


Frederico Hassin Sanchez1; Timótio Volnei Dorn2
Received on: 13/09/2017
Approved on: 07/03/2018
This study was conducted at the EpiOne Centro de Ensino e Pesquisa - Chapecó (SC), Brazil.
Financial support: None
Conflict of interests: None
There are many procedures for the rejuvenation of the cervical region. Nevertheless, the most invasive ones – such as the rhytidectomy – can lead to relatively large unaesthetic scars. In contrast, noninvasive procedures – such as the classic absorbable lifting threads – have no significant effect on the treatment of the most evident platysmal bands. Aiming at solving the problem of short durability linked to the lifting threads and eliminating the undesirable submental scar caused by rhytidoplasty, a less invasive technique is described for the treatment of cervical laxity. This technique can be used isolatedly in patients with small amounts of skin redundancy, or associated to mini face lifts in patients with considerable sagginess.
Keywords: Cosmetic techniques; Dermatologic surgical procedures; Esthetics; Lifting; Mandible; Neck muscles; Rejuvenation; Rhytidoplasty
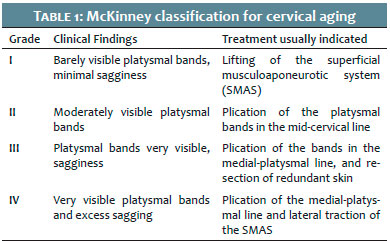
Bone resorption, combined with sagging, determines the unsightly appearance of the cervical region.1,2 Over time, there is loss of the mandibular contour and accumulation of submentonian fat, with a consequent increase in the cervical-mentonian angle, muscular hypotonia, prominence of platysmal bands, ptosis of the submandibular glands, and changes in texture and pigmentation due to photoexposure.1,2 There are several classification systems aimed at quantifying the severity of cervical aging, including the McKinney’s (Table 1).3
Although cervical lifting techniques have gone through remarkable advance, the stigma caused by visible scars or the appearance of “stretched face”, causes many patients to seek alternative techniques to rhytidectomy.2,4,5
Minilifting and its variations are considered very effective treatments, nevertheless very invasive. Most recently, suspension threads have popularized the treatment of this region.5,6 Polylactic acid or polydioxanone support threads are generally absorbable and are pledged to cause a skin lift effect, and promote collagen stimulation.7-9 However, they are not usually anchored to any bone structure, entailing that their lifting effect is limited and ephemeral. In contrast, rhytidoplasty has a lasting effect; nonetheless, it results in an undesirable scar (measuring 3 to 5 cm) in the submental region, necessary for the plication of the platysmal bands.4
In order to solve the problem of the little durability linked to the suspension threads and the undesirable submental scar caused by rhytidectomy, one of the authors of the present paper has developed a technique for treating cervical laxity, aimed at providing greater durability with minimal visible scarring.
The objective of the present study is to describe a minimally invasive technique for treating cervical laxity, termed transmastoid support (TMS) by the authors.
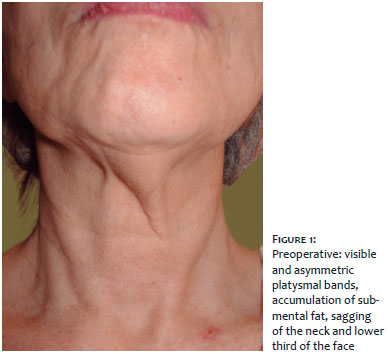
Lean female patients with prominent platysmal bands and loss of mandible angle definition (McKinney grade II and III) are the ones that benefit most from this technique. Patients with a large accumulation of submental fat may require extensive liposuction of the submental area, and if there is a large amount of skin sagginess (of McKinney grade IV), association with mini lifting should be considered (Figures 1 and 2).
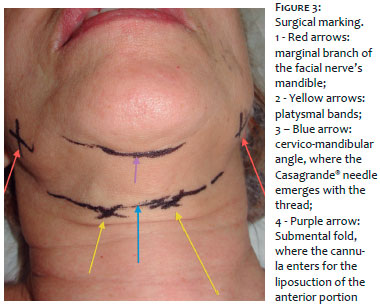
After the cleansing of the skin, surgical marking is performed with the patient in sitting position, and the head rectified in an anatomical position so that the central point of the cervical-mental angle, as well as the area to be lipoaspirated, can be identified and marked (Figure 3). Next, injection of tumescent anesthetic solution with 0.5% lidocaine and 1/100,000 adrenaline is performed.
1) Incision with n. 11 blade, enough for the passage of the 2mm liposuction cannula, bilaterally in the retroauricular region, in the mastoid bone’s topography
2) Incision with n. 11 blade in the submental fold for the passage of the cannula
3) Tumescent liposuction is performed in the submental region according to each patient’s need. For patients who do not have significant accumulation of fat in this region, liposuction is aimed at effecting a blunt dissection, partially detaching the skin, facilitating the passage of the thread
4) The retroauricular excisions are enlarged up until the mastoid bone’s periosteum, bilaterally
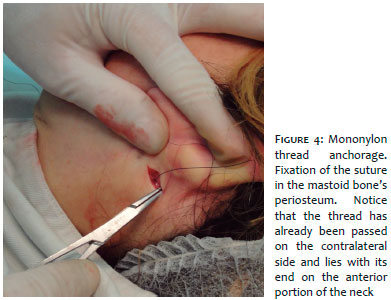
5) Two 3.0 mononylon sutures are respectively attached to the mastoid bone’s periosteum on each side (Figure 4)
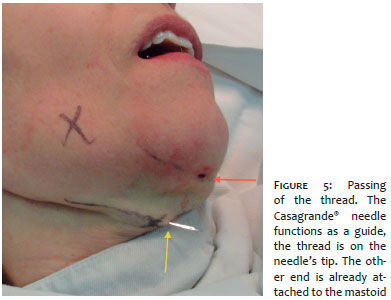
6) After the fixation of the thread in the periosteum, the circular needle is discarded. The free end of the thread is passed through a small hole in the Casagrande needle, which is then introduced by the incision in the retroauricular region, passing along the mandibular contour, in the direction of the cervical-mental angle. A small incision performed with a n. 11 blade in the center of this angle is sufficient to allow exiting with a Casagrande® needle and the suture. The process is repeated on the contralateral side (Figure 5).
7) The threads meet in the ventral region of the neck, in the incision carried out in the center of the cervical-mental angle. A surgical knot is performed in order to join and pull the two ends of the thread up until the point the desired retraction of the platysmal bands is achieved. Next, the tie/knot is placed into the incision so that it does not remain visible (Figure 6).
8) Surgical closure of skin incisions. Some patients with a great volume of sagginess will experience skin redundancy in the pre-auricular region after the threads have been tractionned. This should be corrected with the assistance of miniliftings, which will position the scars in the pre and post-auricular regions.
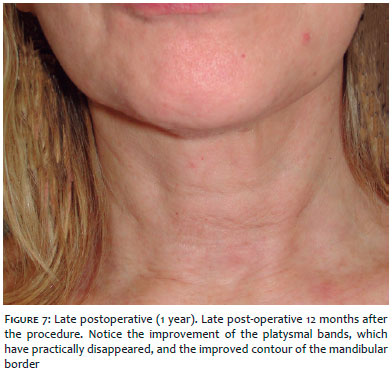
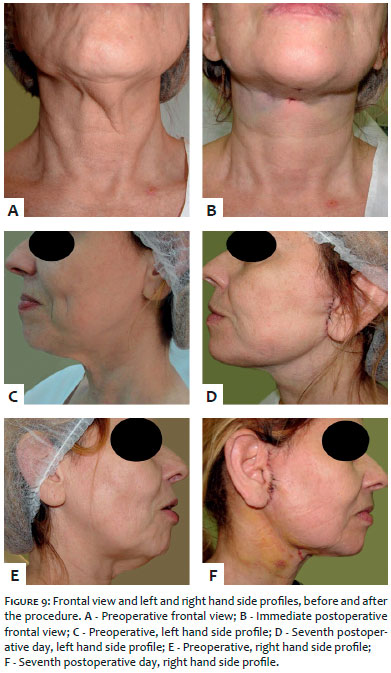
The outcome can be seen immediately after the procedure. In the case described, it was necessary to remove the redundant skin in the pre-auricular region after the threads were tractionned (Figures 7 and 8). The obtained effect was long lasting, with great improvement of cervical sagginess and devoid of complications. In the postoperative period it was already possible to notice improvement in the neck’s and mandible’s contours (Figure 9).
A younger silhouette is characterized by well-defined cervical-mandibular and mandible branch contours, cervical-mental angle of roughly 90º, little local sagging and adiposity.
Knowledge of the anatomy allows greater precision in the treatment of the senile neck, reducing the incidence of postoperative complications. Beneath of the dermis are the subcutaneous fat and the superficial cervical fascia, which is intimately connected with the platysma muscle to the SMAS. The TMS technique is carried out in the plane located between the superficial cervical fascia and the dermis, with the suction of the submental fat and subcutaneous fat from the lateral aspect of the neck, with the subsequent pass of the support thread in the described plane.
The facial nerve mandible’s marginal branch deserves close attention. It is located beneath the platysma, along the mandible’s body (in 80% of cases) – or 2cm below – surfacing on the anterior border of the masseter muscle. If injured, paralysis of the depressor muscles of the angle of the mouth and lower lip may occur, causing asymmetry during the smile.10,11
For patients affected by micrognathism, surgical mentoplasty or filling procedures may be associated with the TMS technique. Exaggeratedly prominent platysmal bands and redundant skin (classified as McKinney degree IV) may require associated minilifting. Special attention should be given to extremely thin women, in whom the lift effect caused by the TMS technique may anteriorize and project the thyroid’s cartilage, lending a masculinized appearance to the neck.2,12
Several types of thread have already been used in cervical rejuvenation, among them, polypropylene, spiculated polypropylene, spiculated mononylon among others. Giampapa and Di Bernardo were pre-cursors in the use of threads for cervical support as an alternative to traditional rhytidectomy.13 Later on, the use of spiculated polypropylene threads became popular (with a technique known as “Russian thread”).9 More recently, a new technique was published employing a colorless modified spiculated 2.0 mononylon, specifically developed for the cervical lift, being marketed under the commercial name I-lift ®. It is introduced with an 18G epidural 18cm needle, and may be an alternative in cervical treatment.14
The authors deem the TMS technique as a good option due to the fact it does not requiring a specific thread, being carried out with a simple 3.0 mononylon suture thread. In addition to its low cost, it is easy to perform, and does not cause extensive submental scars.
The technique can directly address the main factors involved in cervical aging: the accumulation of submental fat and the sagging of the platysma muscle.
Frederico H. Sanchez | ORCID 0000-0001-5856-216x
Responsible for the photographic records, guidance and review of the article.
Timotio Volnei Dorn | ORCID 0000-0001-9666-6146
Responsible for the literature review, and writing of the article.
1. Roy S, Buckingham E. The Difficult Neck in Facelifting. Facial Plast Surg. 2017;33(3):271-78.
2. Patel BC. Aesthetic surgery of the aging neck: options and techniques. Orbit. 2006;25(4):327-56
3. McKinney P. The management of platysma bands. Plast Reconstr Surg. 1996;98(6):999-1006.
4. Kim BJ, Choi, JH, Lee Y. Development of facial rejuvenation procedures: thirty years of clinical experience with face lifts. Arch Plast Surg. 2015; 42(5):521-31.
5. Stephenson KL. The "mini-lift": an old wrinkle in face lifting. Plast Reconstr Surg. 1970;46(3):226-35.
6. Mulholland RS. Nonexcisional, minimally invasive rejuvenation of the neck. Clin Plast Surg. 2014;41(1):11-31.
7. Savoia A, Accardo C, Vannini F, Di Pasquale B, Baldi A. Outcomes in thread lift for facial rejuvenation: a study performed with happy lifttm revitalizing. Dermatol Ther(Heidelb). 2014;4(1):103-114.
8. Khrustaleva I, Khrustaleva G, Borovikova A, Tamarov A, Borovikov A. Our technique of thread lifting for facial rejuvenation. Plast Reconstr Surg Glob Open. 2016;4(6):e739.
9. Sulamanidze M, Sulamanidze G. Facial lifting with Aptos methods. J Cutan Aesth Surg. 2008;1(1):7-11.
10. Daane SP, Owsley JQ. Incidence of cervical branch injury with "marginal mandibular nerve pseudo-paralysis" in patients undergoing face lift. Plast Reconstr Surg. 2003;111(7):2414-8.
11. Batniji RK. Complications/sequelae of neck rejuvenation. Facial Plast Surg Clin North Am. 2014;22(2):317-20.
12. Tavares JP, Oliveira CACP, Torres RP, Bahmad Junior F. Facial thread lifting with suture suspension. Braz J Otorhinolaryngol. 2017; 83(6):712-19.
13. Giampapa VC, Di Bernardo BE. Neck recontouring with suture suspension and liposuction: an alterna- tive for the early rhytidectomy candidate. Aesthetic Plast Surg 1995;19(3):217-23.
14. De Carolis V, Gonzalez M. Neck rejuvenation with mastoid-spanning barbed tensor threads (MST operation). Aesthetic Plast Surg. 2014; 38(3):491-500.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}