


Elisa de Oliveira Barcaui1; Antonio Carlos Pires Carvalho2; Carlos Baptista Barcaui3
The presence of foreign bodies located on the skin, their size, constitution and precise location are often not perceptible on dermatological clinical examination. Despite their benign nature, the presence of foreign bodies in the skin is associated to high morbidity. High frequency ultrasonography has been widely used in different areas of Dermatology. Technological development and the introduction of devices offering high frequency and high resolution makes this method useful in identifying and guiding the removal of foreign bodies located in the skin. The authors describe a case where high frequency ultrasonography was used to identify and remove a rayfish stinger.
Keywords: ULTRASOUND; ULTRASSONOGRAPHY; FOREIGN BODY; SURGERY
Different methods of imaging based diagnosis, such as radiography, computerized tomography (CT), magnetic resonance imaging (MRI) and ultrasound are used to detect the presence of foreign bodies (FB) in the soft parts of the body.1 However, the FB’s constitution, size and depth at which it is located can significantly influence the accuracy of the imaging method. In this way, it is crucial to choose the proper imaging technique for identify a FB.
Brazil has an extensive coastline, which is home to a diverse wildlife. Bathing in the sea is a common habit, entailing that people are more susceptible to exposure to the aquatic fauna. The authors of the present article describe a case in which high frequency ultrasound (HFUS) was used to diagnose a persistent skin disorder after trauma caused by a stingray, detecting the presence of a stinger, determining its exact location and shape, and serving as a guide for a surgical removal procedure.
A 72 year-old Brazilian male patient, had swelling and complained of pain in the third left toe developed two months before, after having been stung by a stingray on the dorsum of the left foot, and treated with topical antiseptic (Figure 1). The patient did not report anything relevant regarding the medical or family history. The physical examination revealed edema with limitation of motion of the interphalangeal joint of the third left toe and pain on palpation. No alteration in the integrity of the skin of the toe in question could be observed (Figure 2).
Ultrasonography was performed with a linear transducer using a 22MHz frequency at the location of the scar on the dorsum of the foot and of the third left toe, showing no considerable alterations.
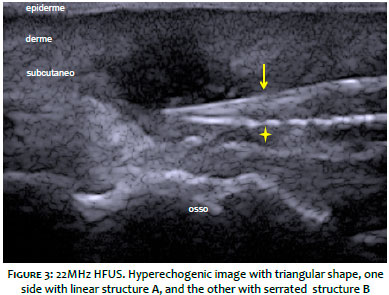
The examination carried out in the plantar region of the toe in question suggested the presence of an hyperechoic structure with elongated triangular shape, measuring 1.3 cm in its greater length, with one of the sides showing a linear profile and the other a serrated profile (Figure 3).
The patient underwent the removal of the FB (Figure 4) through a small incision made in the plantar region with guidance of the ultrasound examination, under local anesthesia. Systemic antibiotic was administered (Cefadroxil, 500mg, 12/12 hours, for 7 days). The post-operative coursed without events.
Foreign body is any objetct originated outside the body. When located in the soft parts of the body, it might have been originated by trauma or piercing. Foreign bodies can be inert or irritating to the body. If irritant, they are capable of promoting inflammation, secondary infection, abscess formation in addition to pain and discomfort. Therefore, identifying it is crucial.2
Symptoms related to accidents with stingrays can have traumatic origin – resulting from the penetration of the stinger, which has a serrated shape – or toxic origin – secondary to the poison produced by glandular structures on its tail.3 In the present case, the patient did not have systemic manifestations suggestive of poisoning and only realized something was wrong 2 months after the accident with the stinger. Therefore, there was not certainty about the presence of a FB in the foot, which is the most commonly affected site by this type of accident, according to the literature. The penetration of the stinger occurred in the dorsum of the left foot, and the symptoms were felt in the ventral face of the third left toe.
Different diagnostic imaging methods are used to identify the presence of FB – which, depending on their nature, can be radiopaque or radiolucent – in soft tissues. Magnetic resonance imaging appears to be the less indicated technique, since most of the FBs have materials with low signal to that kind of technology, entailing that they might be mistaken with calcifications, and scars or tendons. Moreover, metallic materials can move due to the strong magnetic field.4 A study comparing the effectiveness of CT and ultrasonography (USG) for identifying FBs composed by different materials have shown that USG has the best accuracy with radiolucent materials and when they are located on the skin’s surface. 2, 5
Ultrasonography is a painless and non-radioactive imaging based diagnostic method which is based on the reflection of sound waves through the tissues. According to the anatomical structure, vascularization and density, the ultrasonic waves are reflected back to the transducer, which translates them into a scale of gray that can be observed on a monitor. The higher the frequency of the waves emitted by the transducer, the greater the spatial resolution and resulting visualization of structures close to it. The introduction of transducers with frequencies higher than 15 MHz gave rise to the high frequency ultrasound (HFUS). The shorter wavelength obtained with this frequency allowed better evaluation of superficial structures, meaning their use in dermatological disorders significantly increased.6
Devices with frequencies higher than 15MHz allow the analysis of the skin and its appendages, as they are capable of distinguishing the cutaneous layers and structures. Nevertheless, devices with frequencies higher than 20 MHz offer the best resolution for studying superficial structures.6 In this manner, HFUS allows a better visualization of the FB located in soft parts, yielding information that is useful for their removal (e.g. as exact location, shape and composition) and providing a detailed analysis of the tissue and adjacent structures.
Ultrasonographically, most of the FBs are seen as hyperechogenic structures with a posterior acoustic shadow. Depending on the duration of its permanence in the tissue, it is possible to observe the presence of a hypoechoic area around the FB, that can possibly correspond to edema, abscess or granulation tissue.5 Foreign bodies made of wood are initially hyperechogenic, however can lose their echogenicity over time. 4 Stones arise as hyperechogenic areas with the presence of posterior acoustic shadow, while metals and glasses are hyperechoic and present, as an artifact, reverberation. 2 Foreign bodies that are rich in calcium, as in the case described in the present article, are hyperechogenic.
Ultrasonography allows three-dimensional access (longitudinal axis X transversal axis x depth) to the FB in addition to being an examination carried out in real time, 5 enabling the acquisition of anatomical knowledge of the affected area and exact location of the FB, allowing the surgeon to precisely remove it, minimizing the damage to vital structures, such as nerves and vessels.
The sensitivity to and specificity of HFUS are limitations of the method, and just like as those of other imaging based diagnostic methods, depend on several factors, such as the FB’s composition, size and location, the transducer’s frequency, the image’s resolution and the examiner’s experience.
The authors of the present article conclude that, despite the limitations described, HFUS is a useful method in the screening of FBs located on the surface of the human body, allowing detection and acquisition of knowledge related to their composition and exact location. This analysis provides important parameters to guide the surgical approach.
Elisa de Oliveira Barcaui:
Bibliographic research and drafting of the manuscript
Carlos Batista Barcaui:
Bibliographic research, drafting and review of the manuscript
Antonio Carlos Carvalho:
Review of the manuscript
1. 1 Hill R, Conron R, Greissinger P, Heller M. Ultrasound for the detection of foreign bodies in human tissue. Ann Emerg Med. 1997;29(3):353-56.
2. 2 Haghnegahdar A, Shakibafard A, Khosravifard N. Comparison between computed tomography and ultrasonography in detecting foreign bodies regarding their composition and depth: an in vitro study. J Dent Shiraz Univ Med Sci. 2016;17(3):177-84.
3. 3 Haddad V Jr, Lupi O, Lonza JP, Tyring SK. Tropical dermatology: marine and aquatic dermatology. J Am Acad Dermatol; 2009;61(5):733-50.
4. 4 Hiremath R, Reddy H, Ibrahim J, Haritha CH, Shah RS. Soft tissue foreign body: utility of high resolution ultrasonography. J Clin Diagn Res. 2017;11(7):TC14-TC16.
5. 5 Varshney T, Kwan CW, Fischer JW, Abo A. Emergency point-of-care ultrasound diagnosis of retained soft tissue foreign bodies in the pediatric emergency departament. Pediatr Emerg Care. 2017;33(6):434-6.
6. 6 Barcaui EO, Carvalho ACP, Lopes FPPL, Piñeiro-Maceira J, Barcaui CB. Ultrassom de alta frequência associado ao Doppler colorido na dermatologia. An Bras Dermatol. 2016;91(3):262-73.
This study was conducted at the Universidade Federal do Rio de Janeiro and at the Universidade do Estado do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}