


Fernanda Zanenga Varaschin1; Carlos Alexandre Ayoub2; Nelson Foresto Liezer3; Maria Eugenia Torres Di Luciano4
Vitiligo is a hypopigmentation disorder that is characterized by macules and selective destruction of functional epidermal melanocytes. It is characterized by defilements and circumscribed depigmented patches. Vitiligo affects around 0,5% about 0.5% -2% of the general population worldwide, and is not observed preference for sex and ethnicity. The goals of treatment are repigmentation of vitiligo and stabilization of depigmentation process. We report the case of a 53-year-old female patient who underwent underwent experimental stem cell therapy with autologous biologically expanded stem cells isolated from hair follicle, holding three sessions with three months apart. The vitiligo affected area was relatively decreased in density with a rare repigmentation pattern.
Keywords: STEM CELLS; VITILIGO; THERAPEUTICS
Vitiligo is an acquired idiopathic disorder characterized by the selective destruction of functional epidermal melanocytes. Melanocytes disappear from the skin surrounded by mechanisms that have not yet been fully identified.1,2Vitiligo affects 0.5% to 2% of the general population worldwide, with no distinction for gender or ethnicity. It can occur at any period of a person’s life, with the mean age of onset being 20 years old.2 The disorder is characterized by circumscribed depigmented patches that vary in number and size. The disease can be classified according to the distribution of the lesions as: localized (focal, segmental and mucosal) and generalized (acrofacial, vulgaris and universalis). The physiopathological mechanism of vitiligo is not yet clearly understood. It is a multifactorial disorder related to genetic and non-genetic factors. Studies suggest that vitiligo is a non-Mendelian, polygenic inheritance disease, with recurrence of 20% to 30% among first-degree relatives. Among the known non-genetic hypotheses, the most important are: autoimmune destruction of melanocytes, intrinsic defect in the structure and function of melanocytes, imperfect defense against free radicals, and reduction of melanocyte survival.3The objectives of the treatment are the repigmentation and the stabilization of the depigmentation process. Among the repigmentation therapies are the Narrow Band UVB, psoralen photochemotherapy, topical and immunosuppressant corticosteroids, surgical therapies and micropigmentation.4-6The treatment of vitiligo is difficult and long since, despite the available therapeutic arsenal, the disease can progress with incomplete repigmentation depending on the affected area. Thus, new therapeutic approaches are emerging, being that stem cell therapy has a vast and unexplored potential in the treatment of patients with vitiligo. Stem cells are characterized by being undifferentiated, capable of proliferation and regeneration after tissue injury, presenting several subpopulations, and have been studied in the research on vitiligo. The skin, in particular, is a rich source of different types of stem cells: epidermal, hair follicles, sebaceous and sweat glands, as well as dermal mesenchymal with regenerative properties, which are increasingly being explored in vitiligo management strategies.
A 53-year-old female patient presented with vitiligo lesions four years previously, starting on the front, back of the hand, abdomen, and external genitalia (Figure 1). She was submitted to 30 sessions (three times a week) of PUVA Treatment (psoralen + UVA phototherapy) during the first year after the onset of the lesions. Due to the poor response to treatment, she dropped out of therapy and remained for the past three years without any oral or topical medication.
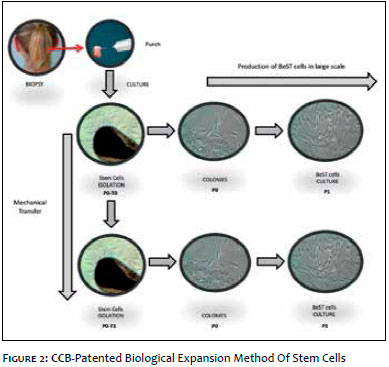
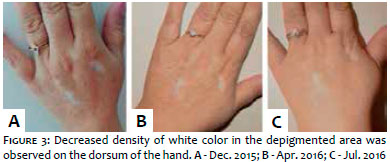
A circular 5mm fragment of skin from the left posterior region of the scalp was obtained from a punch and sent to the laboratory at the Cellular Technology Center - CCB - ISO N7. The various types of stem cells present in the skin sample were isolated and expanded using the biological method of stem cell expansion (Figure 2). After expansion,1.5x106/ml cells (second passage) were placed in a physiological solution (0.09% NaCl), in a syringe, and applied to the affected area. Thousands of stem cells are transplanted into the vitiligo areas with each procedure. The number of procedures required depends on the size of the affected area. The patient was submitted to experimental therapy with stem cells in December of 2015 (three sessions with three months interval). The images show the patient before the therapy,at the end of the treatment (last session) and four months after the last session (Figures 3 and 4).
The patient has not undergone any therapy for the improvement of her vitiligo lesions between the last session of the treatment in question and the time at which this article was prepared.
Vitiligo affects millions of people around the world, and the melanocytes, cells that give color to skin, play an important role in repigmentation. There is a theory that suggests that melanocytes are responsible for repigmentation in vitiligo, dividing and migrating to the surface along the epidermis. Nishimura et al. demonstrated that the stem cells in the bulge region could migrate towards the surface to the epidermis, resulting in repigmentation in animal models. Chemical and physical stimuli may promote the migration of precursor melanocytes involved in the repigmentation of vitiligo lesions.7, 8 Phototherapy can be used to accelerate this process, but success is not guaranteed, and sometimes there is no pigmentation after the procedure. The shade of the new pigmentation may be lighter, darker or more irregular than the surrounding normal skin. The technical aspect of the procedure, performed exclusively by the authors of this article, is the application of a mixture of biologically expanded autologous stem cells in the lesion of vitiligo. The cells are harvested from a painless biopsy on the scalp, expanded in vitro (Figure 2) and then transferred to the affected area with the aim of replacing the missing pigment cells, restoring the patient’s natural skin color. Repigmentation begins with the appearance of dotted or drop-like spots in the follicular ostia within the patch or in the centripetal direction from the edges (Figures 3 and 4). Pigmentation occurs due to the application of stem cells, which promotes the proliferation and migration of melanocytes from hair follicles to the basal layer of depigmented skin. The authors of the present article demonstrated the presence of evident decrease in the density of the area affected by vitiligo, with exceptional repigmentation. The usual treatment of vitiligo is difficult and long since, despite the available therapeutic arsenal, the disease can advance and complete repigmentation does not occur. Thus,in order to achieve success in the treatment of vitiligo, personalized stem cell therapy should also be considered as a way to provide adherence to treatment even when therapeutic failures occur.
By the present report, a relative decrease in the density of the area affected by vitiligo was observed, with a rare repigmentation pattern. These findings indicate the need for further studies on stem cell therapy for the treatment of vitiligo. The clinical efficacy of the stem cell transplantation in the studied patient suggests the existence of potential for the treatment of patients with vitiligo.
Fernanda Zanenga:
Chief investigator, patient evaluation, preparation of the study, bibliographic research (dermatologist physician at the Centro de Criogenia Brasil)
Nelson Foresto Lizier:
Co-investigator, preparation of the study protocol, drafting of the manuscript (biotechnologist at the Centro de Criogenia Brasil)
Carlos Alexandre Ayoub:
Co-investigator, preparation of the study protocol, patient evaluation (pediatrician physician and medical director at the Centro de Criogenia Brasil)
Maria Luciano:
Co-investigador, preparation of the study protocol (biotechnologist at the Centro de Criogenia Brasil)
1. Tamesis ME, Morelli JG. Vitiligo treatment in childhood: a state of the art review. Pediatr Dermatol. 2010;27(5):437-45.
2. Ortonne JP, Mosher DB, Fitzpatrick TB. Vitiligo and Other Hypomelanoses of Hair and Skin. New York: Springer US; 1983.
3. Moellmann G, Klein-Angerer S, Scollay DA, Nordlund JJ, Lerner AB. Extracellular granular material and degeneration of keratinocytes in the normally pigmented epidermis of patients with vitiligo. J Invest Dermatol. 1982;79(5):321-30.
4. Njoo MD, Westerhof W. Vitiligo. Pathogenesis and treatment. Am J Clin Dermatol. 2001;2(3):167-81.
5. Falabella R, Barona MI. Update on skin repigmentation therapies in vitilgo. Pigment Cell Melanoma Res. 2009;22(1):42-65
6. Forschner T, Buchholtz S, Stockfleth E. Current State of vitiligo therapy - evidence based analysis of literature. J Dtsch Dermatol Ges. 2007;5(6):467-75.
7. Staricco RG, Miller-Milinska A. Activation of the amelanotic melanocytes in the outer root sheath of the hair follicle following ultra violet rays exposure. J Invest Dermatol. 1962;39:163-4.
8. Quevedo WC Jr, Isherwoob JE. Influence of hair growth cycle on melanocyte activation in rabbit skin after a single application of methylcholanthrene. J Invest Dermatol. 1961;37:93-101.
This study was conducted at the Centro de Criogenia do Brasil (CCB)
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}