


Emerson de Andrade Lima1; Mariana de Andrade Lima1; Cláudio Eduardo Cavalcante de Araújo2,3; Yara Maria Maia Nakasawa2,3; Nilma Cintra Leal2,3
Received on: 20/10/2017
Approved on: 12/01/2018
Study conducted at Instituto Aggeu Magalhães (IAM), Fundação Oswaldo Cruz (FIOCRUZ) – Recife (PE), Brazil.
Financial support: None
Conflict of interests: None
Introduction: Retinoic acid in peeling solution is widely used in the treatment of photoaging. To date, the degree of sterility of these solutions or the safety of their use in skins whose integrity has been lost through microneedling interventions is unknown.
Objectives: To evaluate the bactericidal potential of 3% and 5% retinoic acid in peeling solution, with and without a colored vehicle, as well as the safety and tolerance to its administration immediately after application with microneedles.
Methods: Samples of 3% and 5% retinoic acid solution, with and without a colored vehicle, prepared by two dispensing pharmacies (A and B) were exposed to Pseudomonas aeruginosa and Staphylococcus aureus colonies. These solutions were used as drug delivery agents after percutaneous induction of collagen with needles.
Results: The samples evaluated in D0, D30, D60 and D90 indicated the presence of bactericidal capacity of the tested agents. The use of the solutions following intervention with microneedles was well tolerated and yielded satisfactory results.
Conclusion: The retinoic acid peeling solution can be safely used following procedures that lead to a loss of integrity of the skin barrier. The absence of adverse effects and good results yielded by the procedure suggest that the association of microneedling and retinoic acid peeling is an innovative, reproducible and safe proposal.
Keywords: Chemexfoliation; Therapeutics; Tretinoin
The proposal of ablative treatments aiming at stimulating and remodeling the collagen is advocated by dermatologists for a long time. It is known that mechanical or chemical removal of the epidermis favors cytokine release and migration of inflammatory cells that result in the replacement of the damaged tissue by a remodeled tissue.1 The use of retinoic acid as a chemical peel agent has been proposed for lightening, rejuvenation and improvement of the texture of the skin.2
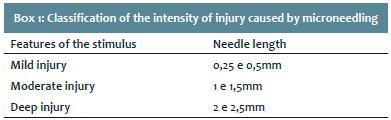
By stimulating cell turn over, transcutaneous elimination of pigments and a moderate collagen remodeling, retinoic acid enables softening of fine wrinkles, treatment for melasma and makes shallow scars more superficial, as well as improves the aspect of stretch marks. This agent is conventionally used in concentration ranging from 3% to 5%, in isolation or associated to other chemical peel substances such as Jessner’s solution, applied immediately before. Classified as a superficial peel, it aims at removing the stratum corneum, with injury to the epidermis, reaching the basement membrane and leading to repercussions in the dermis. The big advantage of retinoic acid chemical peel is its relative safety in all phototypes, limiting the risk of complications when all necessary recommendations for an ablative procedure are taken into consideration.1,2. The epidermis, stripped off its basement membrane, is replaced by a tissue seen as cicatricial, with flattening of the dermal papillae. An inflammatory response in the dermis is triggered by the destruction of the epidermis, leading to the production of parallel thick collagen bundles, different to the interlacing collagen network found in normal skin.3 Studies have revealed that transforming growth factor -β (TGF-β) plays an important role in the first 48 hours of scar formation. Whereas TGF-β1 and TGF-β2 promote formation of cicatricial collagen, TGF-β3 seems to promote regeneration and healing of the wound due to a more physiologic collagen, almost with no feature of the pre-existing one. In an attempt to achieve a shorter time for resolution after the procedure and reduce the risk of complications, we currently observe a trend to indicating procedures that avoid deepithelization.4,5 Percutaneous collagen induction with needles proposes the stimulation of collagen production preventing deepithelization. Percutaneous Collagen Induction, first assessed by the African plastic surgeon Des Fernandes,6 whose studies with 480 patients with scars, wrinkles and laxity yielded good results, has been used all over the world. In Brazil, Emerson Lima7 registered the name percutaneous collagen induction with needles (IPCA®). This intervention produces hundreds of microlesions through a roller with microneedles and results in partial loss of the integrity of the cutaneous barrier, with the dissociation of keratinocytes as a target, and stimulates the release of cytokines such as mainly interleukin-1α, but also interleukin-8, interleukin-6, TNF-α and GM-CSF. This process results in dermal vasodilation and keratinocyte migration to repair the epidermal damage.4-6 Lima EVA et al7 evaluated, in an experimental study, the relationship between the length of the needle and the depth of the injury caused using pig skin, which is considered similar to human skin.7 From the results, the authors proposed a classification into mild, moderate and deep injury, related to the length of the needle and its ability to cause the planned damage (Box 1).7 Considering the diffuse erythema with few petechiae seen in moderate injuries, a favorable condition to receive an active substance, this article proposes the use of the IPCA® technique, associated to retinoic acid chemical peel as drug delivery, with the objective to optimize results of procedures to improve the quality of the skin. We assumed that an active substance applied as drug delivery over the skin that lost its integrity due to a previous procedure needs to be sterile. Until now, studies published do not offer support about the safety of using retinoic acid solution, commonly used for chemical peels, after IPCA®. Therefore, we began our investigation with the evaluation of this active substance.
This study aimed at evaluating the bactericidal action of 3% and 5% retinoic acid solutions used for superficial chemical peels, compounded by two different independent pharmacies, as well as if the sterility of these solutions would be affected by adding coloring, by time after compounding or by storage conditions.
Another objective was to evaluate the safety of the above-mentioned solutions, used in procedures where skin integrity was lost, allowing their use as drug delivery.
Evaluation of the safety of 3% and 5% retinoic acid as drug delivery agents.
Tinted and non-tinted retinoic acid solutions at 3% and 5% in alcohol where evaluated, compounded in two different pharmacies: A (Roval) and B (Pharmapele), both in Recife (PE), Brazil), with a shelf life of 90 days, keep in room temperature (RT) and at 4°C. The objective was to investigate sterility and bactericidal action.
Sterility of the four solutions from each pharmacy was evaluated at the same day of compounding, with seeding of an amount of 100µL from each sample in BHI agar (Brain Heart Infusion) and incubated at 37°C for 24 hours, observing bacterial growth.
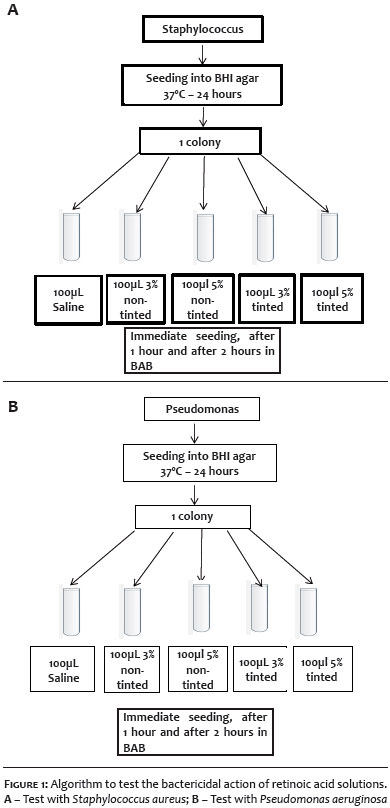
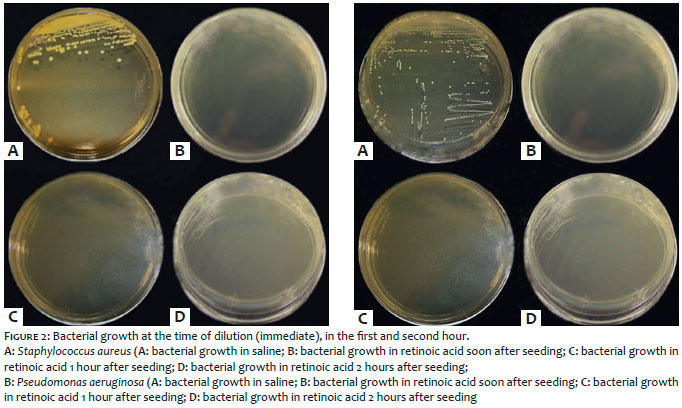
On the same occasion, bactericidal action was initially tested with an amount of 100µL of retinoic acid from each packaging, diluted in 480µL of BHI medium plus 20µL of a 24-hour culture of Pseudomonas aeruginosa. The same experiment was repeated for Staphylococcus aureus (Figure 1). Retinoic acid was diluted five times in this procedure. Bactericidal action of retinoic acid was also evaluated in the second and third months of shelf life. This time, the product was not diluted, as it is used for chemical peels and recommended by the manufacturers, at 3% and 5%, tinted and non-tinted, stored at RT and at 4°C (fridge temperature recommended by the pharmacies for conservation of the product). A quantity of 500µL from each jar was placed into sterile microtubes, inoculated with P. aeruginosa or S. aureus colony, and part of the homogenized product was seeded into BHI agar plates in three situations: soon after homogenization, and one and two hours after. As control, bacteria were also inoculated into sterile saline. Plates were incubated at 37°C for 24 hours, when bacterial growth was observed (Figure 2).
In the first seeding for evaluation of the product sterility, no bacterial growth was observed in any of the plates, what confirmed the sterility of the product in all packages tested. In the tests performed in the first month, when the product was diluted, bacterial growth was seen in many situations. In view of this, in the second and third months of shelf life tests were performed as recommended by the manufacturer and as it is conventionally used for chemical peels. From the seeding soon after homogenization of the inoculum there was growth only in saline and some jars of retinoic acid. Seeding in the first and second hours only showed growth in saline (Figure 2), confirming the bactericidal action of tinted and non-tinted 3% and 5% retinoids acid recommended for use. It was also seen that the product is not changed whether stored at room temperature or at 4°C (Table 1). Of note is the bactericidal effect of agents tested with S. aureus, even considering that this bacterium has thicker cell membrane and is supposedly more resistant.
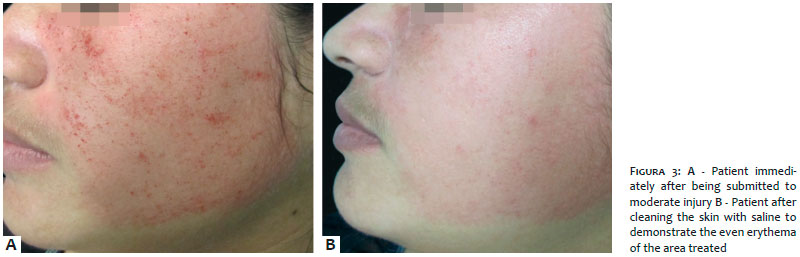
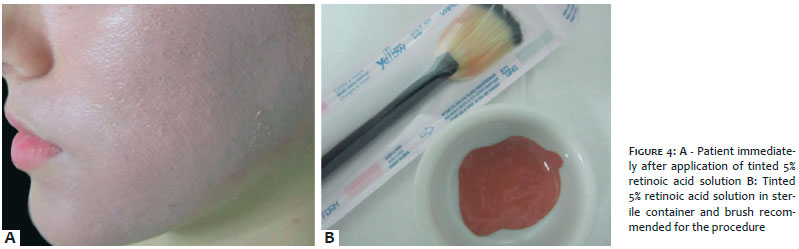
In view of the proven bactericidal action of tinted and non-tinted 3% and 5% retinoic acid solutions, we proposed its use as drug delivery agent in association with IPCA®. For this purpose, we proposed moderate injury (Figure 3) for the application of tinted 5% retinoic acid (Figure 4), considering that with this end point the skin would be subject to receiving the active substance with no interference of a more intense bleeding as the one seen in deep injuries. Twelve volunteers participated in this assessment, with complaints of acne scars and photoaging, between 21 and 38 years of age, seen at the Outpatient Clinic of Cosmiatry of the Santa Casa de Misericórdia do Recife. The study was conducted according to the recommendations of the 1996 declaration of Helsinki, modified in 2013, and authorized by the Ethics Committee of the institution. The procedure was conducted under topical anesthesia with 4% lidocaine cream (Dermomax® Aché, São Paulo, Brazil) applied 40 minutes before the intervention. A device with needle length of 1.5mm (Dr.Roller® Mooham Enterprise Co. Gyeonggi-do South Korea, Anvisa n.80669600001). We performed back and forth movements, forming horizontal lines that were subsequently crossed by vertical and diagonal lines until a diffuse erythema developed all over the face, with mild pin-point bleeding, characterizing moderate injury (Figure 3).
Immediately after, a tinted 5% retinoic acid solution was applied using a sterile brush all over the area treated (Figure 4) and left for 2 hours, when it was removed with water and liquid soap, at home. It was recommended the patients did not apply any products on the skin for the following 8 hours, using SPF > 50 sunscreen. All subjects evaluated were photographed before and after 30 days of the procedure by the same researcher, with the same camera and using the same light. Eight days after the procedure, the patients returned to the clinic to evaluate tolerability of the intervention.
In the eighth day post-procedure there were no complaints of discomfort, burning, erythema or peeling in the 12 patients treated. Two reported mild burning between 48 and 72 hours after the intervention and one reported intense peeling after 72 hours accompanied by erythema. None of the subjects had to take time off work in the period after the procedure, and all continue to use only sunscreen until eight days after. In the 30-days follow-up appointment, all reported lightening, increased glow and vigor, with softening of superficial scars and fine wrinkles. Two independent evaluating dermatologists who analyzed the standardized photographs, considered that the intervention resulted in an overall improvement of the quality of the skin in the whole group treated. On physical examination, lightening, improved texture, increased glow and closure of pores. All in the group chose the option “very satisfied” when answering the evaluation questionnaire, with the options of little satisfied, moderately satisfied, very satisfied. No side effects such as persistent erythema, hypersensitivity, irritation, pruritus or post-inflammatory hyperpigmentation were seen. Six of the 12 patients had moderate peeling even after seven days of the procedure. None of them had to stop their daily activities because of the intervention.
The benefits of IPCA® on the correction of scars, wrinkles and laxity are well established, as well as the ability of retinoic acid peel in providing cosmetic improvement of the quality of the skin. Until present, retinoic acid peel has been proposed to intact skin, when there is no need to question its sterility, even less its bactericidal action, because of the protection offered by the cutaneous barrier. To our knowledge, this is the first investigation study that evaluated the destructive ability of retinoic acid over two common bacteria in the environment, S. aureus and P. aeruginosa. Despite studies on the viability of microorganisms, no reports were found on the sterility of retinoic acid solutions used for chemical peels.8,9 According to our results, it was possible to use this active substance safely, even after disruption of skin integrity with a moderate injury caused by microneedles. This proposal provides another therapeutic option of association of techniques in the dermatological practice. Tests using the solutions kept in the fridge and at room temperature, even three months after manufacturing, showing their bactericidal action, offer the safety of a formulation for drug delivery after intervention with IPCA®. It was also important the evaluation of different concentrations (3% and 5%), besides the feature of tinting, confirming the same reliable profile. IPCA® alone leads to platelet and neutrophil release, responsible for making growth factors available, which act on the keratinocytes and fibroblasts, such as transforming growth factors a and β (TGF-a and TGF-β), platelet-derived growth factor (PDGF), protein III activator of the connective tissue and connective tissue growth factor, followed by neutrophils, angiogenesis, fibroblast proliferation and production of collagen type III, elastin, glycosaminoglycans and proteoglycans. In parallel, fibroblast growth factor, TGF-a and TGF-β are secreted by monocytes. Approximately 5 days after the injury, the fibronectin matrix is formed, allowing deposit of collagen underneath the basal layer of the epidermis. This collagen type III is slowly replaced by collagen type I, more longer lasting. In order for this inflammatory cascade to develop, the trauma caused by the microneedle should reach depths of 1mm to 3mm in the skin, resulting in red blood cell columns followed by edema of the treated area and almost immediate homeostasis. The intensity of these reactions is proportional to the length of the needle used in the procedure.10-14 This study proposes a moderate injury associated to the action of tinted 5% retinoic acid for optimization of the results, as well as aiming at masking the small hematic crusts caused by IPCA®. The immediate return to work activities of the whole group studied with only photoprotection provides convenience to the intervention, what favors its application.
Retinoic acid solution for chemical peels can be safely used after procedures that lead to loss of integrity of the cutaneous barrier.
The absence of side effects and patient’s and assessor’s satisfaction allows for the suggestion of the association of microneedling and retinoic acid peel as an innovative, reproducible and safe proposal.
Emerson de Andrade Lima | ORCID 0000-0002-6132-5031
Clinical evaluation, literature review, writing and proofreading.
Mariana de Andrade Lima | ORCID 0000-0003-2499-0873
Clinical evaluation, literature review, writing and proofreading.
Cláudio Eduardo Cavalcante de Araújo | ORCID 0000-0001-7190-6625
Laboratory evaluation of the samples.
Yara Maria Maia Nakasawa | ORCID 0000-0002-0178-6522
Laboratory evaluation of the samples.
Nilma Cintra Leal | ORCID 0000-0001-9769-7630
Laboratory evaluation of the samples.
1. Jackson A. Chemical Peels. Facial Plast Surg. 2014; 30(1):26-34.
2. Kang HY, Valerio L, Bahadoran P, Ortonne JP. The role of topical retinoids in the treatment of pigmentary disorders: an evidence-based review. Am J Clin Dermatol 2009; 10(4):251-60.
3. Brody HJ. Trichloroacetic acid application in chemical peeling. Operative Techniques Plast Reconstr Surg. 1995; 2(2):127-8.
4. Aust MC. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation-fact or fiction?. Plast Reconstr Surg. 2008; 122(5):1553-63.
5. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997;21(1):48-51.
6. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
7. Lima EVA, Lima MA, Takano D. Microneedling experimental study and classification of the resulting injury. Surg Cosmet Dermatol. 2013;5(2):110-4.
8. Paris I, Paci A, Rey JB, Bourget P. Microbial growth tests in anti-neoplastic injectable solutions. J Oncol Pharm Practice. 2005; 11(1): 7-12.
9. Sarakbi I, Federici M, Krämer I. Viability of microorganisms in novel chemical and biopharmaceutical anticancer drug solutions. Eur J Parenteral Pharm Sci. 2015; 20(1): 5-12.
10. Fernandes D, Signorini M. Combating photoaging with percutaneuos collagen induction. Clin Dermatol. 2008; 26(2): 192-9.
11. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy (pci)-an alternative treatment for scars. Wrinkles skin laxity. Plast Reconstr Surg. 2008;121(4):1421-9.
12. Bal SM, Caussian J, Pavel S, Bouwstra JA. In vivo assessment of safety of microneedle arrays in human skin. Eur J Pharm Sci. 2008; 35(3):193-202.
13. Cohen KI, Diegelmann RF, Lindbland WJ. Wound healing: biochemical and clinical aspects. Ann Surg. 1992; 216(5):613.
14. Fabroccini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scar treatment using skin needling. Clin Exp Dermatol. 2009; 34(8):874-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}