


Douglas Haddad Filho1; José Victor Siervo2; Juliana Nascimento Brunhara3; Erika Leide da Silva3; Luiza Vieites3
The use of skin flaps for covering lesions is a better option than skin grafts, due to the diversity of the receptor area after the tumor’s resection and the greater degree of safety. For better results, the lesion’s location and extent, as well as the safety of the vascularization, should also be taken into account. Three resections were performed, with different coverage techniques. The patients had excellent development, without necrosis or dehiscence.
Keywords: RECONSTRUCTIVE SURGICAL PROCEDURES; SURGICAL FLAPS; FREE TISSUE FLAPS; PLASTIC SURGERY; SKIN DISEASES
Leg lesions may arise from diverse etiologies, from traumatic to infectious, and even neoplastic. They may present as superficial or deep, with muscle and/or bone involvement, where severe infections may exist. Depending on the etiology, the evolution, the type of lesion and the anatomical characteristics of the leg, different reconstructions are proposed, with different structures involved, such as muscles, fascia, septum and skin, or a combination.1 The site and size of the lesion are also important factors when considering the reconstruction. Due to the superficial anatomical vascular characteristic of the leg, where a great part of blood distribution occurs through musculocutaneous perforating vessels originating from deep vessels, the cutaneous flaps used for reconstruction in this region are based on the areas vascularized by this type of vessels.2
The incidence of skin cancer has been increasing over the last decades. The chances of developing skin cancer during a person’s life is multifactorial, for instance due to sun exposure, skin type and phenotype, and family history.3 Skin cancers have a higher incidence in areas that are more exposed to the sun, and are represented by the basal cell carcinoma, squamous cell carcinoma and melanoma. Basal cell carcinomas account for 65% of all epithelial neoplasias, the face being the most affected area. In turn, the squamous cell carcinoma represents 15% of all epithelial neoplasias, with 64% of them also present in the face.4, 5 Melanomas have an incidence of 3% to 4%, accounting for the smallest among skin tumors. However, they present the highest mortality rate among all skin tumors.6
The objective of this article was to present alternatives to skin flaps for cutaneous lesions in lower limbs.
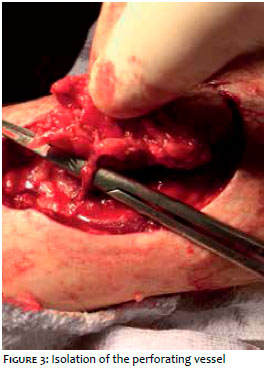
Three tumors were resected in three patients, using different coverage techniques. The options for cutaneous leg flaps are: circular rotation flap (small rotating arc), circular rotation flap (large rotating arc) and rectangular rotation flap. These options will be detailed below. In the first case, the skin tumor was located in the medial region of the lower third of the right leg, presenting 2.5cm in diameter, with clinical aspect compatible with basal cell carcinoma. In this patient the first option was chosen: circular rotation flap (small rotation arc). The tumor was marked [taking into consideration safety margins, and the planned skin flap to be performed (Figure 1). After the circular removal of the tumor, the rotation flap was designed, starting circularly on the lateral side of the tumor’s perimeter, and extending cranially in the form of a hook, as a flap diameter similar to that of the tumor (Figure 2). A musculocutaneous perforating vessel (Figure 3) made it possible to mobilize the flap, even with a small arc of rotation. The donor area was then closed (Figure 4) after adjustment and release of the surrounding tissues.
In the second case, the skin tumor was located on the lateral posterior side of the right leg, presenting a 5cm diameter and clinical aspect compatible with basal cell carcinoma. The second option was chosen for this patient: circular rotation flap (large rotation arc). The surgical marking took into consideration safety margins and the cutaneous flap to be performed (Figure 5). After the circular removal of the tumor, the rotation flap was performed (Figure 6). It started circularly at the most distal area of the tumor perimeter and was extended cranially, with a diameter greater than that of the tumor. Its vascularization was based on a musculocutaneous artery. Due to the size and shape of the flap, it was easily and safely mobilized toward the receiving area. The primary closure of the donor area was performed after adjustments and release of the surrounding tissues (Figure 7).
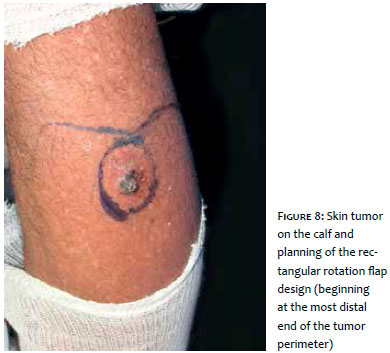
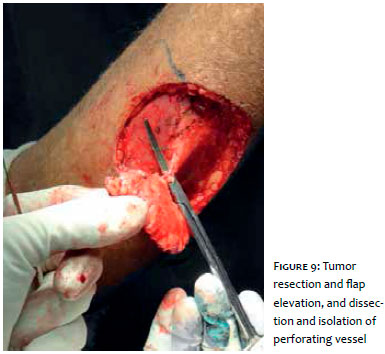
In the third case, the tumor was located in the mid-third of the right leg, on the posterior face, presenting 3cm in diameter, with clinical aspect compatible with basal cell carcinoma. In this patient the third flap option was chosen: the rectangular rotation flap. The tumor was marked taking into consideration safety margins, and the cutaneous flap to be performed (Figure 8). After circular removal of the tumor, the rectangular flap was designed, starting rectangularly at the distal extremity of the tumor perimeter, and extending 4cm laterally and 5cm cranially, with measurements larger than those of the tumor. Its vascularization was based on a musculocutaneous artery (Figure 9). Due to the shape of the flap, it was mobilized easily and safely towards the recipient area. The primary closure of the donor area was performed after adjustments and release of the surrounding tissues (Figure 10).
The option of using the skin flap to cover the recipient area overlaps the use of the skin graft, since the latter is a thin and often vulnerable cover, especially when localized on the bone tissue. In addition, for good graft integration, a homogeneous receptor area is needed, different from that found after the resection of tumors.7 The flap transfer should take into consideration the location of the lesion: whether on the anterior or posterior side of the leg. The amount of skin on the anterior face, that is, on the pretibial area, is smaller than that on the calf, which means increased difficulty in rotating the flap and/or closing the donor area. The inclusion of the regional perforating vessel in the flap, regardless of its design, means a safe vascularization.8 Its inclusion, however, must be planned prior to surgery, either by anatomical knowledge or by locating it through a vascular Doppler test.2 The latter is more frequently used when the flap is mobilized in a helical form.9 The planning of a flap at the lower extremity without the location of the perforator does not impair its use, but limits its extension and the arc of rotation, which becomes more vulnerable to tension and eventual necrosis. Cutaneous flaps used in superficial reconstructions of the lower limb may vary in size depending on the size of the lesion. Sometimes, depending on the location of the lesion, the amount of skin may not suffice to cover the recipient area and to close the donor area. Thus, skin grafts can be used in the donor areas. In regard to the shape of the flap, it should be chosen according to the location of the reconstruction.2 The circular flaps have the advantage of being able to be rotated bilaterally, if necessary. The rotation of the skin flap that is based distally, however, leads to an increased risk of necrosis, especially in the most distal area of the leg.
The options presented for skin flaps for the leg are safe and easy to perform, being that circular flaps may be added with additional opposing flaps when necessary.
Douglas Haddad Filho:
Conception and planning of the study. Effective partici pation in the orientation of the research. Elaboration and final revision of the manuscript
José Victor Siervo:
Drafting and revision of the manuscript
Juliana Nascimento Brunhara:
Drafting of the manuscript and bibliographic review
Erika Leide da Silva:
Drafting of the manuscript and bibliographic review
1. Mathes SJ, Nahai F. Leg. In: Livingstone C, editor. Reconstructive Surgery: Principles, Anatomy and Technique. Vol. 2. New York: Quality Medical Publishing; 1997. p. 1317-1512.
2. Geddes CR, Tang M, Yang D, Morris SF. Anatomy of the integument of the lower extremity. In: Blondeel PN, Morris SF, Hollock GG, Neligan PC, Publishing QM, editors. Perfurator flaps: Anatomy, Techinique and Clinical Applications. 2nd ed. Vol. 2. St Louis: Quality Medical Publishing; 2013. p. 668-703.
3. Lages RB, Barbosa PB, Almeida IP, Lopes LRS, Lopes Filho LL. Detecção precoce do câncer de pele: experiência de campanha de prevenção no Piauí- Brasil. Rev Bras Promoç Saúde. 2012;25(2):221-7.
4. Albert RE. In: Andrade R, Gumport SL, Popkin GL, Rees H,editors. Cancer of the skin: Biology. Diagnosis and management. Philadelphia: Saunders; 1976. p. 111-156.
5. Allen AC. The skin: A Clinicopatohologic Treatise. 2 nd ed. Orlando: Grune and Stratton; 1967.
6. Rizzatti K, Schneider IJC, d'Orsi E. Perfil epidemiológico dos cidadãos de Florianópolis quanto à exposição solar. Epidemiol Serv Saúde. 2011;20(4):459-69.
7. Kamrin BB. Analysis of the union between host and graft in the albino rat. Plast Reconstr Surg Transplant Bull. 1961;28:221-6.
8. Timmons MJ. Landmarks in the anatomical study of the blood supply of the skin. Br J Plast Surg. 1985;38(2):197-207.
9. Hyakusoku H, Yamamoto T, Fumiiri M. The propeller flap method. Br J Plast Surg. 1991;44(1):53-54.
This study was conducted at the Universidade Santo Amaro (Unisa) - SãoPaulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}