular study that, after two daily applications for 14 days in 21 patients, has been shown to be effective in treating that condition. Although the mechanism linked to this effect is not fully understood, it is known that the drug inflicts damage to the epidermis, later stimulating its healing with dermal remodeling and overall improvement of the skin’s appearance.14
Imiquimod is an immune response modifier analogous to nucleosides belonging to the imidazoquinolines family. It is approved by the FDA and ANVISA for the treatment of external genital warts, AK and superficial basal cell carcinomas, however with off-label use in the treatment of other dermatoses with variable results.15 Some studies confirm that imiquimod is a strong inducer of the immune response due to the fact it is an agonist of toll-like receptors (TLR) 7 and 8, with the NF-κβ transcription factor being activated by this signaling path, which triggers the transcription of proinflammatory cytokine genes, such as interleukins (IL) IL1b, IL2, IL6, IL8, IL12; TNF, interferon alpha (IFNa), granulocyte colony stimulating factor (GM-CSF), induction of the activation of natural killer cells (NK), CD8 cytotoxic T lymphocytes, and the production of activated B lymphocytes. Imiquimod has direct and indirect pro-apoptotic effects on tumor cells, direct and indirect effects on the induction of the Fas receptor on the cell’s surface, decrease in the Bcl-2 y protein and increase in the apoptosis regulator protein BAX.16
There are few studies on the effect of imiquimod on photoaging, however they demonstrate the presence of some benefit. Its mechanism of action on this condition is not entirely clear.17-19 Likewise 5-fluoracil, its use for this purpose is also not approved by the FDA or ANVISA.
In order to evaluate the performance of imiquimod as a topical treatment agent in photoaging – in addition to being a skin cancer chemoprophylactic – the authors of the present article carried out a study considering pre and post treatment clinical and histological changes in the presence of topical imiquimod.
An interventional longitudinal study was carried out at the cosmiatry outpatient clinic of the Instituto de Dermatologia Professor Rubem David Azulay, Santa Casa de Misericórdia do Rio de Janeiro (IDPRDA – SCMRJ), Rio de Janeiro, Brazil. The lead-time of the study was 20 weeks, with 12 weeks of imiquimod treatment, starting 4 weeks after the first contact with the patient, plus 4 weeks for the consolidation the intervention’s results.
The criteria for inclusion of patients were: signature of the consent term, age between 30 and 60 years; Fitzpatrick’s Phototype between I and IV; Glogau photoaging Type II or higher; and the not to have used anti-aging topical treatment in the previous month. On the other hand, the exclusion criteria were: pregnancy or lactancy for female patients; positive clinical examination for malignant / pre-malignant lesions on the skin; personal or family history of autoimmune diseases. Finally, patients with unrealistic expectations were also excluded.
The dependent variables used were: i) the patients’ subjective evaluation in terms of improvement or worsening, based on a satisfaction questionnaire that took into account changes in texture, brightness, vitality, pigmentation, elasticity and skin’s general quality; ii) the clinical evaluation of a investigator physician, that took into account the above criteria in addition to photographic documentation; iii) histological evaluation with pre and post-treatment biopsies, harvested from the pre-auricular region with a 4mm punch. The pathologist physician performed the examination in a blind manner, meaning he or she did not know whether the samples corresponded to pre or post-treatment biopsies, focusing on the following aspects: epidermal thickness, inflammation, granular layer’s thickness, solar elastosis, fibrosis, melanin, pigmentary incontinence, melanocytic population and presence of atypia in keratinocytes.
The independent variables used were: patient’s gender, age, education level, profession, phototype, Glogau photoaging type, skin type, texture, brightness and pigmentation.
Each patient received a box containing 20 Imiquimod sachets per month. The substance was applied by the patient all over the face at night after facial cleansing, and removed in the morning with soap and water. The product was applied from Monday to Friday, and SPF 30 sunscreen was prescribed for use every two hours during the day.
Patients were evaluated monthly. Possible adverse effects were recorded and rated. Erythema, desquamation, vesiculation, vesiculation, pruritus, burning sensation, and edema were received ratings from 0 to 3 (0 = absent, 1 = mild, 2 = moderate, 3 = intense).
The study began with the recruitment of patients. In this first contact, demographic, clinical, and photographic data were collected, with a biopsy being performed. After 4 weeks, the drug was supplied for the patients to apply at home. The patients returned for evaluation every 4 weeks. After 12 weeks of treatment, new clinical and photographic data were collected, as well as a new biopsy performed, for histological examination. A patient satisfaction questionnaire was also administered at this experimental timepoint.
The data obtained from the questionnaires, forms and photographs were entered in Microsoft Excel spreadsheets, with subsequent descriptive analysis being carried out.
The study was evaluated and approved by the Institution’s Ethics Committee and conducted in compliance with all ethical principles applicable to clinical research, in accordance with local regulatory requirements.
The sample consisted of 12 female patients with a mean age of 52.1 years (SD: 6.06). All patients were literate, with 5 of them holding at least a Secondary Education degree. Only 2 female patients carried out professional activities while exposed to the sunlight.
The vast majority of the patients were rated with at least Type III, according to the Fitzpatrick phototypes classification. In the pre-treatment analysis, 9 patients were rated with Glogau Type III, according to the Glogau scale of photoaging, indicating the presence of expressive photoaging.
Four fundamental parameters were evaluated in the pre-treatment clinical examination, which yielded the following results: predominance of oily (5/12) or mixed skin (5/12); regarding the skin’s texture, 4 patients had rough skin; 7 had dull skin, with loss of natural vitality; facial hyperchromia (represented by melanoses and solar lentigines) were present in 9 patients.
Among the 12 patients participating in the study, 6 experienced adverse effects during the treatment, managed with momentary interruption of the protocol, associated with emollients and short courses of topical combination of corticoid with antibiotic. Notwithstanding, 3 of these 6 patients chose not to continue with the treatment. There was, however, no discontinuation due to loss of follow-up or even by medical contraindication.
Of the patients who experienced adverse effects, 1 had Glogau Type II, with the remaining 5 classified as Type III.
Nine patients completed the study. Based on the subjective evaluation questionnaires answered by the patients after the proposed treatment, the following outcomes were perceived: 8/9 had smooth or very smooth skin texture; of these, half had rough skin prior to the treatment; 7/9 had normal (not oily) skin at the end, while at the beginning they complained of oily or mixed skin; likewise, of the 9 patients treated for the proposed period, 5 experienced the return of the skin’s natural brightness and vitality, while these same 5 previously complained of dull skin; regarding pigmentation, 6 patients who had evident hyperchromia in the pre-treatment clinical examination, experienced whitening, with the facial skin becoming homogeneously fairer (it is important to highlight that 1 patient did not notice difference, and 2 complained of worsening.
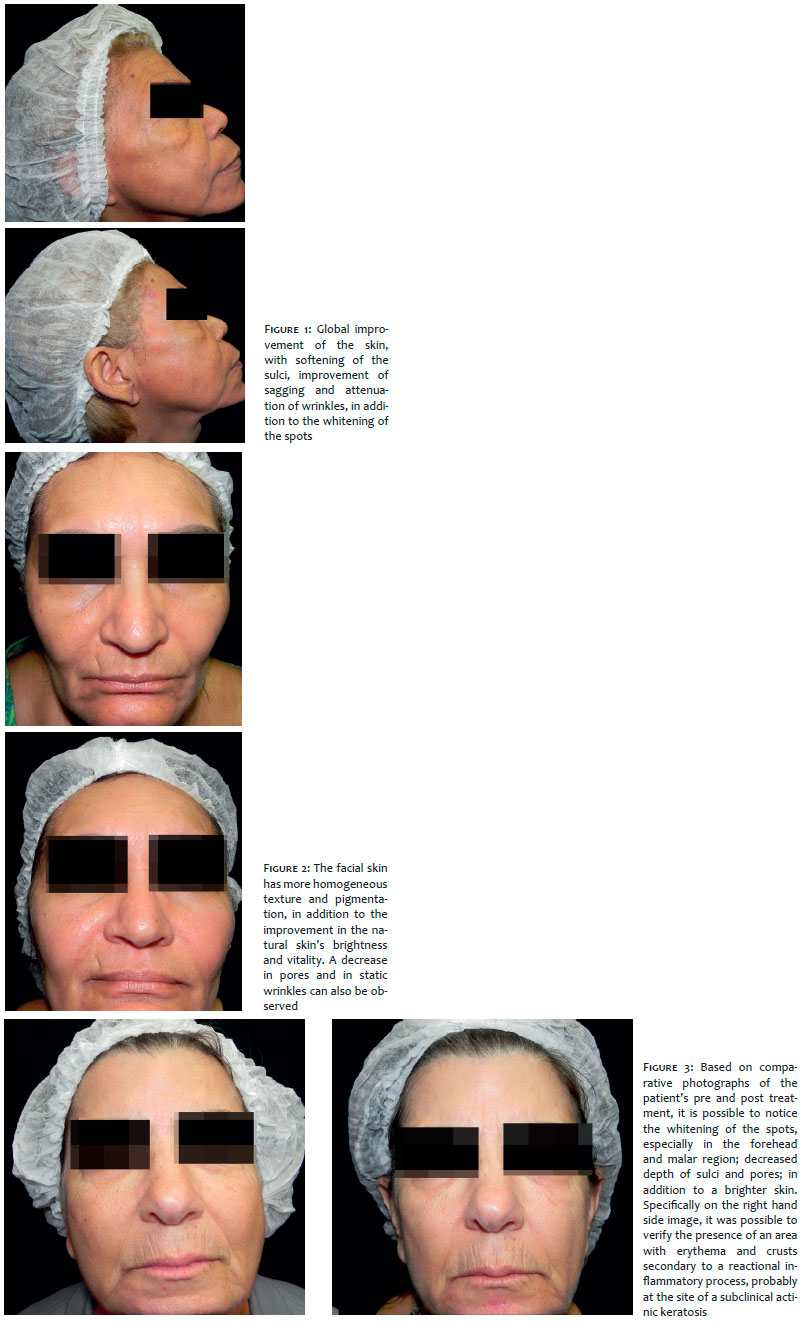
At the end of the treatment, 8/9 patients perceived improvement and were satisfied with the treatment. Of these 8, all would recommend the treatment – however 1 of these patients concedes that there are other treatments, perhaps with superior results (Figures 1 to 3).
The clinical examination performed by the examiner physician at the end of treatment evidenced improvement in 8/9 patients. Of the patients who experienced improvement, 6 had their improvement rated as significant, while 2 had their improvement rated only as slight.
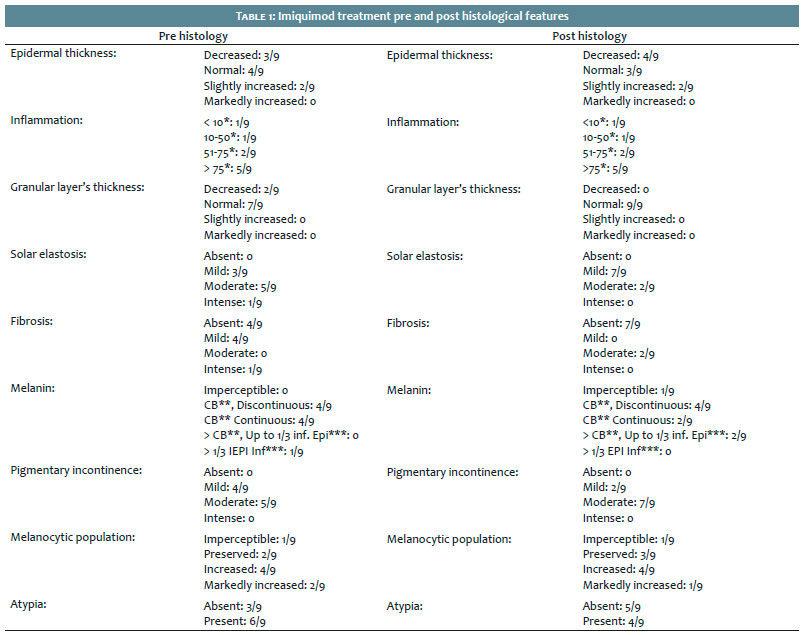
The pre and post-treatment histological characteristics of the 9 patients who completed the study are presented in Table 1.
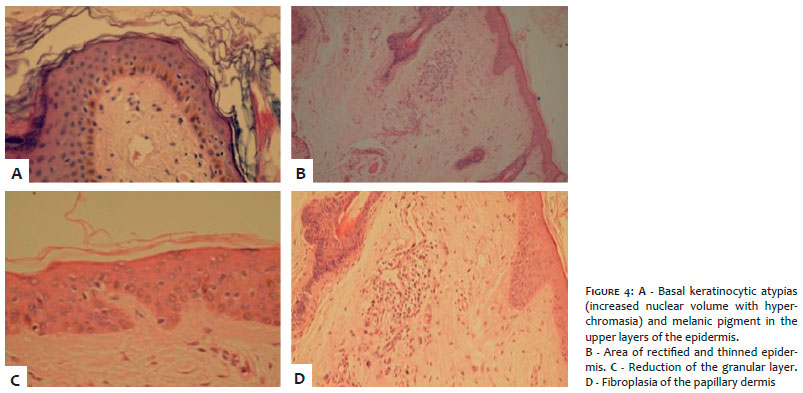
Regarding the intervention’s histological outcomes, 4 patients who already had epidermis with normal or increased thickness maintained these characteristics; 2 patients, however, coursed with normalization of thickness. On the other hand, thinning of the epidermis was observed in 3 cases. Only 2/9 patients had a decreased granular layer in the pre-treatment period, while the others had this epidermal parameter with normal thickness. Nonetheless, there was normalization of the granular layer’s thickness in these 2 cases. There was no change in the parameter inflammation (Figures 4 and 5).
Five patients had reduction of solar elastosis after the treatment. In contrast, only 1 patient experienced an increase in the degree of fibrosis in the papillary dermis, while 3 had their degrees unchanged, with reduction in 5 patients. Four patients had their amounts of melanin decreased, while another 3 did not experience change in melanin. It should be noted that 1 patient experienced an increase in melanin after the treatment. Regarding pigmentary incontinence, the majority (7/9) did not experienced change, while 2 patients presented increases. The melanocytic population, however, remained unchanged, decreased or increased in equal proportions. Finally, 2 patients with pre-treatment keratinocytic atypia did not present it in the second experimental timepoint.
A clinical and histological study of the outcomes obtained with the application of imiquimod for the reversion of photoaging in a series of patients was carried out.
The sample comprised solely female patients, with a mean age that approached the upper cut of the inclusion criteria (up to 60 years of age), meaning a more advanced chronological age. The vast majority had Fitzpatrick phototypes Grade III or superior and was rated as Glogau Type III.
In 2006, Kligman et al. published a series of ten cases of female patients treated with imiquimod aiming at evaluating the drug’s therapeutic efficacy in photoaging. As compared to that study, in which the mean age was 45 years and there was presence of lower phototypes (Grade II), the present study’s sample had a higher mean age and included higher phototypes.17 That same study did not use the Glogau scale, however it described its sample in a more generalized manner and with moderate signs of photodamage – fine periorbital wrinkles, depigmentation, slight roughness and loss of elasticity – which would amount to Type II on the Glogau scale of photoaging. Therefore, it is possible to conclude that the sample’s photoaging was less expressive than that in the present study.
Still regarding the sample’s profile, it is important to highlight that the majority of the patients had at least a full secondary education degree, and 5/12 had completed higher education. Most of the patients’ professional activities did not involve exposure to the sunlight. In light of these two aspects, the authors of the present study emphasize how much is still lacking in terms of prevention given that the sample group of patients with sufficient intellectual capacity bears expressive photodamage – probably due to recreational exposure to the sunlight without adequate photoprotection care.
The present study had a 25% loss during the treatment protocol. A study by Metcalf et al. evaluated the use of imiquimod with daily application for 12 weeks, with the initial purpose of treating patients with clinical and histological diagnosis of lentigo maligna. Based on this sample and outcomes, they performed a parallel evaluation of the action of imiquimod on photodamaged skin associated with lentiginous lesions. In total, 28 patients participated in this open trial, with 26 of them completing the treatment.8 In a study by Kligman et al. the 10 included patients completed the proposed four-weeks period of treatment.19
The determining factor for treatment withdrawal in the present study was the occurrence of side effects in half of the patients. Among the patients who developed adverse events linked to the study’s intervention, half chose to discontinue the treatment. Erythema, desquamation and pruritus were the most prevalent adverse effects, having also been evaluated as the most intense, according to the proposed rating. Regarding the adverse effects that occurred, it is relevant to highlight two important aspects: the 3 patients who abandoned the study were more symptomatic, having reported pruritus or burning sensation with higher intensities; in addition, of the 6 patients who experienced side effects, 5 were classified with Glogau Type III in the pre-treatment phase, therefore with a higher degree of photodamage and, possibly, a greater tendency to the presence of subclinical AK.
Although the study by Metcalf et al. has recorded that 2 patients did not reach the end of the study’s treatment period, neither the percentage of side effects nor even the reason for discontinuation were described.19 In the series of 10 cases treated by Kligman et al., none of the patients experienced adverse effects linked to the application of imiquimod in the proposed interval. However, 3 of the 10 patients had an episode of herpes simplex labialis, all 3 of whom presented a previous history of recurrent herpes.17 Again, it is important to emphasize the aspect of the present study’s shorter treatment time. There were no episodes of herpes simplex among the 12 patients included.
Kligman et al. observed that although their sample was comprised of patients with lower phototypes, photoaging was not as expressive and there was probably no significant number of subclinical AKs, with reactions inherent to the treatment not having therefore been observed.17 This aspect is relevant, since the effectiveness of imiquimod in the treatment of AK is established, either as a focal treatment of the lesions10 or as a field cancerization treatment.11 Some degree of inflammatory reaction is expected to take place along the course of the treatment of AK. The authors of the present study could observe the following symptoms in the 6 patients who experienced side effects: circumscribed areas of erythema, desquamation, vesiculation and / or edema, in varying degrees, accompanied by subjective symptoms. In none of the cases this reaction occurred in a diffuse way, throughout the imiquimod application area. The authors of the present study believe that the focal aspect of the adverse reaction reinforces the hypothesis of the possible presence of subclinical AK lesions.
The authors of the present study deem the evaluation carried out by the patients themselves as fundamental, even considering the subjectivity inherent to this type of analysis, since it evidences the perception of the treatment by the most interested part. At the end of the 12 weeks, most of the patients’ self-assessments identified an improvement in the signs of skin aging. This improvement was especially linked to the skin’s texture and brightness, whitening, in addition to the control of oiliness.
In their study, Metcalf et al. did not report the patients’ impressions as a therapeutic outcome.19 Kligman et al. also demonstrated the presence of subjective improvement from the patient’s point of view, classifying it into slight improvement (1/10), moderate improvement (5/10), and great improvement (4/10). According to the patients, the improvement was attributed to the skin’s texture (which became smoother) and whitening of the hyperpigmentation (which led to a more homogeneous coloration of the facial skin), as well as to the reduction of fine wrinkles.17
From the clinical examination point of view, a significant improvement was observed in most patients. The only patient who did not realize improvement with the treatment was the one who had been considered unresponsive to the therapy during the clinical examination and follow-up.
Again, the study by Metcalf et al. does not refer to clinical improvement.19 On their turn, Kligman et al. report improvement in 9 of the 10 patients, from the examiner physician’s point of view. However, regarding the degree of improvement, 5/10 had mild improvement, and 4/10 moderate – meaning that no patient experienced a huge benefit.17
From the histological point of view, 4/9 coursed with a decrease in epidermal thickness, with 3/9 having experienced thinning of their epidermis, while 1/9 experienced normalization of their epidermis’ thickness. Two of the 9 patients who had thin granulation layers coursed with normalization. Four of the 9 patients experienced decreased inflammation. There was a decrease in solar elastosis in 4/9 patients. Only 1 of the 9 patients presented increased fibrosis after the treatment. There was a decrease in the amount of melanin in 5/9 patients, with a reduction in the melanocytic population being observed in 3/9. Among the 6 patients who had keratinocytic atypia in the pre-treatment phase, 2 developed with normalization.
Considering the treatment of photoaging, histological improvement is deemed as the increase of both the thickness of the epidermis and the amount of collagen in the papillary dermis, combined with the reduction of solar elastosis.7
The findings of Metcalf et al. were more expressive, with 92.3% of patients coursing with increased fibroplasia in the papillary dermis, associated with the reduction of solar elastosis, in addition to the restoration of the epidermis’ normal thickness. All these findings were statistically significant.19 Kligman et al. generically report that in the hematoxylin-eosin evaluation, patients presented epidermis of normal or acanthotic thickness, with the complete normalization of epidermal dysplasias and reduction of the melanocyte population, without, however, clarifying the frequencies with which those changes occurred. They conclude that, from a histological point of view, modifications caused by imiquimod would be restricted to the epidermis, without having observed any effects on the dermis in their study.17
Smith et al. published a study containing histological and immunohistochemical findings before and after treatment of photoaging with 5% imiquimod in cream, applied three times a week, for a period of four weeks. Of the 12 patients who were treated, 11 were included in the analysis. The normalization of the stratum corneum was observed in all 11 patients (all showed some degree of hyperkeratosis in the pre-treatment phase). Seven presented acanthotic epidermis, and all coursed with normalization of epidermal thickness. In contrast, the remaining 4 who had atrophic epidermis also experienced normalization of the epidermal thickness at the end of the treatment. Finally, 6 of the 11 patients presented increased stromal cells amid areas of solar elastosis. It is worth noting that the study by Smith et al. did not provide clinical evaluation of the patients.18
The findings of the present study were in line with the few studies found by the authors in a bibliographic review. The authors consider that despite the non-controlled character of the intervention and the relative small size of the sample, the present study contributes with the demonstration of results in agreement with the proposed parameters, and may be the precursor of further research. Based on the patients’ subjective evaluations, clinical evaluation performed by a researcher dermatologist physician, and histological evaluations, the authors conclude this study (a series of photoaging cases treated for 12 weeks with a daily application of imiquimod) by stating that imiquimod may be an option for the treatment of photoaging and should be evaluated in subsequent, controlled studies with larger samples.
We would like to thank Dr. Carla Tamler and Dr. Ana Carolina Amaral for the incentive to perform the study. We would also like to thank Dr. Gustavo Amorim for the support and review of the manuscript.
André Ricardo Adriano | ORCID 0000-0002-2986-959X
Approval of the final version of the manuscript; Design and planning of the study; Conception and drafting of the manuscript; Data collection, analysis and interpretation; Intellectual participation in propaedeutic and / or therapeutic management of the cases studied; Critical review of the literature
Dâmia Leal Vendramini | ORCID 0000-0002-6841-6323
Statistical analysis; Approval of the final version of the manuscript; Conception and drafting of the manuscript; Data collection, analysis and interpretation; Critical review of the literature
Carlos Daniel Quiroz | ORCID 0000-0002-4052-9457
Statistical analysis; Conception and planning of the study; Effective participation in research guidance; Intellectual participation in propaedeutic and / or therapeutic management of studied cases
Leonardo Pereira Quintella | ORCID 0000-0002-2076-8776
Data collection, analysis and interpretation; Intellectual participation in propaedeutic and / or therapeutic management of studied cases
1. Rabe JH, Mamelak AJ, McElgunn PJ, Morison WL, Sauder DN. Photoaging: Mechanisms and repair. J Am Acad Dermatol. 2006; 55(1):1-19.
2. Montagner S, Adilson C. Molecular basis of photoaging. An Bras Dermatol. 2009;84(3):263-9.
3. Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: a Review. Int J Cosmet Sci. 2008;30(2): 87-95.
4. Fitzpatrick T. The validity and practicality of sun- reactive skin types I through V1. Arch Dermatol. 1988;124(6):869-71.
5. Fairley JA in: Bolognia JL, Jorizzo JL, Rapini RP. Dermatology. 2ª ed. [tradução Renata Scavona de Oliveira. et al.]. Rio de Janeiro: Elsevier; 2011. 691-8.
6. Zouboulis CC, Makrantonaki E. Clinical aspects and molecular diagnostics of skin aging. Clin Dermatol. 2011;29(1):3-14.
7. Kohl E, Steinbauer J, Landthaler M, Szeimies M. Skin Ageing. J Eur Acad Dermatol Venereol. 2011;25(8):873-84.
8. Schmitt JV, Miot HA. Actinic keratosis: a clinical and epidemiological revision. An Bras Dermatol. 2012;87(3):425-34.
9. Ulrich M, Krueger-Corcoran D, Roewer-Huber J, Sterry W, Stockfleth E, Astner S. Reflectance Confocal Microscopy for Noninvasive Monitoring of Therapy and Detection of Subclinical Actinic Keratoses. Dematol. 2010;220(1):15-20.
10. Hadley G, Derry S, Moore RA. Imiquimod for actinic keratosis: systematic review and meta-analysis. J Invest Dermatol. 2006;126(6): 1251-5.
11. Dréno B, Amici JM, Basset-Seguin N, Cribier B, Claudel JP, Richard MA. Management of actinic keratosis: a practical report and treatment algorithm from AKTeam expert clinicians. J Eur Acad Dermatol Venereol. 2014;28(9):1141-9.
12. Glogau RG. Chemical peeling and aging skin. J Geriatr Dermatol. 1994; 2:30-5.
13. Poon F, Kang S, Chien AL. Mechanisms and treatments of photoaging. Photodermatol Photoimmunol Photomed. 2015;31(2): 65-74.
14. Sachs DL, Kang S, Hammerberg C, Helfrich Y, Karimipour D, Orringer J, et al. Topical fluoracil for actinic keratosis and photoaging: a clinical and molecular analysis. Arch Dermatol. 2009;145(6):659-66.
15. Hanna E, Abadi R, Abbas O. Imiquimod in Dermatology: an overview. Int J Dermatol. 2016;55(8):831-44.
16. MP Schön, Schön M. Imiquimod: mode of action. Br J Dermatol. 2007;157 (Suppl 2):8-13.
17. Kligman AM, Zhen Y, Sadiq I, Stoudemayer T. Imiquimod 5% Cream Reverses Histologic Changes and Improves Appearance of Photoaged Facial Skin. Cosmet Dermatol. 2006;19(11):704-711.
18. Smith K, Hamza S, Germain M, Skelton H. Does Imiquimod Histologically Rejuvenate Ultraviolet Radiation-Damaged Skin. Dermatol Surg. 2007;33(12):1419-29.
19. Metcalf S, Crowson N, Naylor M, Haque R, Cornelison R. Imiquimod as an antiaging agent. J Am Acad Dermatol. 2007; 56(3):422-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}