


Daniella de Grande Curi1; Cristiane Lima Roa2; Lana Maria de Aguiar3; Abdo Salomão Junior4; Edmund Chada Baracat5
Lichen sclerosus is a chronic dermatosis, usually anogenital and mainly affecting pos-menopausal women. The use of topical corticosteroids is the mainstay of medical treatment. Other treatments are topical testosterone, calcineurin inhibitors, photodynamic therapy, cryotherapy, antibiotic therapy and laser therapy. In this article, five patients with vulvar lichen sclerosus which had no response to treatment with topical clobetasol, had good results when treated with fractional Erbium:YAG laser 2940.
Keywords: LASER THERAPY; VULVAR LICHEN SCLEROSUS; 17-HYDROXYCORTICOSTEROIDS
Lichen sclerosus (LS) is a chronic and benign dermatosis that affects the genital and extragenital region.Vulvar involvement is predominantly observed in premenopausal and menopausal women, and may cause pruritus, pain, dyspareunia and sexual dysfunction (1,2).
Autoimmune and genetic factors are implicated in its etiology. Association with other autoimmune diseases corroborates this theory (3). The participation of the spirochaete Borrelia Burgdorferi is still controversial (1).
Clinically, it affects the perineum, labia majora and minora, clitoris and perianal region. It is characterized by hypochromic plaques, fissures, as well as causing a buried clitoris and fusion of the labia majora and minora. The main complaint is pruritus vulvae, associated or not with dysuria, dyspareunia and burning sensation. Lesions can also be observed lesions in genitocrural folds, thighs and buttocks (4).
Histologically the epidermis is scarce with hyperkeratosis, homogenization of collagen between the dermis and the epidermis, and lymphocytic infiltrate (4).
Some cases of LS can progress to squamous cell carcinoma, requiring the control and clinical follow-up of these patients (5).
Many patients respond to treatment with the abolition of signs and symptoms, but in other cases the signs remain and the symptoms are intermittent (6).
Currently, the treatment is done with a high-potency topical corticosteroid (clobetasol) with good results. Other options are topical immunomodulators (tacrolimus and pimecrolimus), photodynamic therapy, cryotherapy, antibiotic therapy and laser therapy (7). The use of laser in the treatment of lichen is recent and few studies have used the fractional CO2 laser (8,9,10); none have used the fractional 2,940 Er:YAG fractional laser.
The purpose of this study was to evaluate the efficacy of the 2,940 Er:YAG fractional laser in the treatment of LS in cases where other treatments were not successful in relieving symptoms.
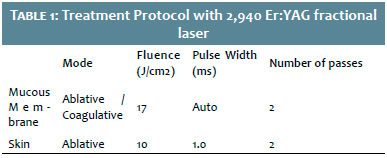
We have described in this article five cases of patients with LS confirmed by histological exams, resistant to the use of clobetasol who underwent five sessions of 2,940 Er:YAG fractional laser (Solon Platform – LMG, MG, Brasil) every 21 days, with an important improvement of lesions and pruritus. The parameters used are shown in Table 1.
Case 1
MSNL, 68 years old, Caucasian, underwent menopause 13 years previously, with clinical and anatomopathological diagnosis of LS for 8 years, intense vulvar pruritus without improvement with clobetasol 0.5 mg/g daily. At the examination presented with a loss of the vulvar architecture, hypopigmentation, whitish plaques and excoriations (Figure 1).
Two months after the last session the patient reported complete improvement of pruritus and that she was no longer using the topical clobetasol. During the clinical examination, presented improvement of skin texture and areas of repigmentation (Figure 1).
Case 2
MAV, 69 years old, Caucasian, underwent menopause 24 years previously, complaint of intense vulvar pruritus for 2 years. Clinical and anatomopathological diagnosis of LS, using clobetasol 0.5mg/g daily without improvement of pruritus. At examination, vulva with hypopigmentation and areas of leukoplakia mainly on the clitoral hood. (Figure 2).
Two months after the end of treatment, the patient reported improvement of 70% of pruritus and that since the last consultation she had not used the topical clobetasol. During the clinical examination, presented significant improvement of leukoplakia and areas of repigmentation (Figure 2).
Case 3
ERN, 70 years old, Caucasian, underwent menopause 25 years previously, presenting intense vulvar pruritus and little response to daily use of clobetasol 0.5mg/g. Upon examination, presented with a loss of the vulvar architecture, erythematous and atrophic mucosa, and fusion of the labia minora (Figure 3).
Two months after the end of the treatment, the patient reported improvement of 80% of pruritus and that since the last consultation she had used the topical clobetasol only when she had pruritus (once a week). During the examination, presented improvement of texture and separation of the labia minora (Figure 3).
Case 4
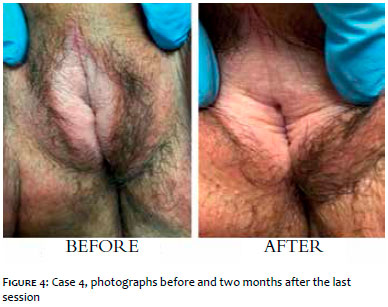
VES, 60 years old, Caucasian, underwent menopause 6 years previously, reported vulvar pruritus for over 1 year, using clobetasol 0.5mg/g twice a day since then, with little improvement. Upon examination, were observed loss of the vulvar architecture, hypopigmented and atrophic mucosa and whitish plaques (Figure 4.1).
Two months after the end of the treatment, the patient reported improvement of 100% of pruritus and that since the last consultation had not used the topical clobetasol. During the examination, presented improvement of the texture and color of the vulvar mucosa (Figure 4.2).
Case 5
JGP, 67 years old, Caucasian, underwent menopause 24 year previously, presenting vulvar pruritus for over 23 years. She has used several topical medications without clinical improvement and underwent surgery for debridement in the clitoral region one year previous due to phimosis and abscess formation. Has been using clobetasol 0.5mg/g for 6 months, once a day with little response. During the clinical examination presented loss of the vulvar architecture, hypopigmented and atrophic mucosa (Figure 5).
Two months after the end of the treatment, the patient reported improvement of 100% of the pruritus and that she had not used the topical clobetasol. During the examination, presented improvement of the texture and pigmentation of the vulva (Figure 5).
Lichen Sclerosus can occur at all ages and both genders, but it is more frequently seen in postmenopausal women (11). Pruritus is the main complaint, often important, causing discomfort and even social isolation. Dyspareunia and loss of vulvar architecture are also common (12). Severe pruritus was reported by all patients, even with daily clobetasol use prior to the start of the treatment. After the third session there was a significant improvement in pruritus (of at least 50%) and a decrease in the frequency of daily corticosteroid application to once a week or less.
The pain during laser application was reported by all patients as moderate in the first session and mild in the following. We believe that the fear of the unknown towards the treatment, in its first session, was responsible for the greater intensity of the pain, because in the subsequent sessions it was less intense, without change to the parameters that were used. The topical anesthetic may ease the pain during the application.
Godoi et al., in 2015 (2) compared tissue biopsies with and without lichen sclerosus and found in patients with LS decreased elastic fibers in the upper layer of the dermis, associated with the increase of type V collagen and decreased expression of extracellular matrix protein 1, the latter two probably due to poor tissue repair due to the disappearance of the elastic fibers. As demonstrated in other areas of the body, laser induces remodeling of connective tissue through the production of collagen and elastic fibers (13). This process involves the interaction of the heat shock proteins 43, 47 and 70 that induce local increase of cytokines such as TGF-α (transforming growth factor alpha) that stimulates proteins in the matrix such as collagen, FGF (fibroblast growth factor) that stimulates angiogenic activity, EGF (epidermal growth factor) that stimulates reepithelialization, PDGF (platelet-derived growth factor) that stimulates fibroblasts to produce the components of the extracellular matrix and VEGF (vascular endothelial growth factor) that regulates angiogenesis (14). We believe that the remodeling promoted by the laser may play an important role in the reorganization of elastic fibers and consequently in the treatment of lichen sclerosus, bringing hope that a more stable treatment, with better results may be used in these patients.
Our subjective (pruritus) and objective (aspect of the vulva) results corroborate with our hypothesis; however, studies with more patients are necessary.
The 2,940 Er:YAG fractional laser has shown promise in the treatment of vulvar lichen sclerosus, even in resistant cases to topical treatment with clobetasol.
Daniella De Grande Curi:
Conception of the study project, implementation and drafting of the manuscript
Cristiane Luma Roa:
Conception, implementation and drafting of the manuscript
Lana Maria Aguiar:
Conception of the study project and implementation
Abdo Salomão Junior:
Supply of the Solon device and drafting of the manuscript
Edmund Chada Baracat:
Drafting of the manuscript
1. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. 2013; 14(1):27-47.
2. Godoy CA, Teodoro WR, Velosa AP, Garippo AL, Eher EM, Parra ER, et al. Unusual remodeling of the hyalinization band in vulval lichen sclerosus by type V collagen and ECM 1 protein. Clinics (Sao Paulo). 2015; 70(5):356-62.
3. Murphy R. Lichen sclerosus. Dermatol Clin. 2010; 28(4):707-15.
4. Leibowitch M. Lichen sclerosus. Semin Dermatol. 1996; 15:42-6.
5. Micheletti L, Preti M, Radici G, Boveri S, Di Pumpo O, Privitera SS, et al. Vulvar lichen sclerosus and neoplastic transformation: a retrospective study of 976 cases. J Low Genit Tract Dis. 2016; 20(2):180-3.
6. Neill SM, Ridley CM. Management of anogenital lichen sclerosus. Clin Exp Dermatol. 2001; 26(8):637-43.
7. Neill SM, Tatnall FM, Cox NH. British Association of Dermatologists' guidelines for the management of lichen sclerosus. Br J Dermatol. 2010 Oct;163(4):672-82.
8. Peterson CM, Lane JE, Ratz JL. Successful carbon dioxide laser therapy for refractory anogenital lichen sclerosus. Dermatol Surg. 2004; 30(8):1148-51.
9. Aynaud O, Plantier F. Genital lichen sclerosus treated by carbon dioxide laser. Eur J Dermatol. 2010; 20(3):387-8.
10. Lee A, Lim A, Fischer G. Fractional carbon dioxide laser in recalcitrant vulval lichen sclerosus. Australas J Dermatol. 2016; 57(1):39-43.
11. Kirtschig G. Lichen Sclerosus-Presentation, Diagnosis and Management. Dtsch Arztebl Int. 2016; 113(19):337-43.
12. Bradford J, Fischer G. Long-term management of vulval lichen sclerosus in adult women. Aust. N Z J Obstet Gynaecol. 2010; 50(2):148-52.
13. Perino A ,Calligaro A, Forlani F, Tiberio C, Cucinella G, Svelato A, et al. Vulvo- vaginal atrophy: A new treatment modality using thermo-ablative fractional CO2 laser. Maturitas. 2015; 80(3): 296-301.
14. Salvatore S, Maggiore ULR, Athanasiou S, Origoni M, Candiani M, Calligaro A, et al. Histological study on the effects of microablative fractional CO2 laser on atrophic vaginal tissue: an ex vivo study. Menopause. 2015; 22(8):845-9
This study was conducted at the Medical School, Hospital das Clinicas, Universidade de São Paulo (HCFMUSP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}