


Leila David Bloch1; Cassiano Carlos Escudeiro 1; Fernanda Daud Sarruf 1; Neusa Yuriko Sakai Valente2
Received on: 16/05/2017
Approved on: 07/03/2018
Study conducted at Instituto de Pesquisa Clínica Integrada (IPClin) – Jundiaí (SP), Brazil.
Financial support: The study received financial support from SM Empreendimentos Farmacêuticos Ltda / Fagron
Conflict of interests: The authors state they have no personal, commercial, academic, political or financial interests in this manuscript
Introduction: Latanoprost has been shown to have potential for the treatment of hair loss evidenced by increased thickness and length of eyelashes and hypertrichosis that can be observed when it is used in the periorbital region.
Objective: To evaluate the effectiveness of latanoprost, used isolatedly or in associations, for reducing hair loss and/or stimulating its growth in patients bearers of telogen effluvium or androgenic alopecia.
Methods: A comparative, double-blind study was carried out during 180 days, with 6 groups: G1 - placebo, G2 - 5% minoxidil, G3 - 5% minoxidil + 0.005% latanoprost, G4 - 0.005% latanoprost, G5 - 5% minoxidil + 0.010% latanoprost, G6 - 0.010% latanoprost. The total and percentage count of hair strands was carried out based on phototrichogram in the anagen and telogen phases.
Results: There was improvement in G2 (total number of hair strands, number of anagen strands in D92 and D180), G3 (total number of hair strands and number of anagen hair strands in D242), G4 (total number of strands in D182, and number of anagen hair strands in D92 and D182), and G5 (total number of hair strands in D182, percentage of telogen and anagen hair strands and number of anagen hair strands in D92 and D182). Treatment of G6 did not yield significant difference regarding the placebo.
Conclusions: The treatments with 5% minoxidil, 5% minoxidil + 0.005% latanoprost, 0.005% latanoprost, 5% minoxidil + 0.010% latanoprost were shown effective in controlling hair loss and in increasing the total number of hair strands.
Keywords: Alopecia; Hair; Minoxidil
Both in men and women, androgenetic alopecia and telogen effluvium are among the most common causes of hair loss. Androgenetic alopecia is an androgen-dependent condition characterized by miniaturization of hair follicles, with shortening of the anagen phase (phase of active hair growth) and lengthened telogen phase (“rest” phase) in each development cycle of the hair follicles.1-4 Telogen effluvium is characterized by increased number of hairs in the telogen phase and increased number of hairs shed per day. It can be associated to many factors, such as nutritional deficiencies (zinc, iron, essential fatty acids, etc.), endocrine disorders (thyroid, menopause, etc.), stress and drug reactions, among others.
Currently, there are not many options available for the treatment of hair loss, being minoxidil the only treatment approved by the Food and Drug Administration (FDA) for topical use. Minoxidil is a vasodilating agent originally used for the treatment of systemic hypertension and used topically for the treatment of androgenetic alopecia in humans.5
Latanoprost is analogous to prostaglandin F2, used for the treatment of open-angle glaucoma and ocular hypertension. This substance demonstrated potential for the treatment of hair loss because of the side effects seen with its topical use on the ocular region, mainly thickening and lengthening of eyelashes and hypertrichosis.6,7
The mechanism of action of these substances are not completely understood. Minoxidil seems to act by stimulating hair follicles, particularly those dormant, prolonging the anagen phase,5 whereas latanoprost seems to act by stimulating the anagen phase, increasing the conversion of vellus hair into terminal hair. The objective of this study was to evaluate the efficacy of minoxidil and latanoprost, in isolation or associated, and confirm if these substances are capable of reducing hair shedding and/or stimulate hair growth on patients with androgenetic alopecia and/or telogen effluvium.
Double-blind, comparative between six treatment groups: G1: placebo - control inactive product; G2: topical lotion containing minoxidil 5%; G3: topical lotion containing 5% minoxidil + 0.005% latanoprost; G4: topical lotion containing 0.005% latanoprost; G5: topical lotion containing 5% minoxidil + 0.010% latanoprost; G6: topical lotion containing 0.010% latanoprost.
The distribution of the participants in the above-mentioned groups was randomized.
The study was performed at the Instituto de Pesquisa Clínica Integrada – IPclin (Jundiaí-SP). Before the study commenced, it was approved by the Committee of Ethics in Research of the same institution.
In total, 123 participants were included, with 21 participants in groups G1, G2 and G3, and 20 participants in groups G4, G5 and G6. An initial dermatological assessment was performed at the time of inclusion to verify the absence of initial clinical signs not compatible with the inclusion criteria of the study (D0).
The inclusion criteria were: healthy participants of both genders, phototype I to IV, age between 20 and 55 years, presence of androgenetic alopecia (stages I to III in men, according to the Hamilton scale and I to II in women, according to the Ludwig scale), intact skin on the area to be studied (scalp), habit of washing the hair at least 3 times a week and those who were not using any product for hair growth for at least 4 weeks before the study.
Exclusion criteria were: presence of cicatricial alopecia or concurrent scalp disorders (infections, severe psoriasis and seborrheic dermatitis); active atopic dermatitis; allergy to the products being tested; pregnancy or breastfeeding; candidates with renal, cardiac or liver transplant, immunodeficiencies, use of corticosteroids, antihistamines, immunosuppressants, retinoids or anti-inflammatories; previous hair transplant or surgery for scalp reduction; use of minoxidil or finasteride (oral or topical) within 6 months before the study; treatments with low energy light, infrared or laser within 6 months before the study; solar erythema on the area to be studied or predicted intense exposure to sun light or UV lamps during the study and use of hair extensions, wig or hair straightening during the 3 months prior to the study.
The products were used by the participants themselves at home, according to the following instructions: daily topical application on dry and clean scalp, using the fingertips. The participants were instructed to wash their hands soon after using the product.
Total duration of the treatment was 6 months (180 ± 4 days) for all participants, except for the group G3, whose treatment was prolonged for 2 more months (240 ± 4 days). The dermatological safety clinical evaluations were performed in the following experimental periods: D0, D30, D60, D90, D120, D150, D180, D210 and D240 (i.e., on the day of the first visit and 30 ± 2, 60 ± 4, 90 ± 4, 120 ± 4, 150 ± 4, 180 ± 4, 210 ± 4 and 240 ± 4 days after the first visit). On the same days, the participants filled out a questionnaire of sensitization, regarding possible clinical signs and discomfort experienced with the products being investigated.
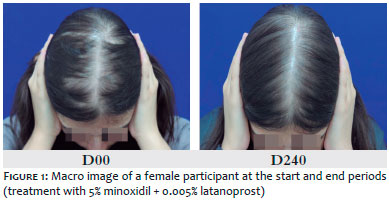
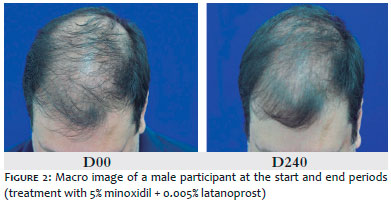
To visually assess the efficacy of the products in promoting uniformity and coverage of the scalp of the participants, we conducted a macro image registry using a photographic camera (Canon® T3i), with standardized configurations of camera, distance, background (blue) and lighting. The images were captured on the following experimental days: D0, D90 and D180. For the participants using minoxidil + 0.005% latanoprost (G3), the images were also taken on D240.
With the goal of evaluating hair growth and control of shedding provided by the use of the products being studied, according to the percentage increase of hairs in the anagen phase, reduction of the percentage of hairs in the telogen phase and increase in the total of hairs in the experimental phase, phototrichogram analyses were conducted. For this, images were captured with the device Dermoscope® Dynamic (FotoFinder Systems, Inc, Maryland, USA) in standardized conditions with the software Trichoscale, that performs a semiautomatic count of hairs in each phase of the growth cycle. Data obtained with the equipment: total number of hairs, percentage of hairs in the anagen phase and percentage of hairs in the telogen phase.
Images were captured two days after the participants had a small area of the scalp shaved. An area of the scalp was selected for the shaving (preferably on the right of left frontoparietal region) of approximately 2cm2, which was marked and shaved with an electrical shaver, in the direction of the hair shaft, allowing a maximum length of 1mm. Images were taken in the following experimental periods: D02, D92 and D182. For the participants in G3, images were also captured on D242. Data obtained with phototrichogram were analyzed statistically with the software SPSS version 17.0. A T test was performed with paired data to determine if there was any statistical difference between the periods of evaluation (p-value ≤ 0.05).
Of the 123 participants included in the study, 98 finished it and 25 withdrew for personal reasons not related to the research, being them 3 participants in G1, 4 in G2, 7 in G3, 4 in G4, 3 in G5 and 4 in G6. The high number of withdrawal can be attributed to the long duration of the study. The total of participants finishing the study for each treatment was: G1: 18 participants; G2: 17 participants; G3: 14 participants; G4: 16 participants; G5: 17 participants and G6: 16 participants.
None of the participants reported discomfort related to the treatments and no clinical signs were detected on the scalp after 30 ± 2, 60 ± 4, 90 ± 4, 120 ± 4, 150 ± 4, 180 ± 4, 210 ± 4 and 240 ± 4 days using the products. The evaluation of the results of the sensitization questionnaires showed that the products were well tolerated, with no significant signs of discomfort, pruritus, scaling or erythema on the scalp during the study.
Through comparative visual analysis of the macro images captured at each experimental period, no visual improvement was seen on groups G1 and G6 after 90 ± 4 and 180 ± 4 days of treatment, per treatment (respectively, D90 and D180), in relation to the initial aspect (D0).
For the other treatments, there was a visual improvement for: 35% of the participants in G2 (six), 36% of the participants in G3 (five), 19% of the participants in G4 (three) and 6% of the participants in G5 (one), on D30, D60, D120 and D150, in comparison to D0. Figures 1 and 2 demonstrate the visual improvement seen for the treatment with 5% minoxidil + 0.005% latanoprost.
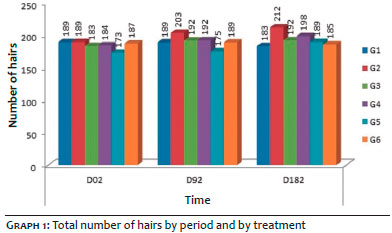
Based on comparative analysis, it was observed in the phototrichogram in relation to D0: increased total number of hairs on D92, caused by treatment 2 (p-value = 0.0010) and on D182 caused by treatment 2 (p-value = 0.0026), treatment 4 (p-value = 0.016) and by treatment 5 (p-value=0.005). Treatment 3 caused increased number of total hairs on D242 (p-value = 0,.0025).
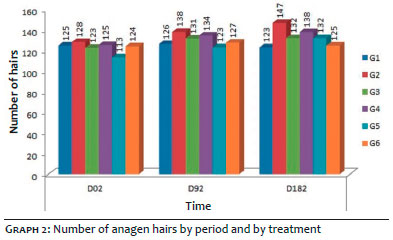
Regarding anagen hairs, an increased was observed on D92 in the groups receiving treatment 2 (p-value = 0.0005), 4 (p-value = 0.024) and 5 (p-value = 0.004) and also on D182 for the same treatments (treatment 2: p-value = 0.0003; treatment 4: p-value = 0.004; treatment 5: p-value = 0.0001), while treatment 3 increased the amount of anagen hairs after 242 days of use (D242) (p-value = 0.001).
None of the six treatments significantly reduced the amount of telogen hairs.
Graphs 1, 2 and 3 show the total number of hairs, the number of anagen hairs and the number of telogen hairs, respectively, on each period, per treatment.
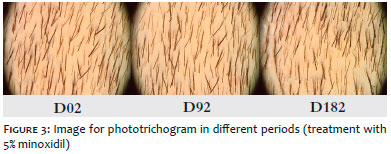
Figure 3 demonstrates the phototrichogram analysis in different periods (treatment with 5% minoxidil).
By observing the results obtained, 5% minoxidil (G2) significantly increased the total hairs and total anagen hairs, from the first 90 days of use. A superior result than seen previously, where the increased density of hairs was only seen after 24 weeks of using the product being tested.8 In another research, the increase was reported after 16 weeks.9
The 0.005% latanoprost (G4) yielded slightly inferior results to 5% minoxidil, in the total increase in the number of hairs and in the total number of anagen hairs after 180 days of use. On the other hand, 0.010% latanoprost (G6) did not yield statistically significant improvement, with comparable results to placebo. When used for a prolonged time and in a higher concentration, more effective results were seen. In the end of a 24-week treatment with 0.1% latanoprost, there was increased percentage of anagen hairs and reduction in the percentage of telogen hairs.6
The combination of both treatments had a better performance for 0.010% latanoprost (G5), with increased total number of hairs after six months of treatment, whereas 0.005% latanoprost associated to 5% minoxidil (G3) only yielded increased number of hairs after eight months of use.
None of the participants reported discomfort and no clinical signs were detected on the scalp during the study.
From the phototrichogram evaluation, we can conclude that:
Treatment with topical 5% minoxidil increased the total number of hairs and the total number of anagen hairs in the first 3 months of the study (D92).
Treatment with topical lotion containing 5% minoxidil + 0.005% latanoprost only increased the total number of hairs and the total number of anagen hairs after 8 months of study (D242).
Treatment with topical 0.005% latanoprost lotion increased the total number of hairs after 6 months of use (D182).
Treatment with topical 5% minoxidil 5% + 0.010% latanoprost lotion increased the total number of hairs after 6 months of use (D182).
Treatment with topical 0.010% latanoprost lotion showed no statistically significant difference compared to placebo.
Leila David Bloch | ORCID 0000-0001-9596-9583
Clinical support during the execution of the study and writing of the manuscript.
Cassiano Carlos Escudeiro | ORCID 0000-0001-6637-3430
Supervision on the execution and development of the study and proofreading of the final text.
Fernanda Daud Sarruf | ORCID 0000-0003-4454-6323
Coordination of the study, analysis of results and preparation of the article
Neusa Yuriko Sakai Valente | ORCID 0000-0002-8065-269
Proofreading of the final text
1. HALAL J. Tricologia e a Química Cosmética Capilar. São Paulo: Cengage Learning; 2011.
2. KLEINHANS ACS. Stress e raiva em mulheres com Alopecia Androgenética [dissertação]. Campinas: Pontifícia Universidade Católica de Campinas, Centro de Ciências da Vida, Área de Psicologia; 2012.
3. OLSEN EA. Hair. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick's Dermatology in General Medicine. 6th edition. United States of America: McGraw-Hill; 2003. p. 633-655.
4. Sinclair R, Patel M, Dawson TL Jr, Yazdabadi A, Yip L, Perez A, et al. Hair loss in women: medical and cosmetic approaches to increase scalp hair fullness. Br J Dermatol. 2011; 165(Suppl 3):12-18.
5. Pires FE, Fonseca MB, Ramos-e-Silva M. Minoxidil nas alopecias. Folha Médica 1994;108(4):113-17.
6. Blume-Peytavi U, Lönnfors S, Hillmann K, Bartels NG. A randomized double-blind placebo-controlled pilot study to assess the efficacy of a 24-week topical treatment by latanoprost 0,1% on hair growth and pigmentation in healthy volunteers with androgenetic alopecia. J Am Acad Dermatol. 2012;66(5):794-800.
7. Sasaki S, Hozumi Y, Kondo S. Influence of prostaglandin F2alpha and its analogues on hair regrowth and follicular melanogenesis in a murine model. Exp Dermatol. 2005;14(5):323-8.
8. Blume-Peytavi U, Hillmann K, Dietz E, Canfield D, Bartels NG. A randomized, single-blind trial of 5% minoxidil foam once daily versus 2% minoxidil solution twice daily in the treatment of androgenetic alopecia in women. J Am Acad Dermatol. 2011; 65(6): 1126-34.
9. Olsen EA, Whiting D, Bergfeld W, Miller J, Hordinsky M, Wanser R, et al. A multicenter, randomized, placebo-controlled, double-blind clinical trial of a novel formulation of 5% minoxidil topical foam versus placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2007; 57 (5):767-74.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}