


Valéria Barreto Campos1; Juliana Merheb Jordão2; Valéria Romero3; Célia Luiza Kalil4
Introduction: Currently there is a growing demand for non-invasive therapies aimed at treating facial aging. Non-ablative fractional lasers lead to excellent outcomes, with reduced side effects. Objective: To evaluate the facial rejuvenation achieved by 1,340nm non-ablative fractional laser using a single pass at high energy versus three passes at medium energy, through a prospective comparative study. Methods: Twenty patients with facial aging were treated with 2 or 3 laser sessions with 4-week intervals. The right hemiface was treated with three passes of 1,340nm non-ablative fractional laser at a fluence of 90 mJ, pulse duration of 5ms and 100 mtz/ cm2. The left hemiface was treated with a single pass of the same laser at a fluence of 120 mJ, pulse duration of 5ms and 100 mtz/cm2. The evaluated variables were spots, wrinkles, porphyrins and overall appearance. Results: The patients (n = 20) were evaluated during 6 to 24 months. The photographic evaluations demonstrated a significant improvement of the spots on the right hand side and wrinkles on the right and left hand sides. Eighteen of the 20 patients reported satisfaction with the treatment. Conclusion: 1,340nm non-ablative fractional laser was proven as a modern, safe and effective alternative for facial rejuvenation. For spots, the triple passes at medium energy protocol led to a superior response. However, regarding wrinkles there was no difference between the single pass at high energy and triple pass at medium energy protocols.
Keywords: LASER; REJUVENATION; FACIAL AGING; FACE
The rejuvenating techniques have been perfected not only due to technological advances, but also due to the concern of the population with health and physical appearance, as well as longevity.1 Some studies suggest that the facial changes due to aging begin at around 30 years of age2 and are clearly noticed from 40 years of age, when there is a reduction in the estrogen levels and collagen fibers, making the skin thinner and more sensitive, with pigment changes and the appearance of wrinkles, telangiectasias and lentigos. The formation of wrinkles, irregularities, reduction of elasticity and firmness of the facial skin are the most expressive signs of the biologic age.3 In chronological aging, the thickness of the dermis reduces due to biochemical and structural changes of the collagen and elastic fibers, as well as the ground substance.4,5 There is reduction in the production of collagen and increased degradation due to the elevated levels of collagenase. The cutaneous amount of collagen reduces 1% per year on average throughout adulthood, beginning between 30 and 40 years of age in women and somewhat later, between 40 and 50 years in men. Remaining collagen fibers are disorganized, more compact and fragmented. Elastic fibers are reduced in number and diameter. The amount of mucopolysaccharides in the ground substance is reduced, especially hyaluronic acid. These changes have a negative influence on the skin turgor and the collagen.6 Skin aging is a natural and multifactorial process that results in cutaneous deterioration, sagging and wrinkles. The extension of aging is determined by factor related to genetics, skin pigmentation and thickness, as well as external factors, such as sun exposure, smoking and quality of nutrition.7,8
The conservation of youth was always fascinating and there has been an increase in demand for non-invasive treatments to control facial aging.9 Some people invest time and money in rejuvenation techniques, many of which do not have their efficacy proven.10 According to survey by the American Society for Dermatologic Surgery in 2014, around 150 thousand laser resurfacing procedures were performed. More directed studies are needed with each device to try to evaluate the role of different parameters and their standardization.11
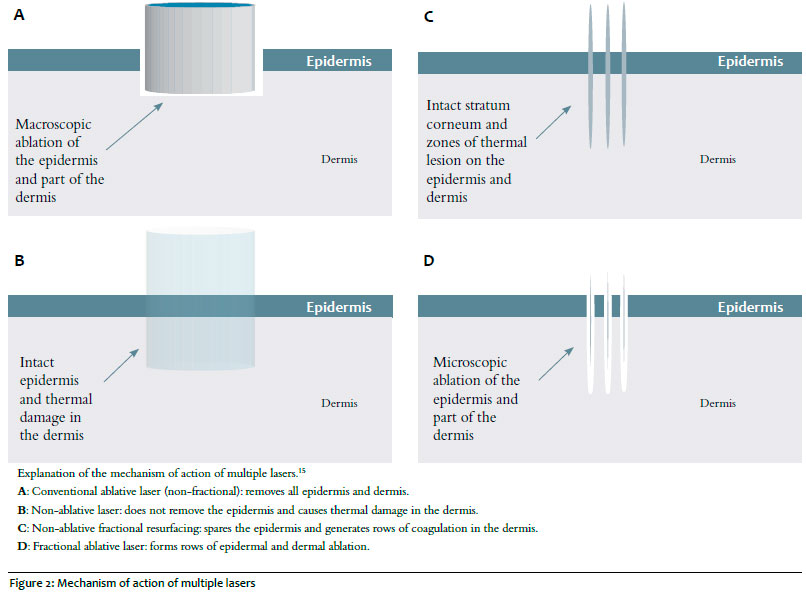
Cutaneous laser rejuvenation has shorter operation and recovery times, with more natural result when compared to traditional surgery.12,13 Non-ablative lasers and other sources of electromagnetic energy represent the new approaches to improve photoaged skin. Since the degree of collagen remodeling is not as high as seen with other techniques, that are more destructive and ablative, the non-ablative technique is appropriate for the treatment of persons who aim at improving the quality of their skin, with no downtime.14 The main indication for the non-ablative fractional laser is mild to moderate photoaging, because the neocollagenesis with this technique is limited. Removal of epidermal and superficial dermal pigmentation is a second indication.15 For decades, devices and peels were used for facial rejuvenation and for the treatment of skin damage. In the last few years, new laser systems were developed, including ablative and non-ablative fractional, that can provide good results with less side effects.16 Non-ablative rejuvenation uses laser to improve the skin appearance and reduce the number of wrinkles, blemishes and scars by generating heat in the dermis, keeping the epidermis intact. The fractional approach allows the skin to recover much quicker than the non-fractional. This approach reduces recovery time and the number of possible complications. In most cases, multiple sessions are needed.17
The objective of the present study was to evaluate and compare facial rejuvenation with non-ablative fractional laser (LFNA) 1340nm with a single pass and high energy to triple pass and medium energy.
For this clinical, prospective, single-center and comparative study, 20 female patients, aged 40 to 70 years, Fitzpatrick phototypes I to IV and Glocau’s aging index of moderate to severe were recruited from the Dermatology Outpatient clinic of the Faculdade de Medicina de Jundiaí (SP). It was conducted in accordance to the Helsinki Declaration and according to the CNS Resolution n. 466/12 of the Anvisa, according to Good Clinical Practice (Document of the Americas and ICH E6: Good Clinical Practice). The patients were informed about the objective, methodology, duration, advantages and clinical restrictions related to the study. The participants confirmed their interest, signing a consent form. Technical documentation of this study will be kept in file for five years.
Exclusion criteria were infection on the site to be treated, history of keloid scarring, known connective tissue or autoimmune diseases Raynaud phenomenon or circulation changes, pregnancy or lactation, presence of suspicious lesion for malignancy on dermoscopy, history of allergy to anesthetics agents and unrealistic expectations for the treatment.
All patients were prepared for the treatment with the application of topical anesthetic with lidocaine 4%, 30 minutes before the session. Fifteen patients had three laser sessions for the face and other five patients, due to scheduling problems, had two sessions, 4 weeks apart. The treatment platform used was ETHEREA-MX® (VYDENCE Medical®, São Carlos, SP, Brazil), and its handpiece ProoDeep – non-ablative fractional laser Nd:YAP (Neodimiun:Ytrium Aluminum Peroviskita) of 1340nm. The right side of the face was treated with LFNA 1340nm with the fluence of 90mJ, pulse duration of 5’, 100mtz/ cm2, three passes and skin cooling with the device SIBERIAN (VYDENCE Medical®, São Carlos, SP, Brazil) for comfort during and after the procedure. The left side of the face was treated with LFNA 1340nm with the fluence of 120mJ, pulse duration of 5’, 100mtz/cm2, single pass and cooling identical to the other side of the face.
The patients received instructions to avoid topical agents on the treated area for the duration of the study and to report adverse cutaneous or systemic reaction after laser. They were contacted between 6 and 24 months after the last session. Clinical efficacy of the treatment was performed by three blinded dermatologists, through photographic analysis before and after the treatment. Besides analyzing the photographs, the results were evaluated with the device Visia. The parameters used for the clinical evaluation before and after the treatment were: blemishes, wrinkles and porphyrins.
After the procedure, the patients were advised to avoid sun exposure and use sunscreen daily on the treated area, with a large UVA and UVB protection spectrum (solar protection factor 50), until fully recovered. Besides, they were advised to avoid contact with substances that could irritate ou sensitize the area in the first week after the procedure.
The statistical analysis of the results was performed using the software Grafhpad Prism 7. Scores of 0 to 4 were created to evaluate and grade the improvement, with 0 corresponding to the category “None”, 1 to the category “Little”, 2 to the category “Medium”, 3 to the category “Large” and 4 to the category “Excellent”. The quantitative variables were described by the mean and standard deviation and compared by the Student T test for matched samples. We considered the significance level of 5%.
The patients (n = 20) were assessed in a period of 6 to 24 months between the first treatment and the last clinical assessment. Upon examination of the results of the photographical analysis (Figure 1), evaluated and quantified the parameters blemishes, wrinkles and porphyrins, before and after the treatment, with the device Vísia, there was a statistically significant improvement of the blemishes on the right side of the face (p < 0.05 Student t test), wrinkles on the right and left sides (p < 0.05 Student t test). Regarding porphyrins, there was no statistically significant improvement (p > 0.05, Student t test). The photographic analysis demonstrated treatment efficacy and the possibility of reaching a unique benefit in a short time. Figure 1 illustrates wrinkle improvement on both sides of the face.
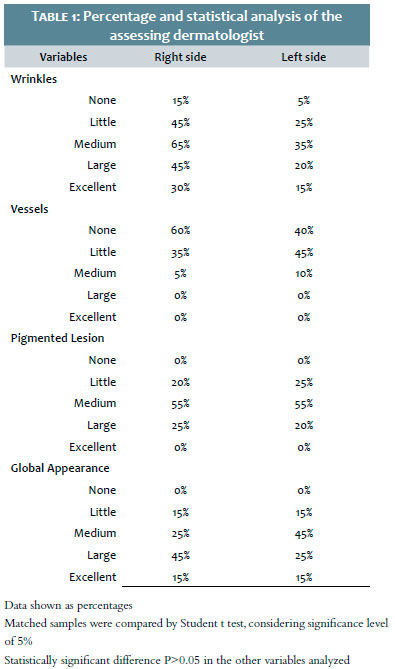
In the evaluation of the percentage and statistical results performed by the blinded dermatologists (A1,A2 and A3) (Table 1), we observe the statistically significant clinical efficacy of the wrinkle treatment tratamento by examiner 1 (A1). Regarding the assessment of the other examiners, there was no statistically significant difference between matched samples (p > 0.05).
Global rejuvenation (global appearance), analyzed in percentages, showed that the variables “Large” and “Excellent” were higher. In the subjective evaluation of the patients, 90% (18/20 patients) demonstrated a higher satisfaction rate with the treatment given. The level of satisfaction was evident after 30 days of the first reassessment, before the second session, with the manifestation of interest to continue the treatment. The patients reported improvement on the skin for up to 6 months after the last session.
The side effects reported were erythema and edema immediately after the session, with similar intensity on both sides of the face, that disappeared spontaneously in the first 48 hours; no other side effect was seen after that.
Innovative treatments for facial rejuvenation are in constant evolution, in particular with the use of non-ablative laser. However, no studies were published on its efficacy or the specifications of Nd:YAP 1340nm laser for this indication.
Inevitable changes occur on the skin with chronologic aging, including loss of elasticity, texture and color changes.18 The modification of the thickness of the dermis occur via biochemical and structural changes in the collagen and elastic fibers and in the ground substance, with reduction of the collagen synthesis and increased degradation due to the elevation in the levels of collagenase The elastic fibers are reduced in number and diameter, and the amount of mucopolysaccharides in the ground substance is also reduced, and of the hyaluronic acid in particular, which influences negatively the skin turgor and also on the deposition, direction and size of collagen fibers.19
The market of non-surgical, energy-based facial rejuvenation techniques increased exponentially since lasers were first used for this indication. The advance is this area lead to a wide range of products that demand a great repertoire of knowledge from the modern doctor.20 Since the advent of high potency pulsed ablative carbon dioxide laser for the reduction of wrinkles and treatment of photoaging in the mid-1990s, laser resurfacing became the standard treatment for rejuvenation of facial skin. In the beginning, this technique was popular. Even though the results are impressive, the discomfort, the prolonged recovery and the high risk for complications lead to patient dissatisfaction and it became gradually less popular. Although this laser continues to be the treatment of choice for the skin with severe photoaging, the use of non-ablative laser also imporves lines and wrinkles in mild to moderate aged skin, with a minimal risk of complications and without the downtime associated to ablative laser techniques. With the advances in laser technology, multiple non-ablative lasers for facial rejuvenation became available. The results of the treatment with these devices were reported by various researchers.21,22
In the present study, high-energy 1340nm non-ablative fractional laser with a single pass and medium energy with a triple pass proved to be an effective treatment for facial rejuvenation. There was a slight overall improvement, with an obvious global rejuvenation, not as dramatic as what is seen with ablative laser treatment.23,24 None of the patients in this study reported any side effect after 48 hours of treatment.
Non-ablative fractional laser rays generate rows of coagulation in the skin, maintaining an intact, non-ablated epidermis (Figure 2). In this row, there is a process of reconstitution of all the area that was coagulated, from the dermis to the epidermis, after a few hours and with months’ duration. Collagen and fractions of pigment and vessels that were coagulated are slowly eliminated through the epidermis.15 The penetration of the rays varies depending on the fluence. The literature shows that the higher the energy released, the deeper the action and the greater the neocollagenesis, allowing for a modulation of the desired result.25 In this study, the use of higher energies with a single pass was not more effective in the reduction of wrinkles than the treatment with medium energy and three passes.
Despite the fact that melanin and hemoglobin are not the targets of this lasers, the ray row coagulates part of pigments and/ or vessels that are reached by it upon penetration in the skin. Thus, even indirectly, there is removal of superficial epidermal and dermal pigments and also of some smaller blood vessels. There was no significant reduction of the vessels. Regarding lentigos, the side treated with a triple pass and medium energy had a higher reduction than the side treated with a single pass and higher energies. This is the first study of the use of Nd:YAP 1340nm laser for facial rejuvenation, so more studies are needed to compare with the efficacy of other well-established lasers.
Even with a small number of patients in this clinical study, the treatment with 1340nm non-ablative fractional laser with high energy and single pass versus medium energy and three passes proved to be safe and effective for facial rejuvenation, becoming an alternative for the face. The technique of triple pass and medium energy showed a better reduction in lentigos than the single pass with higher energies; however, there was no difference regarding the reduction of wrinkles with the two techniques. An approach with the identification of the degree of aging will certainly improve the efficacy of the treatment, possibly achieving even better results. The proposed treatment ended with satisfied patients, who had more beautiful skin and a younger look.
We thank VYDENCE MEDICAL® for the support with the platform ETHEREA-MX®, fundamental for this study.
To Camila Bonati Mattos, Cyntia Simonetti, Fernanda de Mattos Pereira Barucci, Josinete da Silva, Karina Infanti, Lidiane Terron, Lucimara Bingazzolli and Thaís Bologna Flora, for helping in the execution.
Valéria Barreto Campos:
Substantial contribution for study conception and de sign; Data analysis and interpretation. Approval of the final version for publication.
Juliana Merheb Jordão:
Substantial contribution for study conception and de sign; Data collection and interpretation.
Valéria Romero:
Approval of the final version for publication. Contribu tion for the data conception, analysis and interpretation.
Célia Luíza Kalil:
Substantial contribution for study conception and de sign; Data analysis and interpretation. Approval of the final version for publication.
1. Velasco MVR, Ribeiro ME, Bedin V, Okubo FR, Steine D. (2004). Rejuvenescimento da pele por peeling químico: enfoque no peeling de fenol Facial skin rejuvenation by chemical peeling: focus on phenol peeling. An Bras Dermatol. 2004; 79(1), 91-99.
2. Souza CB, Guerra JG, Barbosa MA, Porto CC. Rejuvenescimento facial por intervenção miofuncional estética: revisão integrativa. Med Cutan Iber Lat Am. 2013; 41(4):165-71.
3. Giacomini PO, Rein R. A mechanistic model for the aging of human skin. Micron 2004; (35): 179-84.
4. Fisher GJ, Varani J, Voorhees JJ. Looking older: fibroblast collapse andtherapeutic implications. Arch Dermatol. 2008; 144(5):666-72.
5. Quan T, Fisher GJ. Role of age-associated alterations of the dermal extracellular matrix microenvironment in human skin aging: A Mini-Review. Gerontology. 2015;61(5):427-34.
6. Yaar M, Gilchrest B. Aging of skin. In: Fitzpatrick's dermatology in general medicine. 7th ed. New York : McGraw-Hill Medical; 2008. p. 963-73.
7. Jansma J, Schepers RH, Schouten HJ, Vissink A. Blepharoplasty in aesthetic facial surgery. Ned Tijdschr Tandheelkd 2014; 121:395–400.
8. Shehzad A, Mian A, Shah S. Skin aging. Journal of Pakistan Association of Dermatology. 2016; 21(2):77-79.
9. Fitzpatrick RE, Rostan EF. Reversal of photodamage with topical growth factors: a pilot study. J. Cosmet. Laser Ther. 2003; 5(1), 25–34.
10. Zouboulis CC, Makrantonaki E. Clinical aspects and molecular diagnostics of skin aging. Clin. Dermatol. 2011; 29(1): 3–14.
11. Motta MM. Avaliação histológica e morfológica da pele de ratos adultos submetidos à ação de um laser de CO2 fracionado aplicado com três diferentes parâmetros. 2016. (s.n.).
12. Jindal K, Sarcia M, Codner MA. Functional considerations in aesthetic eyelid surgery. Plast Reconstr Surg. 2014; 134(6): 1154–70.
13. Zoumalan CI, Roostaeian J. Simplifying blepharoplasty. Plast Reconstr Surg. 2016; 137(1):196–213.
14. Goldberg DJ. Lasers for facial rejuvenation. Am j clin dermatol. 2003; 4(4); 225-34.
15. Campos V, Mattos R A D, Fillippo A, Torezan LA. Laser no rejuvenescimento facial. Surg Cosmet Dermatol. 2009; 1(1): 29-36.
16. Zachary CB. Facial Rejuvenation: 40th Anniversary Review. Semin Cutan Med Surg. 2016; 35(6 Suppl): S122-24.
17. ASDS – American Society for Dermatologic Surgery. Non-ablative Laser Rejuvenation. [Internet]. 2016. Acesso em 12 de julho de 2017. Disponível em: https://www.asds.net/_PublicResources.aspx?id=8215&terms= rejuvenation%20and%20laser
18. Fitzgerald R, Vleggaar D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatol Ther. 2011; 24(1):2-27.
19. Varani J, Dame MK, Rittie L, Fligiel SE, Kang S, Fisher GJ, Voorhees JJ. Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am J Pathol. 2006; 168(6):1861-8.
20. Britt C J, Marcus B. Energy-Based Facial Rejuvenation: Advances in Diagnosis and Treatment. JAMA facial plast surg. 2017;19(1); 64-71.
21. Trelles MA, Allones I, Luna R. Facial rejuvenation with a non-ablative 1320nm Nd:YAG laser. Dermatol Surg.2001;27(2):111-16.
22. Fournier N, Dahan S, Barneon G, Diridollou S, Lagarde J M, Gall Y, et al. Nonablative remodeling: clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540 nm Er: glass laser. Dermatol Surg. 2001; 27(9):799- 806.
23. Ross E, Victor M, Joseph R. Anderson R. Why does carbon dioxide resurfacing work?: a review. Arch Dermatol. 1999; 135(4): 444-54.
24. Alster TS, Lupton JR. An overview of cutaneous laser resurfacing. Clin Plast Surg. 2001; 28(1): 2837- 52.
25. Walgrave S, Zelickson B, Childs J, Altshuler G, Erofeev A, Yaroslavsky I, et al. Pilot investigation of the correlation between histological and clinical effects of infrared. Dermatol Surg. 2008; 34(11):1443-53
Study conducted at Faculdade de Medicina de Jundiaí - Jundiaí (SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}