


Gisele Gargantini Rezze1; Maurício Mendonça Nascimento2; Regiane Salera1; Clóvis Antonio Lopes Pinto3; Francisco Macedo Paschoal1,4
Received on: 23/01/2018
Approved on: 02/03/2018
This study was conducted at the Dermaimage Médicos Associados - São Paulo (SP), Brazil.
Financial Support: None
Conflict of Interests: None
The diagnosis of pigmented facial lesions is considered challenging since benign and malignant lesions might have similar clinical and dermoscopic features – especially in the early stages of the lesion – entailing that it is often difficult to identify lentigo maligna lesions in the face. In this way, confocal reflectance microscopy has the potential to become a useful tool both in the diagnosis and surgical planning of lentigo maligna.
Keywords: Dermoscopy; Hutchinson's melanotic freckle; Keratosis, actinic; Melanoma; Microscopy, confocal
Lentigo maligna (LM) is a form of in situ melanoma that occurs in photodamaged skin of elderly patients. Due to the fact it most often arises as a facial pigmented lesion, its clinical diagnosis is challenging, for it may resemble benign pigmented lesions.1
Facial dermoscopy presents some peculiarities linked to this anatomical area. It is a region with intense exposure to ultraviolet radiation, which causes a certain degree of epidermal atrophy, solar elastosis and epithelial cones rectification, leading to the absence of pigmentary networks (used to classify lesions as melanocytic or non- melanocytic in other regions of the skin) and presence of the so-called pseudo network. The latter is formed by the interruption of the melanin pigment in the follicular ostia and the presence of adnexal structures in melanocytic and non- melanocytic lesions of the face.2,3
In 2000, Schiffner et al.2 proposed a dermoscopic diagnostic model for LM lesions and lentigo maligna melanoma (LMM) with 93% accuracy, 89% sensitivity and 96% specificity. According to these authors, the dermoscopic features corresponding to the combination of grayish spots and globules, dark rhomboidal structures and asymmetric pigmentation of the follicular ostia are the most commonly observed in these lesions and correlate with the histological characteristics typical of this type of melanoma – folliculotropism in particular.2
Although the dermoscopic findings described for the diagnosis of LM have a high degree of accuracy, differential diagnosis with pigmented actinic keratosis (PAK) is still challenging, since these latter may present some of the dermoscopic characteristics typical of LM. Only black blotches are specific for the diagnosis of LM, however their occurrence is delayed, rarely emerging in early lesions.3
In this context, Nascimento et al. described a new relevant dermoscopic feature, the inner gray halo (IGH), whose presence proved to be considerably effective in differentiating LM from PAK. The presence of three or more of these new structures (IGH) would characterize a PAK, with a 91.4% sensitivity, 71.4% specificity and positive predictive value of 89.8%. The IGH’s histological substrate would correspond to the umbrella pattern described by Pinkus.4
Dermoscopy has particular limitations in incipient pigmented lesions of the face, and confocal microscopy becomes a promising test in when considering a greater degree of diagnostic reliability.1
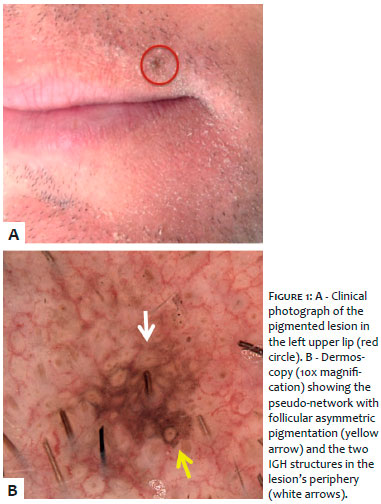
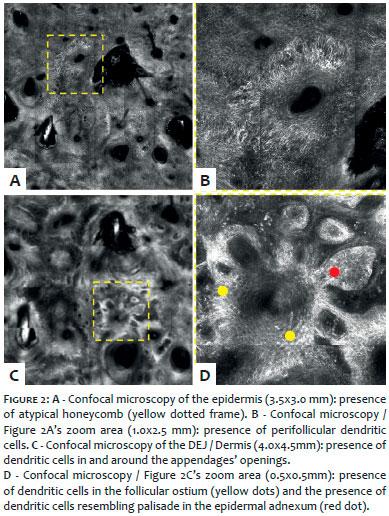
A 42-year-old male patient, Fitzpatrick’s type II skin, with light brown hair and eyes, with history of sunburn in childhood and adolescence, family history of cutaneous melanoma (father and paternal grandfather, confirmed by histological examination) and personal background of surgically excised atypical nevi, with histological confirmation. In the fifth assessment follow-up (total body mapping and digital dermoscopy examination due to multiple melanocytic nevi), the patient presented a new pigmented lesion on the upper left lip, measuring roughly 3mm in diameter (Figure 1A). The dermoscopic examination evidenced a lesion with brownish pseudo network with a discrete area containing an annular-granular pattern, asymmetric pigmentation in the follicular openings, and two structures compatible with peripheral IGH (Figure 1B). The diagnostic hypotheses of PAK and LM were considered. A confocal microscopy examination showed the presence of bright dendritic cells in large numbers in the epidermis with absence of buds due to typical epidermal rectification of the face. Also, it evidenced the presence of bright dendritic cells around and in the adnexal openings in the dermal-epidermal junction (DEJ), as well as bright dendritic cells in the epidermal appendages in the papillary dermis (Figure 2).
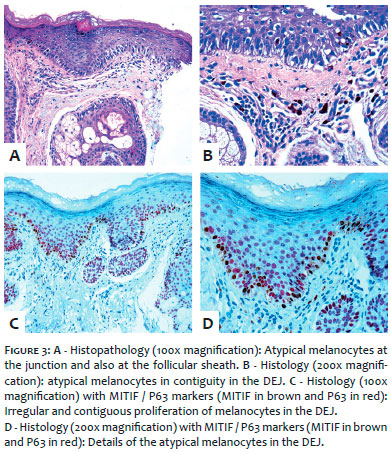
Based on the clinical and dermoscopic findings, in addition to those obtained from confocal microscopy, the diagnostic hypothesis of LM in a photodamaged area was established. Histological examination (H&E) of the excisional biopsy suggested the presence of atypical melanocytic proliferation in the junctional layer of the epidermis, extending up until the follicular infundibulum. Atypical melanocytes had epithelioid and fusiform patterns. The nuclei were hyperchromatic, and sometimes multilobular. The melanocytes were distributed continuously and contiguously. Some cells were arranged perpendicular to the epidermis. The cytoplasm had a variable amount of moderate to intense melanin pigment. There were scarce atypical mitoses in junctional melanocytes. There was no proliferation of melanocytes in the dermis, but only melanophages in the papillary dermis. Some dendritic cell clusters with mitotic figures and atypical multinucleated melanocytes were present at the dermo-epidermal junction and adjacent follicular sheath (Figures 3A and 3B). The immunohistochemical study with double expression of MITF1 / P63 antibodies demonstrated the presence of lentiginous proliferation of atypical melanocytes in the basal layer of the epidermis. The melanocytes’ nuclei stain the antibody MITF1 in brown while the keratinocytes’ nuclei stain the antibody P63 in red (Figures 3C and 3D).
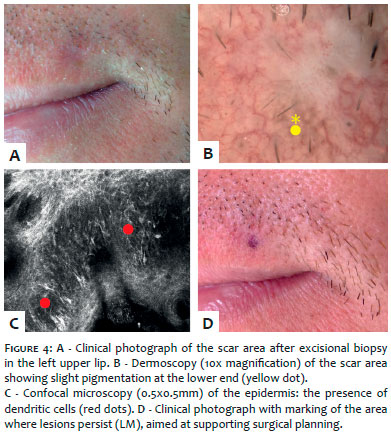
Fifteen days after the biopsy was carried out, a new confocal microscopy examination was performed aimed at refining the surgical planning (to decrease the chance of local recurrence and achieve better esthetical results), and evidenced the persistence of the lesion in one of the scar’s margins (Figure 4).
Confocal microscopy is useful in the early diagnosis of LM and LMM. Although these entities are cellularly different in nature from PAK, differential diagnosis between them is sometimes difficult, from both the clinical and the dermoscopic points of view. In this context, confocal microscopy can be of great help in the diagnostic definition.5
The finding related to bright dendritic cells invading the follicular ostium strongly suggests the diagnosis of LM and corresponds to the asymmetrically pigmented follicular openings observed in dermoscopy. Although these cells located within the follicle can be mistaken with the basal cell carcinoma’s palisade in the dermoepidermal junction, images of the stratum spinosum are key to the diagnosis with the presence of large numbers of dendritic cells.
The dermoscopic findings of the IGH structures can be explained by the presence of small bright cells that do not invade the follicles at the lesion’s periphery, which in tandem with the atypical honeycomb arrangement, and the presence of photodamage, suggest the diagnosis of PAK. According to the histopathology described by Pinkus, non-invasion by tumor cells of the perifollicular epithelium in actinic keratosis is a possible correlation model with dermoscopy and with confocal microscopy, and may be an supporting factor in the differential diagnosis with LM.4
In this clinical case, confocal microscopy was important not only for elucidating the clinical diagnosis – which was confirmed by histology – but also for being significantly useful in the surgical planning, identifying the lesion’s presence in the margins of the excisional biopsy.
Gisele Gargantini Rezze | ORCID 0000-0001-9084-4634
Design, preparation and writing of the manuscript. Collection, analysis and interpretation of the data. Intellectual participation in the propaedeutic and therapeutic approach of the case. Approval of the final version of the manuscript.
Maurício Mendonça do Nascimento | ORCID 0000-0003-0060-8473
Design, preparation and writing of the manuscript. Approval of the final version of the manuscript.
Regiane Salera | ORCID 0000-0002-2961-1361
Collection, analysis and interpretation of the data.
Clóvis Antonio Lopes Pinto | ORCID 0000-0003-1711-0081
Design, preparation and writing of the manuscript. Collection, analysis and interpretation of the data.
Francisco Macedo Paschoal | ORCID 0000-0002-6264-1538
Intellectual participation in the propaedeutic and therapeutic approach of the case. Approval of the final version of the manuscript.
1. Guitera P, Pellacani G, Crotty KA, Scolyer RA, Li LX, Bassoli S, et al. The impact of in vivo reflectance confocal microscopy on the diagnostic accuracy of lentigo maligna and equivocal pigmented and nonpigmented macules of the face. J Invest Dermatol. 2010; 130(8):2080-91.
2. Schiffner R, Schiffner-Rohe J, Vogt T, Landthaler M, Wlotzke U, Cognetta AB, et al. Improvement of early recognition of lentigo maligna using dermatoscopy. J Am Acad Dermatol. 2000; 42(1 Pt 1):25-32.
3. Akay BN, Kocyigit P, Heper AO, Erdem C. Dermatoscopy of flat pigmented facial lesions: diagnostic challenge between pigmented actinic keratosis and lentigo maligna. Br J Dermatol. 2010; 163(6): 1212–7.
4. Nascimento MM, Shitara D, Enokihara MM, Yamada S, Pellacani G, Rezze GG. Inner gray halo, a novel dermoscopic feature for the diagnosis of pigmented actinic keratosis: clues for the differential diagnosis with lentigo maligna. J Am Acad Dermatol. 2014;71(4):708-15.
5. Nascimento MM. Lentigo maligno, lentigo maligno melanoma e queratose actínica pigmentada. In: Rezze GG; Casagrande J, editors. Atlas de Microscopia Confocal na Dermatologia. São Paulo: Editora Lemar; 2016. p. 139-49.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}