


Atefeh Shahbazi1; Marzieh Nikoo2; Masoud Habibi3; Mohammad Hasan Naseh2,4; Seyed Mohammad Akrami5; Hamid Choobineh5
Received on: 15/03/2018
Approved on: 01/08/2018
This study was performed at the University of Medical Sciences of Tehran - Tehran, Iran.
Financial support: None
Conflict of interests : None
INTRODUCTION: Vitiligo is a hypopigmented disorder characterized by irregular loss of of the skin pigmentation. Current therapeutic modalities focus on increasing melanin production and modulating immune system responses. The use of some combined topical agents, in appropriate concentrations, is a possibility for the treatment of such hypopigmentation disorders.
OBJECTIVE: To follow-up patients who used a combination of creams in the experimental times of 6 and 14 months and to determine the effectiveness of the formulation.
METHODS: Forty-one patients with generalized stable vitiligo participated in the study. Patients applied a cream containing acetyl hexapeptide-1, mometazone furoate and dihydroxyacetone. The sites of the lesions included eyelids, forehead, face, neck, fingertips, hands, feet and legs. The variations in the treated patches were evaluated by dermatologists at each experimental visit. The percentage of repigmentation was evaluated after 6 months.
RESULTS: After 6 months of treatment, 8 patients (19.51%) had an excellent response to treatment, while a good response was observed in 19 patients (46.34%), moderate response in 10 (24.39%), and unsatisfactory in 4 (9.75%). Eyelids, face and forehead presented the best rate of repigmentation, while fingertips response was generally unsatisfactory.
CONCLUSIONS: The data support the efficacy of the new cream evaluated by the present study.
Keywords: Skin Pigmentation; Skin Cream; Vitiligo
Vitiligo is a complex autoimmune disorder of hypopigmentation characterized by irregular pigmentation loss of the skin and destruction of functional melanocytes in the epidermis that can affect any part of the body that has pigmented cells.1,2 The prevalence of this pigmentation disorder in the world population is estimated between 0.1% and 8%, without differences of race or gender. Although this disease has been known for a long time, its exact etiology is still a matter of debate and studies on efficient treatments are still in progress. Several treatment modalities were developed for repigmentation of patients with vitiligo,3-6 including non-invasive therapies and surgical techniques. Non-invasive treatments used for vitiligo include combined ultraviolet A (PUVA, administered 2-3 times per week and generally continued for several years), ultraviolet B narrowband (UVB-NB), Excimer laser, topical steroids, topical immunomodulators and calcipotriol. On the other hand, surgical methods may be a treatment alternative for patients with stable leukoderma.7,8
Lack of response to treatment is common in some body sites, especially in the hands and feet. In this manner, topical treatments consist of creams containing one or more chemical agents.9 The authors of the present study introduce a cream called DN Vitil Cream, which contain three main chemical agents: Elocon® (Mometasone furoate), Melitane® (acetyl hexapeptide-1), and DHA (dihydroxyacetone). Several studies have suggested that preparations containing corticosteroids may promote repigmentation of the skin affected with vitiligo.10,11 Topical corticosteroids are anti-inflammatory and immunosuppressive agents and various forms of these components that have the ability to alter the skin’s immune function are used as a treatment for vitiligo. Mometasone furoate is a safe and potent synthetic corticosteroid with anti-inflammatory action that is used in the treatment of diseases such as psoriasis and atopic dermatitis. Nevertheless, few studies have been found regarding its role in the treatment of vitiligo as compared to other dermatological conditions.14-16 The use of other chemical agents, such as α-MSH analogues, which act on melanocytes enhancing their proliferation as well as melanogenesis, is equally essential in the treatment of vitiligo.17 Melitane® is a synthetic peptide that has anti-inflammatory and melanogenesis-promoting properties, however its effect on patients with vitiligo has not yet been evaluated.18
One of the main goals of the treatments for patients with vitiligo is to lessen psychological distress and improve their quality of life. Cosmetic camouflage is an ancient and useful treatment.19 In fact, it is not a real solution, however it can be suggested when patients are not motivated enough to adhere to non-cosmetic treatments. Dihydroxyacetone (DHA) is a well-known 3-carbon sugar that causes brown skin coloration through the polymerization of amino acids in the stratum corneum’s cells.20-21
In the present study, the authors demonstrate that the combination of these three components, in specific concentrations, in a new cream formulation can act synergistically via the activation of pathways, such as: melanocyte stimulation, melanogenesis, modulation of immune system responses, and camouflage of areas under treatment. All these approaches have led to positive results in patients with vitiligo. The authors of the present study selected 41 patients with vitiligo – with a generalized and stable pattern – aimed at studying repigmentation after the use of this combination of therapeutic agents. Likewise, they report their experience with 41 other patients who used various treatments, such as ultraviolet (UV), light therapy and transplantation of non-cultured melanocytes, with absence of results.
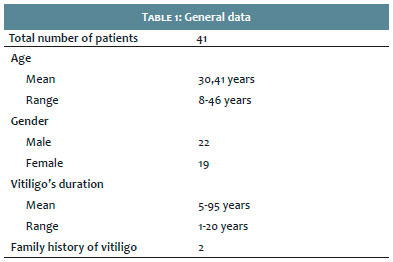
Forty-one patients (22 men and 19 women) bearing generalized stable vitiligo who had not been treated for the disease during the previous 6 months were selected for the present study.
All patients signed an Informed Consent Term provided by the Dermatology Department of the Helal Iran Pharmaceutical and Clinical Complex, and the study was conducted according to the principles of the Helsinki Declaration.
Prior to beginning treatment, basic patient data, as well as medical history, including body site, progression, and duration of the vitiligo lesions were evaluated. The exclusion criteria were: any progression of the disease during the previous 6 months, lesions extending for more than 20% of the total body area, being an active or passive smoker, pregnancy, lactation and any concomitant medical treatment during the previous 6 months.
The patients’ age ranged from 8 to 46 years (mean = 30.41 years) (Table 1). Disease stability was defined as the total absence of new spots or increase in the existing lesion’s size during the previous 6 months. All important laboratory diagnostic tests were performed. The antiperoxidase antibody of all patients was checked, with results within the normal range, and the clinical protocols completely met. The active components of the new formulation were mixed by shaking for 4 hours at 22-25°C, in the following proportions: 10% of 0.1% Mometasone furoate, 2% of Acetyl hexapeptide-1, 1% of Dihydroxyacetone, creamy vehicle – QS.
The study patients applied this new combination of active principles once a day on their vitiligo lesions. The lesions’ sites where the cream was applied included the eyelids, forehead, face, cervical region, extremities of the fingers, hands, feet and legs. Dermatologists evaluated the variation that ensued in treated spots with digital photographs taken at each visit under natural light and Wood’s lamp.
The photographs were taken before and after the use of the cream. Some of them were damaged due to technical problems. Repigmentation percentage was evaluated six months later and rated according to the following categories, for each side of the body: absence of repigmentation (0-25%), moderate repigmentation (26-50%), satisfactory repigmentation (51-75%), excellent repigmentation (76-100%).
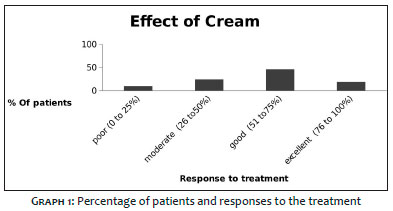
Forty-one patients (22 men and 19 women) bearing generalized stable vitiligo were selected and treated. Their ages ranged from 8 to 46 years old, and all had a history of generalized and stable vitiligo for more than 1 year. They were asked about concomitant disorders, with none offering positive answers. The vitiligo areas did not involve more than 10% of the patients’ skin and the results indicate the effects of the treatment on several body areas. The overall evaluation of these effects in each of the 41 patients after 6 months of treatment yielded the following results, which are also depicted in Graph 1:
Of the 41 patients with generalized vitiligo, 8 (19.51%) had excellent response to the treatment, 19 (46.34%) had satisfactory response, 10 (24.39%) had moderate response, and 4 (9.75%) coursed with absence of repigmentation after 6 months of treatment with the combination of the studied active principles (Graph 1).
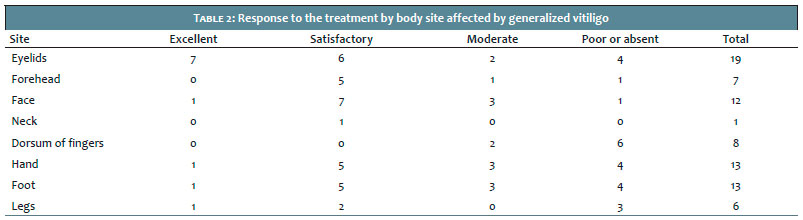
The analysis of the response classified by body site suggested that eyelids, face and forehead underwent repigmentation with better consistency. On the other hand, the response to the treatment on the dorsum of the fingers was unsatisfactory (Table 2). Initial hyperpigmentation began gradually after 2 months, especially on the forehead.
The dermatological examination after 6 months evidenced that the recent pigmentation was similar to that of the surrounding skin.
A number of studies show abnormalities in humoral and cellular immunity in patients with vitiligo.22-23 These studies indicate the presence of an autoimmune disorder that could occur in melanocytes, which produce pigmentation.24 The outcomes of current therapeutic modalities for vitiligo generally remain variable, with frequent observation of resistance to treatment.25
Topical formulations contain active ingredients (often drugs or botanical essences), and a vehicle. During the development of new topical formulations (creams, ointments, gels etc), small differences in the formulation may produce surprising effects on the efficacy of a medication, resulting in high effectiveness in the treatment of patients.26
The authors of the present study focused their efforts on developing a new drug-based treatment for cases that do not respond to other therapies. For this, patients with stable vitiligo were selected, meaning that no new spot had arisen during the previous 6 months. Patients with limited white patches, located on the eyelids, forehead, face, neck, dorsum of the fingers, hands, feet and legs were also selected.
The new cream formulation is soluble and composed of different agents combined in specific concentrations, and was named DN Vitiligo Cream. The use of immunosuppressive agents has been studied in the treatment of vitiligo. One of the oldest and most widely used methods for treating vitiligo is topical corticosteroids, whose efficacy can be attributed to multiple mechanisms, such as their anti-destructive action that protects melanocytes, the prevention of immunological changes, T-cell blockade and stimulation of melanocyte reactivation.27 Among these corticosteroids, mometasone furoate, a class 3 corticosteroid, has been shown to be effective and long-acting in all body sites. Mometasone furoate is available in cream, ointment and lotion for the treatment of different dermatological conditions, including atopic dermatitis, seborrheic dermatitis, scalp psoriasis and psoriasis vulgaris.15,29 Its ability to suppress immune changes by inhibiting inflammatory mediators (such as leukotriene, interleukins (IL) -1, IL-4, IL-5, IL-6, interferon-¿, tumor necrosis factor -α and IL-8, which led to the inhibition of T-cell activation) was studied. As a result, mometasone furoate is a drug that is acceptable for the treatment of vitiligo, isolated or in combination. Current treatment modalities simultaneously potentiate the action and proliferation of melanocytes, modulating the immune system. ¿lpha-MSH analogues are components that bind to melanocortin-1 (MC1-R) receptors in keratinocytes and melanocytes, inducing intracellular pathways, which lead to melanogenesis and anti-inflammatory processes.31 Studies have shown that the combination of α-MSH analogues with other therapies resulted in higher repigmentation rates. Acetyl peptide-1 is one of these effective substances, having been used for the first time in combination with other active ingredients in the new cream. In this manner, these 2 active principles used in the new cream have effective action in the mechanism of the disease.
Dihydroxyacetone is an active agent used in cosmetic creams in order to cover white patches of the epidermis. Due to the psychosocial effectiveness of cosmetic camouflage in vitiligo patients, the authors of the present study used it in the new formulation. Dihydroxyacetone reacts only with the skin’s corneocytes and has the advantage of being water resistant.19-20 Some studies have demonstrated correlation of the homogenization of the patches’ coloration with the DHA’s concentration in various skin types, suggesting that darker-skinned individuals require higher concentrations of that active principle. Similarly, the intensity of the skin’s color directly correlates with the thickness and compaction of the stratum corneum due to the fact that DHA reacts only with that skin layer. Rougher and more hyperkeratotic skins, as well as older or mottled skins, absorb the pigment more unevenly. Scales should be removed by mechanical friction or chemical peel before the application of DHA. Hair and nails absorb the agent’s staining, which does not occur with the mucous membranes.
In the present study, the authors evaluated the efficacy of a cream with an innovative formulation containing mometasone furoate, acetyl hexapeptide-1 and DHA in 41 patients with generalized vitiligo, demonstrating the presence of acceptable repigmentation, since only 9.75% of patients experienced unsatisfactory responses.
In the present study, the authors assumed that satisfactory outcomes for the patients would be an indicator of sufficiency for indication of use of the new cream for the treatment of the disease. In line with that assumption, the present study demonstrated that this combination led to satisfactory results when compared to other treatments, suggesting that the components in question may be more effective when associated than isolated. The present study also found that the proximal regions, including the eyelids, face and forehead, had better repigmentation, whereas dorsum of the fingers (glabrous skin) presented unsatisfactory repigmentation, with the lack of melanocyte reserves in these areas being the main reason for the poor outcome. The authors hypothesize that the therapeutic effects of the new cream’s formula may be due to the mometasone furoate’s capacity of suppressing the immune response, as well as to the efficacy of acetyl hexapeptide-1 in inducing melanogenesis. In addition, the DHA’s camouflage effect improved the final outcome. The authors believe that changes in the concentration of the components in the new cream may further improve their effectiveness.
The statistical analyses were performed using the softwares R (version 3.2.4) and SPSS (version 16.0). The binomial test was used to evaluate differences between proportions. The chi-square test was used to test the association of categorical variables. The Spearman correlation coefficient was used to analyze the correlation between variables. Based on the correlation between the experimental observations, the multilevel analysis was performed to evaluate the effects of covariates on response variables. P-values less than 0.05 indicated statistical significance.
The authors presented results that confirm that the active principles contained in the studied formulation were sufficiently effective in the repigmentation of the stained skin.
The authors of the present article would like to thank the teams working at the Dermatology Clinic of the Pharmaceutical and Clinical Complex of Helal Iran and at the Behrooyan Dermatology Clinic for sharing their experience and advice. We would also like to thank the patients and their families for participating in this study.
Atefeh Shahbazi
Elaboration and drafting of the manuscript, critical review of the literature, critical review of the manuscript
Marzieh Nikoo
Review and approval of the final version of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Masoud Habibi
Review and approval of the final version of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Mohammad Hasan Naseh
Review and approval of the final version of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Seyed Mohammad Akrami
Review and approval of the final version of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Hamid Choobineh
Review and approval of the final version of the manuscript, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
1. Stromberg S, Björklund MG, Asplund A, Rimini R, Lundeberg J, Nilsson P, et al. Transcriptional profiling of melanocytes from patients with vitiligo vulgaris. Pigment Cell Melanoma Res. 2008;21(2):162-71.
2. Hong WS, Hu DN, Qian GP, McCormick SA, Xu AE. Ratio of size of recipient and donor areas in treatment of vitiligo by autologous cultured melanocyte transplantation. Br J Dermatol. 2011;165(3): 520-5.
3. Strömberg S, Björklund MG, Asplund A, Rimini R, Lundeberg J, Nilsson P, et al. Transcriptional profiling of melanocytes from patients with vitiligo vulgaris. Pigment cell melanoma res. 2008;21(2):162-71.
4. Lin SJ, Jee SH, Hsiao WC, Yu HS, Tsai TF, Chen JS, et al. Enhanced cell survival of melanocyte spheroids in serum starvation condition. Biomaterials. 2006;27(8):1462-69.
5. Gendreau I, Angers L, Jean J, Pouliot R. Pigmented Skin Models: Understand the Mechanisms of Melanocytes. 2013.
6. Hong W, Hu DN, Qian GP, McCormick SA, Xu AE. Ratio of size of recipient and donor areas in treatment of vitiligo by autologous cultured melanocyte transplantation. Br J Dermatol. 2011;165(3): 520-5.
7. Westerhof W. The discovery of the human melanocyte. Pigment Cell Res. 2006; 19(3):183-93.
8. Lin SJ, , Jee SH, Hsiao WC, Yu HS, Tsai TF, Chen JS, et al. Enhanced cell survival of melanocyte spheroids in serum starvation condition. Biomaterials. 2006;27(8):1462-9.
9. Travis LB, WeinbergJM, Silverberg NB. Successful treatment of vitiligo with 0.1% tacrolimus ointment. Arch Dermatol. 2003;139(5): 571-4.
10. Kandil E. Vitiligo--response to 0.2 percent betamethasone 17-valerate in flexible collodion. Dermatologica. 1970;141(4): 277-81.
11. Kandil E. Treatment of localized vitiligo with intradermal injections of triamcinolone acetonide. Dermatologica. 1970;140(3): 195-206.
12. Yeomans JS, Koopmans HS. Letter: On the directionality of medial forebrain bundle fibers mediating self-stimulation. Science. 1974;183(4120):102-3.
13. Kandil E, Treatment of vitiligo with 0-1 per cent betamethasone 17-valerate in isopropyl alcohol--a double-blind trial. Br J Dermatol. 1974;91(4): 457-60.
14. Chang RK, Raw A, Lionberger R, Yu L. Generic development of topical dermatologic products: formulation development, process development, and testing of topical dermatologic products. AAPS J. 2013;15(1):41-52.
15. Popper TL, Gentles MJ, Kung TT, Berkenkopf J, Lutsky BN, Watnick AS, et al. Structure-activity relationships of a series of novel topical corticosteroids. J Steroid Biochem. 1987;27(4-6):837-43.
16. El Nazer H, Emam H, F. Abdel Hamid M, Aly D, Shehata H, Hussein M, et al. The effectiveness of narrow-band phototherapy, corticosteroid, and methotrexate on clinical picture and serum level of soluble interleukin-2 receptors among vitiligo patients. Medical Research Journal. 2011; 10:18–22.
17. Lim Henry W, Grimes Pearl E. Afamelanotide and Narrowband UV-B Phototherapy for the Treatment of Vitiligo. JAMA Dermatol. 2015;151(1):42-50.
18. Zhang L, Falla TJ. Cosmeceuticals and peptides. Clin Dermatol. 2009;27(5):485-94.
19. Rajatanavin N, Suwanachote S, Kulkollakarn S. Dihydroxyacetone: a safe camouflaging option in vitiligo. Int J Dermatol. 2008;47(4): 402- 6.
20. Levy SB. Tanning preparations. Dermatol Clin. 2000;18(4):591-6.
21. Goldman L, Wittgenstein E, Blaney D, Goldman J, Sawyer F. Studies of some physical properties of the dihydroxyacetone color complex. J Invest Dermatol. 1961;36: 233-4.
22. Lang KS, Caroli CC, Muhm A, Wernet D, Moris A, Schittek B, et al. HLA-A2 restricted, melanocyte-specific CD8 (+) T lymphocytes detected in vitiligo patients are related to disease activity and are predominantly directed against MelanA/MART1. J Invest Dermatol. 2001;116(6):891-7.
23. Ogg GS, Rod DP, Romero P, Chen JL, Cerundolo V. High frequency of skin-homing melanocyte-specific cytotoxic T lymphocytes in autoimmune vitiligo. J Exp Med. 1998;188(6):1203-8.
24. Taïeb A, Picardo M. Epidemiology, definitions and classification. In: Taïeb A, Picardo M, editors. Vitiligo. Berlin: Springer-Verlag; 2010. p. 13-24.
25. Kawalek AZ, James MS, Phelps RG. Combined Excimer Laser and Topical Tacrolimus for the Treatment of vitiligo: A Pilot Study. Dermatol Surg. 2004;30(2):130-5.
26. Chang RK, Raw A, Lionberger R, Yu L. Generic development of topical dermatologic products: formulation development, process development, and testing of topical dermatologic products. AAPS J. 2013;15(1):41-52.
27. Le Poole C, Boissy RE. Vitiligo. Semin Cutan Med Surg, 1997;16: 3-14.
28. Mahmoud, BH, Hexsel CL, Hamzavi IH. An update on new and emerging options for treatment of vitiligo. Skin therapy Lett. 2008;13(2):1-6.
29. Cornell TC, Stoughton RB. Correlation of the vasoconstriction assay and clinical activity in psoriasis. Arch Dermatol. l985;121(1): 6-3.
30. Onrust SV, Lamb HM. Mometasone Furoate. Adis Drug Evaluation. 1998;56(4):725-45.
31. Verdie P, Subra G, Feliu L, Sanchez P, Bergé G Gracin G, et al. On-Line Synthesis of Pseudopeptide Library Incorporating a Benzodiazepinone Turn Mimic: Biological Evaluation on MC1 Receptors. J Comb Chem. 2007;9(2):254-62.
32. Fesq H, Brockow K, Strom K, Mempel M, Ring J, Abeck D. Dihydroxyacetone in a new formulation - a powerful therapeutic option in vitiligo. Dermatology. 2001;203(3):241-3.
33. Levy SB. Dihydroxyacetone-containing sunless or self-tanning lotions. J Am Acad Dermatol. 1992;27(6 pt 1):989-93.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}