


Ludmilla Cardoso Gomes; Luisa Preisler; José Roberto Pereira Pegas
Received on: 07/04/2018
Approved on: 27/09/2018
This study was performed at the Complexo Hospitalar Padre Bento de Guarulhos – Guarulhos (SP), Brazil.
Financial support: None
Conflict of interests: None
Lesions located in fingers and toes, including the involvement of the nail apparatus, are not rare in dermatological practice. Many of them can be treated by dermatologist physicians qualified in dermatological and ungual surgeries, who rely on their knowledge of the origin and types, pathophysiology, and available therapeutic options for these lesions. The present study is aimed at presenting a bibliographical review on the various lesions that can affect this topography.
Keywords: Dermatologic surgical procedures; Fingers; Nail diseases
INTRODUCTION
Lesions located in fingers and toes deserve special attention in the dermatological examination, since the hands and feet are of great functionality for patients. 1 Dermatologist physicians who specialize in the field of dermatologic surgery can treat many of these lesions.2,3
Soft tissue tumors of the hands and feet can originate from the skin, subcutaneous tissue, tendons, nerves, and blood vessels. Their characteristics and severity of symptoms vary depending on the location, size and type of tumor, and many lesions can have various forms of clinical presentation.1,2 The nail apparatus can be affected by benign and malignant tumors, which in turn can be more common or rarer lesions.3
Viral warts, fungal or bacterial infections, subungual exostoses, glomus tumors, Koenen’s tumors, fibrokeratomas and onychomatricomas are examples of benign lesions.3 Only a small part of nail tumors is malignant, with the most frequently diagnosed lesions being squamous cell carcinoma1, 2, 3 and subungual melanoma – the latter being more feared due to its presenting aggressive behavior when diagnosis is delayed.
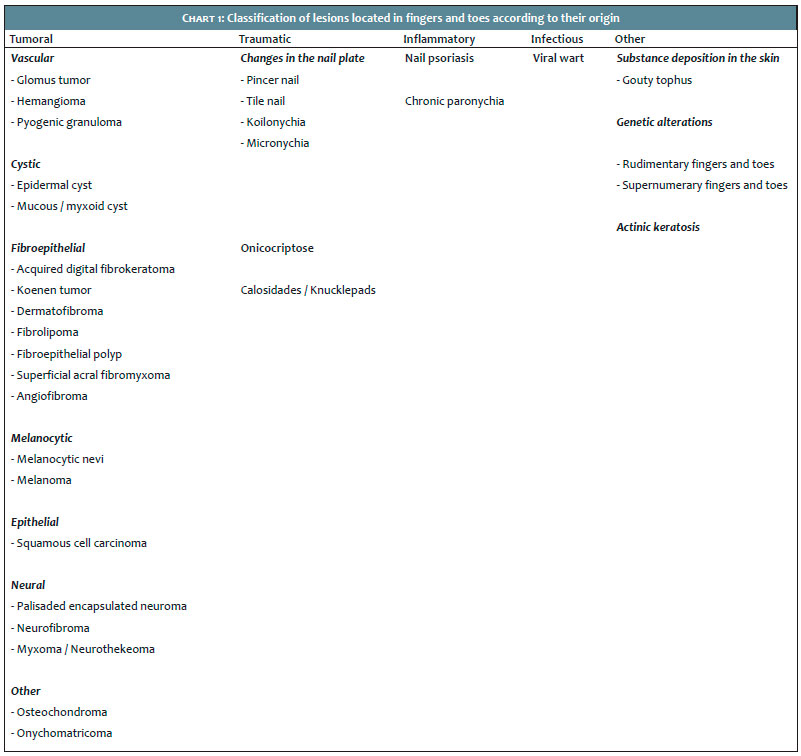
The purpose of the present study is to carry out a bibliographical review on lesions located in chirodactyls and pododactyls that are frequently observed in dermatological care, including those located in the nail apparatus and the therapeutic options available for each of them. Across the existing classifications, these lesions were grouped into: tumors, inflammatory, traumatic and infectious (Chart 1).
It is a benign vascular neoplasm of glomus cells that constitute a neuromyoarterial structure, with a regulating function of blood circulation and body temperature. It arises as an intensely painful subcutaneous tumor of slow growth.1,3-5 It is often observed as a single lesion in the distal phalanx of the fingers, corresponding to 1%-4.5% of the neoplasms of the hands, with a preference for the subungual region (Figure 1). In 80% of cases it occurs in the extremities, with higher frequency in the chirodactyls.2,5
Treatment consists of surgical excision, performed transungually, with a lateral incision, and Mohs micrographic surgery. New techniques, such as the modified lateral subperiosteal approach, which aims at preserving the nail plate, have been suggested.3-7
Characterized as benign neoplasms of vascular endothelial cells, it is often found in children, arising in the first weeks of life, rapidly growing in size and typically receding before the seventh year of life.8, 9 They are rarely located in fingers and toes. Superficial hemangiomas arise as well delimited reddish plaques, while the involvement of deeper tissues arises as a painful mass, and can be mistaken with malignant tumors. Complications include ulceration, bleeding, and infection. The conduct can be expectant in the case of small asymptomatic lesions. Progressive and symptomatic lesions can be treated with corticosteroids, beta-blockers (such as propranolol), and laser ablation. Surgical excision should be considered when the lesion develops with functional impairment, pain or accelerated growth.9
It is a benign tumor of vascular origin. (Figure 2) Relatively common, it often involves the nail bed and periungual tissues, as easily bleeding lesions.4,10 Its etiology is uncertain, however factors such as trauma,4.10 infections, drugs, sexual hormones associated with pregnancy, as well as angiogenic production of angiogenic growth factors, and overexpression of phosphorylated transcription factors – ATF2 and STAT3 – are related to their emergence. Histologic examination is crucial to exclude amelanotic melanoma.4 Treatment of pyogenic granuloma can be performed with high strength topical corticosteroids or surgical curettage under local anesthesia. When it leads to retronychia, surgery is the treatment of choice, with removal of the lesion from the ungual folds and avulsion of the nail plate. The lesion may also be associated with systemic inflammatory diseases, including sarcoidosis, psoriasis and seronegative spondyloarthritis, and treatment in these cases is difficult.
Myxoid cyst is a benign neoplasm of uncertain etiology, small in size, containing mucin in its interior. It is generally located in the interphalangeal region and may affect the nail matrix region, leaving depressions in the nail’s surface.11 Some authors consider it to be identical to the synovial cyst, however most believe that it results from a degenerative alteration of the connective tissue with consequent increase in the synthesis of hyaluronic acid. It affects middle-aged and elderly people, with a twice as large incidence in women as compared to men.4,11 In compressive dermoscopy, it appears as a translucent lesion,11 which confirms its cystic nature.4 There are several proposed treatments, such as drainage with destruction of its bed, transfixation of the cyst, aspiration and injection, cryotherapy and surgical removal.12
It is an acquired benign tumor of fibrous tissue that is usually located in the periungual area or in other parts of the fingers.4, 12, 13 Its first description dates back to 1968, by Bart et al.12 Trauma is considered as the major predisposing factor, yet its etiology is not elucidated. It arises as a single, smooth, asymptomatic fingerlike nodule, and may be sessile or pedunculated (Figure 3). A significant clinical differential sign is the presence of a collarette in the lesion’s base. It does not recedes spontaneously, being more frequent in adults.13 Diagnosis is histological in all cases, and is characterized by acanthosis and hyperkeratosis. The treatment of choice is surgical excision.4,13
They are benign periungual fibromas that develop in 50% of cases of tuberous sclerosis (epiloia or Burneville-Pringle disease).3,4 It usually arises between 12 and 14 years of age and progressively increases in size with the passing of the years. It may be asymptomatic or painful when larger.3 Generally multiple, it has globoid morphology. Ungual fibrokeratoma is its main differential diagnosis.3 Tumors grow from the ungual fold, and can destroy the nail bed when growth is exaggerated. When painful, requires surgical excision. Histological alterations correspond to dense angiofibrotic tissue, sometimes with central neuroglia tissue and hyperkeratosis in the extremity.4
It is the second most frequent fibro-histiocytic tumor of the skin. It is benign and arises as an isolated lesion in the extremities and trunk.14 Dermatofibromas located in the nail apparatus are rare and may resemble fibrokeratomas or supernumerary digits.4 Its histology reveals epidermal hyperplasia and hyperpigmentation of the basal layer. In the dermis, it is possible to observe a spindle-cell tumor.14, 15 Treatment of this lesion is often unnecessary, however surgical excision can be performed.14
It is a benign lipoma variant (Figure 4). It usually occurs as a subcutaneous solitary circumscribed lesion, composed of mature adipose tissue, fusiform cells with positive CD34, dense collagen strands, myxoid matrix and blood vessels.14 Treatment corresponds to surgical removal and the most important aspect of the histological differential diagnosis of this lipoma is the exclusion of liposarcoma.14
It is a benign and rare neoplasia, described in 2001 by Fetsch et al.16 It preferably affects the periungual or subungual regions.16, 17 It generally arises as a painless, slow-growing mass that mainly affects the extremities of the toes and fingers of adult men.17 Its histological analysis shows a poorly circumscribed lesion composed of fusiform or star-shaped neoplastic cells with varying degrees of pleomorphism, arranged in myxoid and collagenous stroma.16 These cells have immunoreactivity to CD34, CD99, and vimentin; and, focally, to epithelial membrane antigen (EMA).16 In most cases, the prognosis is benign, although there are reports of local recurrence in 22% of the cases.17 Since its histology may vary from tumor with mild cellular atypia to sharp nuclear atypia, with several mitosis figures in rare cases,16 the treatment of choice is complete surgical resection with free margins, due to the possible risk of malignant transformation.16, 17
They are formed by nevus cells that derive from stem cells originated in the dorsum of the neural crest, migrating to the epidermis and / or dermis during the embryonic development, and can be present in any region of the body (Figure 5). They can be congenital or acquired, and their removal should be performed when there is suspicion of malignancy, for aesthetic or psychological reasons.
It accounts for 4% of malignant cutaneous tumors, and is the most morbid and fatal skin cancer, although prevention and early diagnosis can assist in controlling the disease.14 Around 10% of melanoma cases are linked to family history of the disease, suggesting the existence of hereditary predisposition, usually associated with atypical nevi syndrome.14 They are clinically and histologically classified into superficial, nodular, acral lentiginous (which encompasses subungual melanoma), lentigo maligna melanoma, and other less frequent types, such as spitzoid melanoma, desmoplastic and neurotropic melanoma, and malignant blue nevus.14,15 Excisional biopsy is the best manner to diagnose melanomas.14 Surgical approach is the treatment of choice for the primary lesion, depending on its staging.14
The incidence of subungual melanoma is approximately 1% - 4% of all melanomas. In Negroids, the incidence is higher than in Caucasians, accounting for 15% - 20% of all melanomas in this group. It is more frequent in the hands than in the feet, with the hallux and thumb being the most affected. Striate melanonychia, Hutchinson’s sign and nail plate deformity are early signs of suspected subungual melanoma diagnosis, the diagnosis of which will be confirmed by histological examination. Ulceration, bleeding and loss of nail plate are late signs. Subungual melanoma’s differential diagnosis is clinically carried out with nevi, hematoma, paronychia, glomus tumor and pyogenic granuloma. Anatomopathology examination is crucial for diagnosis.3
In the nail apparatus, melanocytic lesions clinically arise as melanonychia, and can be due to focal activation of melanocytes, melanocyte hyperplasia, presence of melanocytic nevi or melanoma in the nail matrix.4
This is the second more frequent malignant skin tumor (21.7%).14 Bowen’s disease is an in situ carcinoma that can progress into invasive squamous cell carcinoma.3 When it is located in the nail apparatus, it can be also called epidermoid carcinoma, its malignancy is deemed as being of low degree.4 Incidence is higher in men between 60 and 70 years of age, and the thumb and the hallux are the most involved body sites. In most cases, this carcinoma begins in the lateral region of the nail as a circumscribed plaque with a verrucous surface that can lead to nail dystrophy. Trauma, chronic infection and exposure to chronic radiation are possible etiologic factors,4 as well as human papillomavirus (HPV) infection.3,4 Diagnosis is confirmed by anatomopathology and treatment is most often surgical.3
Also known as a solitary circumscribed neuroma, it is a neural tumor of the skin, unrelated to other neurofibromatosis stigmas.18 It was first described in a 1972 report of 44 cases by Reed et al., who termed it palisaded encapsulated neuroma of the skin.18,19 It is clinically characterized by slow growth and being mainly located in the face of men and women of 30 to 60 years of age.18 The typical lesion is a solitary, painless, non-pigmented sessile papule or papulonodule with a rigid and firm consistency. When pressed, it does not undergo herniation into the dermis, as observed in neurofibromas.18 Histologically, this neoplasm is circumscribed to the dermis and partially or completely surrounded by dense fibrous tissue forming a capsule.15, 18 The lesion consists of numerous fusiform fascicles of Schwann cells with eosinophilic cytoplasm, which are intensely stained by protein S100.18 The main differential diagnoses are: basal cell carcinoma, nodular chondrodermatitis of the helix, pyogenic granuloma, leiomyoma, chalazion, neurofibroma, seborrheic keratosis, actinic keratosis, cysts, sebaceous adenoma, trichofolliculoma, eccrine spiradenoma, facial fibrous papule, nevi and verruca vulgaris.18 Treatment is surgical, with removal of the lesion.20
Neurothekeoma or nerve sheath myxoma is a neural mesenchymal tumor characterized by the proliferation of nerve sheath cells in a variably myxomatous stroma.15,20 It is generally formed by asymptomatic lesions that are clinically mistaken with myxoid or ganglionic cysts, dermal melanocytic nevi, fibrolipomas, and adnexal neoplasias. Treatment is performed by excision of the lesion and, if removal is incomplete, the myxoma of the nerve sheath can recur.20
Neurofibroma is a benign tumor of neural origin, derived from Schwann cells, that can occur in any region of the body – including the skin – being infrequent in the hands.14,21 Clinically, solitary or multiple neurofibromas are tumors of solid consistency, semi globular or pedunculated, of normochromic or violet coloration. They can arise isolated or accompanied by syndromes, and neurofibromatosis may be present. They are in general symptomatic, however may present pruritus, pain and altered sensitivity to touch.14 Some authors report an incidence of 0.8% for neurofibromas in the hands.21 The excision of cutaneous tumors and the clinical or surgical treatment of lesions of other organs affected by the disease can be concomitantly performed.14 Surgery is indicated in cases of exaggerated tumor growth, pain and when malignant degeneration is suspected.21
It is a benign and rare tumor of the nail matrix.3,22 It is asymptomatic,3 yellowish in color and characterized by the thickening of the nail plate, with tubular formation and multiple dotted and irregular vessels.3,22-24 It can affect the hands’ and feet’s nails, without gender preference.22 The avulsion of the nails exposes a tumor and multiple projected filamentous digits originating from the nail matrix.3,23 Magnetic resonance is useful for its diagnosis,3 and its treatment corresponds to the complete excision of the tumor.3,24
Osteochondromas are benign neoplasms and is the most common osseous tumor of the foot (Figure 6), being found in the distal phalanges of the toes,25 most commonly in the hallux.4 The lesions arise as small elevations in the dorsal region of the distal phalange, and may emerge in the nail’s border, destroying its bed.26 Its prevalence is higher in men, and there is often a history of an associated trauma in the site. The triad of pain, deformity of the nail plate and radiographic features usually allows clear diagnosis. There is controversy about the fact of whether subungual exostosis and osteochondroma are different entities.4 Its treatment is surgical,4,26,27 aiming at resolving the pain or functional incapacity, caused either by neurovascular compression or by limitation of the joint movement.26
There are three main types of transverse curvature of the nail plate: the pincer nail; the tile nail; and the plicatured nail.4 The causes can be hereditary or acquired. Toes are affected more frequently. Conservative treatments are preferred by patients, however surgical treatments lead to the best outcomes and should be carried out when the lesion causes pain, inflammation, impossibility to use of closed shoes, or aesthetic embarrassment.28
• Pincer nail
It is characterized by a transverse hypercurvature that increases along the axis, in the proximal to distal direction.4,28 Pain is not very intense in general, however it can be sometimes severe.4 The definitive procedure is surgical treatment using the Haneke technique.4, 27
• Tile nail
The nail in the shape of a tile has an increased transverse curvature, however the lateral margins remain parallel to each other.4,28
• Plicatured nail
It presents moderate convexity in one or both sides of the lateral margins, which abruptly alter their angulation and sharply penetrate the sides of the nail bed.4,28
• Koilonychia
Refers to the concavity of the nail, which assumes the shape of a “spoon”. The nail plate is firmly attached to the bone by vertical bundles of subungual region’s connective tissue, which connect directly to the periosteum.4
It occurs due to the penetration of the nail plate – in varying degrees – in the periungual soft tissues.4,27 It can be caused by hypertrophied nail folds, altered curvature or distal insertion of the nail plate.4 The use of tight shoes that cause excessive external pressure, inadequate nail trimming and traumas are factors that lead to onychocryptosis. Several techniques of treatment are mentioned, with evidence that the nail matrix phenolization technique is efficient in several degrees of onychocryptosis, with a minimally painful post-operative and rapid return to daily activities, often dismissing the necessity of matrix curettage.29 Hypertrophy of the lateral folds usually accompanies chronic ungual deformities in the pododactyls. The nail appears to be normal or slightly involuted, however there is an increase in soft tissue, which overlaps the nail plate. Bone deformities, such as hallux valgus and hallux rigidus, favor hypertrophy of the nail folds in the first toes.4 In regions of impact, silicone protectors can be used in the interdigital space. Treatment corresponds to reducing the excess of periungual soft tissue, with several surgical techniques described.4,14,27
Interphalangeal or knuckle pads are hyperkeratotic nodules, rough on the surface, slightly brownish or grayish, of about one centimeter in diameter, usually rounded, hardened, with precise limits and regular contours. They are asymptomatic lesions with chronic development, most frequently located in the proximal interphalangeal and matacarpophalangial joints. Histology evidences hyperkeratosis, acanthosis and prolongation of the papillary crests. The treatment corresponds to the reduction of the friction in the joints, while surgical removal and intralesional injection of corticosteroids is quoted to reduce the lesion.30
Psoriasis is a chronic inflammatory cutaneous disease of a recurrent character.31 Despite its aesthetic and functional implication, psoriasis nail involvement is an aspect of the disease that has not yet been adequately studied, which is reflected in the limited number of studies on its epidemiology and clinical features. 31 Alterations compatible with ungual psoriasis can also be seen in the absence of the disease, which occurs in only one to 5% of patients.31,32
The effect of psoriasis on the ungual matrix leads to changes in the nail plate, such as cupuliform depressions (pittings), leukonychia, reddish spots in the lunula, and fragmentation of the nail plate (crumbling). On the other hand, the involvement of the nail bed causes an onycholysis, oil or salmon spots, dyschromia, splinter hemorrhages and nail bed hyperkeratosis.4, 31, 32 Psoriasis of the periungual tissues is similar to psoriasis of the dorsum of fingers and is considered to be a cutaneous extension of the involvement of the fingers.32
It is an inflammatory disease that lasts longer than six weeks and involves one or more nail folds (lateral and proximal). It corresponds to 18% of the nail dystrophies, with a higher prevalence in women. Chronic paronychia is based on the inflammatory process and possible infections are deemed as secondary. Clinically, there is inflammation of the proximal nail fold (PNF), absence of cuticle, and nail plate dystrophy.33 The inflammation of the toes’ nail folds is common in athletes, being characterized by edema, erythema, pain, and purulent secretion. It is often caused by the pressure of the shoes, and the hallux is most frequently affected.4 Clinical treatment consists of avoiding predisposing factors and the use of topical and / or systemic drugs, nevertheless results are often unsatisfactory.4,33 Surgery is indicated in cases that are resistant to clinical treatment and is aimed at removing the proximal nail fold. In 1981, Baran and Burean described the technique of bloc excision of the proximal nail fold – or technique with perpendicular incision. The second technique, described in 1976 by Keyser and Eaton, consists of removal of the dorsal surface of the proximal nail fold, leaving the ventral portion of the fold untouched, without removing the nail plate or oblique exeresis of the proximal nail fold (OEPNF).33
They are benign, weakly infectious tumors,1 caused by the human papillomavirus (HPV) that are characterized by a yellow-opaque hyperkeratotic surface.1,14 Verruca vulgaris accounts for roughly 70% of all cutaneous warts, and arise as keratotic papules with hard and rough surface, sometimes with black spots (on the surface), which correspond to thrombosed capillaries. They are usually located on the dorsum of the hands and feet, in the periungual folds, elbows and knees.14 Subungual warts initially affect the hyponychium, slowly growing towards the nail bed, finally raising the nail plate. Bone erosion occurs occasionally with verruca vulgaris.1 There is great diversity in treatments for viral warts – from chemical treatment that employ acids locally to surgical procedures, such as cryosurgery, electrocoagulation with or without curettage, CO2 laser, photodynamic therapy.14
There are a number of other lesions that have not been included in the present review that may appear in fingers and toes, including actinic keratosis, gouty tophus, and supernumerary / rudimentary fingers.
Actinic keratosis is a cutaneous neoplasm caused by the proliferation of cytologically aberrant epidermal keratinocytes in response to prolonged exposure to ultraviolet radiation.14 They are erythematous-squamous lesions of rough texture that emerge in photoexposed sites of the skin.1,14 There may be a malignant transformation into squamous cell carcinoma (SCC), manifesting with infiltration, hyperkeratosis, inflammation, ulceration, recurrence or sudden change in growth.1 Histology differentiates it from SCC.14
Gouty tophus is a lesion typical of gout, which is an inflammatory disease where there is deposition of sodium monourate.14 Gouty tophi can occur in several body sites, sometimes mimicking infectious or neoplastic pathologies. Surgical removal is associated with the possibility of complications, which may result from the difficulty of extracting tightly adhered tophi. However, surgery must be considered in cases of infection, ulceration or intense local pain, as well as for aesthetic reasons.34
Rudimentary or supernumerary fingers are usually isolated congenital deformities, more commonly observed in the ulnar (post-axial) region, implanted in the medial region of the fifth fingers. The supernumerary finger corresponds to a true duplication, whereas a rudimentary bud is an incomplete form of the condition, which can necrose and detach painlessly after birth. In the majority of cases, simple resection of the supernumerary finger is sufficient as a treatment.35
Knowledge of the lesions that manifest in fingers and toes undoubtedly has great importance in the dermatologist physician’s routine. It is therefore crucial that the diverse diagnostic possibilities of these lesions be considered in the dermatological evaluation – either in the case of an isolated presentation or as part of a systemic disease. In this manner, the dermatologist will adopt a better approach aimed at offering the most appropriate treatment, which will result in a better aesthetic and functional outcome for the patient.
Ludmilla Cardoso Gomes | ORCID 0000-0002-8165-5345
Conception and planning of the study; structuring and drafting of the manuscript; collection, analysis and interpretation of data; approval of the manuscript
Luisa Preisler | ORCID 0000-0002-1600-9953
Conception and planning of the study; structuring and drafting of the manuscript; collection, analysis and interpretation of data; approval of the manuscript
José Roberto Pereira Pegas | ORCID 0000-0002-2541-6008
Conception and planning of the study; review and approval of the final version of the manuscript
1. Sobanko JF, Dagum AB, Joseph FS, Davis IC, Kriegel DA. Soft Tissue Tumors of the Hand. 1. Benign. Dermatol Surg. 2007;33(7):651-67.
2. Sobanko JF, Dagum AB, Joseph FS, Davis IC, Kriegel DA. Soft Tissue Tumors of the Hand. 2. Malignant. Dermatol Surg. 2007;33(7):771-85.
3. Quintella MGM, Rosa IP, Michalany NS, Bilemjiam A, Hirata SH, Enokihara MY, et al. Tumores comuns e raros do aparelho ungueal. RBM rev bras med. 2009; 66 supl.3:12-4.
4. Baran R, Dawber RPR, Tosti A, Haneke E. A Text Atlas of Nail Disorders - Techniques in investigation and diagnosis. 3rd edition. London: Mosby; 2003.
5. Vanti AA, Cucé LC, Chiacchio ND. Subungual glomus tumor: epidemiological and retrospective study, from 1991 to 2003. An Bras Dermatol. 2007;82(5):425-31.
6. Grover C, Khurana A, Jain R, Rathi V. Transungual surgical excision of subungual glomus tumour. J Cutan Aesthet Surg. 2013;6(4):196-203.
7. Garg B, Machhindra MV, Tiwari V, Shankar V, Kotwal P. Nail-preserving modified lateral subperiosteal approach for subungual glomus tumour: a novel surgical approach. Musculoskelet Surg. 2016;100 (1):43-8.
8. Valentini JD, Aguiar DF, Ferdinando MPL, Wagner M, Silva JB. Hand tumors – Part I: Soft tissue tumors. Rev AMRIGS. 2015;59 (3):237-42.
9. Henderson MM, Neumeister MW, Bueno RA Jr. Hand tumors: I. skin and soft-tissue tumors of the hand. Plast Reconstr Surg. 2014;133(2):154e-64e.
10. Piraccini BM, Bellavista S, Misciali C, Tosti A, de Berker D, Richert B. Periungual and subungual pyogenic granuloma. Br J Dermatol. 2010;163(5):941-53.
11. De Castro CGC, Amorim BDB, Gomes LA, Steffan MS, Vilhena LAP, Plata G. Cisto mixóide simulando melanoma amelanótico: relato de caso. RBM rev bras med. 2016;72(esp G3):22-5.
12. Bart RS, Andrade R, Kopf AW, Leider M. Acquired digital fibrokeratomas. Arch Dermatol. 1968;97(2):120-9.
13. Pegas JR, Cade KV, Kiyomura MY, Sousa AS, Bazzo ILMS, Tebcherani AJ. Acquired digital fibrokeratoma: report on a clinical case of a clinical case. Surg Cosmet Dermatol. 2012;4(4):357-9.
14. Belda Júnior W, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 2nd ed. São Paulo: Ed. Atheneu; 2015.
15. Rapini, Ronald P. Dermatopatologia Prática. 2nd ed. Rio de Janeiro: Elsevier; 2013.
16. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma: a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes. Hum Pathol. 2001;32(7):704-14.
17. Souza BGS, Lisboa TP, Barbosa VAK, Almeida JPS, Bacchi CE, Souza VG. Superficial Acral Fibromyxoma of the Thumb: a case report. Rev Bras Ortop. 2013;48(2):200-3.
18. Ravelli FN, Oliveira Filho J, Michalany NS, Afonso IAP, Franchin TB, Macedo ACL. Case report: Palisaded encapsulated neuroma simulating a Basal Cell Carcinoma. Surg Cosmet Dermatol. 2013;5(2):177-9.
19. Reed RJ, Fine RM, Meltzer HD. Palisaded, encapsulated neuromas of the skin. Arch Dermatol. 1972;106(6):865-70.
20. Bolognia J, Jorizzo J, Rapini RP. Dermatology. 3rd edition. London: Ed. Mosby; 2015.
21. Batista KT, Araújo HJ, Paz Júnior AC. Plexiform neurofibroma of the upper extremity. Rev Bras Cir Plást. 2011;26(3):546-9.
22. Piraccini BM, Antonucci A, Rech G, Starace M, Mischiali C, Tosti A. Onychomatricoma: first description in a child. Pediatr Dermatol. 2007;24(1):46-8.
23. Baran R, Kint A. Onychomatrixoma: filamentous tufted tumour in the matrix of a funnel-shaped nail: a new entity (report of three cases). Br J Dermatol. 1992;126(5): 510-5.
24. Haneke E, Franken J. Onychomatricoma. Dermatol Surg. 1995;21(11):984-7.
25. Subungual Osteochondroma or Exostosis Cartilaginea of the Hallux: A case report of recurrent bone tumor one year later. The Foot and Ankle Online Journal. 2010;3(2):2.
26. De Souza AMG, Bispo Junior RZ. Osteocondroma: ignorar ou investigar? Rev bras ortop. 2014;49(6):555-64.
27. Chiacchio NG, Ferreira FR, Mandelbaum SH, Di Chiacchio N, Haneke E. Nail Surgery: follow-up on cases conducted during a practical course of a Dermatological Meeting. Surg Cosmet Dermatol. 2013;5(2):134-6.
28. Tassara G, Machado-Pinto J, Gualberto GV, Ribeiro BS. Treatment of pincer nail utilizing Zook’s technique: report of 5 cases. An Bras Dermatol. 2008;83(3):237-41.
29. Tassara G, Machado MA, Gouthier MAD. Treatment of ingrown nail: comparison of recurrence rates between the nail matrix phenolization classical technique and phenolization associated with nail matrix curettage - is the association necessary? An Bras Dermatol. 2011;86(5):1046-8.
30. Pereira JM, Pereira FCN, Pereira VCN. Interphalangeal pads on pachydermodactyly. An Bras Dermatol. 2004;79(3):313-21.
31. Schons KRR, Knob CF, Murussi N, Beber AAC, Neumaier W, Monticielo OA. Nail psoriasis: a review of the literature. An Bras Dermatol. 2014;89(2):317-22.
32. Tan ES, Chong WS, Tey HL. Nail Psoriasis: A Review. Am J Clin Dermatol. 2012;13(6):375-88.
33. Di Chiacchio N, Debs EAF, Tassara G. Surgical treatment of chronic paronychia: a comparative study of 138 surgeries using two different techniques. Surg Cosmet Dermatol. 2009;1(1):21-4.
34. Coutinho M, Barcelos A. Tofo gotoso de localização atípica em doente com múltiplos todos gotosos infectados. Acta Reumatol Port. 2010;35(2):271-2.
35. França Bisneto EN. Deformidades congênitas dos membros superiores. Parte II: falhas de formação e duplicação. Rev Bras Ortop. 2013;48(1):3-10.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}