


Fernanda Aquino Cavallieri1; Laila Klotz de Almeida Balassiano2; Julien Totti de Bastos3; Gabriela Helena Munhoz da Fontoura4; Ada Trindade de Almeida5
Introduction: The use of hyaluronic acid fillers (HA) for esthetic corrections has exponentially grown in recent years. Skin ultrasound (US) is an effective method to identify the filler and its complications. A particular type of adverse effect, characterized by late, persistent edema of an intermittent nature, has been lately observed. Objective: To describe a delayed complication due to easy HA fillers, named by the authors as Persistent, Intermitent Delayed Swelling (PIDS). Methods: From October 2016 to July 2017, US examinations performed at Cavallieri Clinic were selected and referred for evaluation of post-filler complications. Questionnaires were sent to requesting physicians for clinical data collection. Results: Of 108 exams, 33 cases of local subcutaneous edema associated with the presence of HA fillers were identified. Episodes of edema were referred to as recurrent, in the previously affected area, or at another injection site. Conclusion: The authors propose a specific nomenclature: PIDS to refer to this late adverse reaction to HA fillers, which includes delayed and intermittent local swelling, triggered by specific conditions, that persists for as long the HA remains in the subcutaneous tissue.
Keywords: DERMAL FILLERS; HYALURONIC ACID; ADVERSE EFFECTS; SKIN ULTRASOUND
The use of fillers, particularly of hyaluronic acid (HA), for facial aesthetic corrections increased exponentially over the last few years. Skin ultrasound (US) has been shown to be an effective method for the evaluation of the substance injected, as well as its complications.The technique is useful because it is not invasive, provides a good balance between penetration and image resolution, enables distinction of the different skin layers and presents no risk or discomfort for the patient, nor radiologic exposure, use of contrasts ou confinement in small spaces.
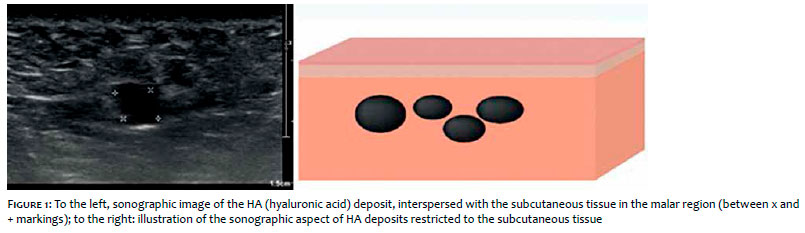
According to Ximena et al1, the sonographic appearance of injected HA has a round or oval-shape, well-defined, anechoic (black) structure, known as “pseudocyst” because of its resemblance with true cysts (Figure 1). HA formulations that are mixed with lidocaine present with interspersed echoes (debris inside the pseudocysts). Polymethylmethacrylate (PMMA) has the sonographic aspect of multiple hyperechoic deposits (white), that cause a mini-artefact shaped like a comet tail, corresponding to the posterior reverberation. Because calcium hydroxyapatite is a compound of microspheres suspended in a lipopolysaccharide carrier, it is identified by hyperechoic deposits with variable degrees of acoustic shadow. Silicone oil appears as a strongly echogenic image in the subcutaneous tissue, determining a strong posterior acoustic shadow in a snowstorm pattern. The sonographic aspect of polyacrylamide gel is of an anechoic, ovalshaped pseudocyst with hyperechoic lines (white), that does not change in volume over time and that determines an enhancement of the echogenicity of the surrounding tissue.Autologous fat filler is visualized as an oval shaped, well-defined, isoechoic (similar to the fat in the adjacent subcutaneous tissue) nodularity, sometimes with minute interspersed anechoic areas. Polylactic acid usually has no sonographic expression, except in cases where the product acquires a nodular aspect and becomes clinically palpable, when it is visualized on ultrasound as a well-defined isoechoic image.
Regarding the complications caused by fillers, US can identify the filler substance, determine its dimensions and location, and evaluate local vasculature with color Doppler. Ultrasound images differ from inflammatory and/or infectious processes, overcorrections and changes consistent with necrosis of the subcutaneous tissue. The test can also help in guiding aspiration biopsies and hyaluronidase and/or corticosteroid injections.1-3
Recently, a particular type of complication that evolves with delayed, recurrent and persistent facial edema, corresponding to the injection site, drew the authors’ attention for being the reason for frequent requests for facial soft tissue ultrasound examination.The intention to better clarify the clinical features of this type of complication lead the authors to conduct this study.
In the period from October 2016 to July 2017, all US performed at Clínica Cavallieri de Diagnóstico por Imagem, Rio de Janeiro (RJ), Brazil, referred for the evaluation of complications of facial fillers were selected. All patients underwent facial US, performed by a radiologist with a large experience in skin and soft tissue ultrasound.The device used was EPIQ7 (Philips Medical Systems,Bothell,WA, USA),with two high frequency transducers (7 to 15MHz and 5 to 18 Mhz).The exam included the study of the whole face in all patients, in B mode and with the association of Color Doppler for the assessment of local vasculature. After recording demographic and image data, the authors created a questionnaire that included questions about: commercial name of the HA used, application sites, time for the onset of symptoms, related events, treatment used, recurrence and duration of edema.The questionnaires were sent by e-mail to the referring doctors for clinical data collection.
In 108 ultrasound exams, performed for the evaluation of complications with fillers, 33 cases of subcutaneous edema associated to HA were seen, all of them in women between 29 and 71 years of age, (mean of 50 years). In 27 exams, HA was identified as the only filler; in six patients, besides HA, another substance was visualized, namely: polymethylmethacrylate (PMMA) in three exams, Poly-L-Lactic acid (PLLA) in one exam, autologous fat in one exam and polyacrylamide gel in one exam. Regarding the presence of the filler, the most affected site by edema was the malar region (15 cases), followed by the lower eyelid region (11), nasolabial fold (eight) and lip (two). Zygoma, chin, pre-jowl region, forehead and nose had one case each. Of the 33 affected patients, five presented with edema in different areas at the same time. Of the 33 patients, the exam was repeated in 12, due to recurrences either in the same site of injection or in other sites.
Among the sonographic findings, the common feature in all 33 cases was the presence of HA associated to a diffuse increase in the thickness and echogenicity of the surrounding subcutaneous tissue, sonographically similar to a diffuse, ill-defined panniculitis, corresponding to the area with clinical edema (Figure 2). No solid nodules or collections of liquid were seen in these patients, therefore ruling out other possible adverse reactions that are characterized by nodules, abscesses or collections. These edema episodes were referred as recurrent by the patients, occurring in the area previously affected or in another injection site. By the features of delayed edema after use of HA filler, intermittent and persistent in nature, all 33 patients were diagnosed as PIDS (persistent intermittent delayed swelling).
Of these 33 cases of PIDS, data of 20 patients were collected through questionnaires. PIDS was characterized clinically by non-pitting, erythematous or not, diffuse or not, ill or well-defined edemas along the area of HA injection. In all cases, accentuation of the edema was reported upon waking up, with slight improvement throughout the day.
The mean duration for each event was difficult to evaluate and varied considerably between patients; most of them were primarily treated with oral corticosteroids and/or antibiotics before being referred for ultrasound examination.The earliest case appeared 25 days after the injection, whereas the latest occurred three years after the procedure.Twelve patients had the onset of PIDS at the same time as an infectious process (sinusitis, urinary tract infection, respiratory tract infection, dental infection), trauma on the face or vaccination. In one case, the patient noted recurrences of the facial edema during menses. Of the products utilized, eight were identified: JuvedermVoluma® (seven cases), JuvedermVolbella® (seven cases), Juvederm Volift® (two cases), Juvederm Ultra (one case) Anteis Modelis® (one case), Restylane Perlane® (one case) and Emervel Classic® (one case). Medical management consisted in systemic antibiotic therapy (ATB) + hyaluronidase (two cases), ATB + systemic and/or intralesional corticosteroid (five cases),ATB + hyaluronidase + oral corticosteroid (five cases), hyaluronidase alone (two cases), oral ATB alone (two cases), oral corticosteroid alone (three cases). One patient did not receive any treatment and had spontaneous resolution.
Clinically recognized, the persistent intermittent delayed edema consists in recurrent episodes of local edema in the HA injection site, with short of long remission, with no evidence of defined palpable nodules. On the ultrasound, the presence of HA corresponding to the edematous area is seen, associated to a diffuse increase in the thickening and echogenicity of the subcutaneous tissue (panniculitis).
Ultrasound is a non-invasive imaging study, of easy access, that is being frequently used in dermatological practice. Ultrasound offers relevant information on adverse reactions of cosmetic fillers, being an important tool in cosmiatry for the better understanding of complications post-fillers.
Many HA complications have been described in the literature, however, each author classifies them according to their clinical experience because there is no consensus on the classification of these adverse reactions. Nonetheless, many articles describe a late adverse reaction similar to PIDS.
Callan et al4 reported a single case (1%) of “edema and hardening of the product” in the injected area in a 24-month study with 103 patients treated with Juvederm Voluma®.
Goodman5 also described a “firm and hardened, non-pitting edema, with no signs of infection or inflammation” in a patient treated with Juvederm Voluma®, 4 months after the procedure.
In a retrospective review of 4,702 treatments with Juvederm Voluma® in 2,342 patients, Beleznay et al6 described 23 cases (1%) of “firm nodules and local edema of late onset”.The time for the development of these nodules was of 4 months, with mean resolution after 6 weeks.
Artzi et al7 reported a series of 400 patients injected with Juvederm Volbella® in the lips and lower eyelids. Of those, 17 (4.25%) developed “change in color and edema in the treated area”, with 8 of these 17 patients having an association with other types of HA besides the Juvederm line.The mean time for onset was of 8 weeks.
In the above-mentioned articles, ultrasound was not used to characterize complications. Perez et al reported the use of US to evaluate one case of complication with HA filler.The patient had “indurated, palpable and asymptomatic lesions” in the marionette lines that appeared 4 months after the injection with Juvederm Voluma® and Juvederm Volift®. US demonstrated a focal subcutaneous area with enhanced echogenicity, suggestive of edema, and an increase vascularization of the area (panniculitis). The patient progressed with improvement of the lesion, but had recurrences in other areas of the face for up to 4 months after the first episode. All 33 cases evaluated in the present study resemble the case in Perez et al article, where HA was identified in areas that corresponded to the edema and associated to the subcutaneous tissue, with increased thickness and hyperechogenicity (signs of panniculitis).8
Of the five articles mentioned above, we highlight 43 cases of an edematous reaction after injection of HA fillers.Two of them were single cases (Goodman – Juvederm Voluma® and Perez – Juvederm Voluma® and Volift®). Two clinical studies were conducted with a single product and comprise 24 cases (Beleznay – Juvederm Voluma®; Callan – Juvederm Voluma®). Lastly, 17 cases came from private practices (Artzi). Contrary to what we found in the literature, with cases from controlled groups or private practices, the cases analyzed by the authors come from different sites, referred by dermatologists from their private practices to a radiology clinic, focused on ultrasound. Therefore, the statistics were collected at Clínica Cavallieri with varied patients from Rio de Janeiro metropolitan area, from a total of 30 referring dermatologists.
In the 20 cases where the performing physician reported the brand of HA,Vycross® line of fillers appeared in a higher number of cases (16) compared to other lines of HA fillers (four).The small number of cases where the filler was identified does not allow us to conclude a cause/effect relationship with a specific product line, since this could be the most used brand of filler.A higher number of cases would be required to reach a more accurate conclusion.
Vycross® technology is based in the incorporation of short and long strands of HA to provide a more effective reticulation. Published data suggest that high molecular weight HA strands are mainly anti-inflammatory, while the low molecular weight strands are pro-inflammatory, activating the immune system.9 It is possible that between three to five months after the injection, when the activation of late inflammatory nodules is more frequently observed, there is a more pronounced breakage of the HA, exposing low molecular weight fragments, that are pro-inflammatory. Even though products from the Juvederm Vycross® line have a higher proportion of low molecular weight particles, is not known if this proportion alone is more inflammatory in comparison to other products.
Regarding triggering factors, 12 patients (36%) associated the event to an infectious condition, and this data was close to what Beleznay described in his article, where 39% of patients reported a respiratory tract infection or a dental procedure before the appearance of the reactions.6
Given the spontaneous resolution of the nodules, their early onset, short duration and treatment response, including steroids and hyaluronidase, Beleznay et al defend the idea that these types of reactions seen with HA are more consistent with an immune-mediated etiology as opposed to biofilm, a commonly implicated mechanism in the literature.The opinion of those authors is that, when HA is injected into a predisposed individual, triggers such as respiratory tract infections, dental procedures, systemic bacterial or viral infections, vaccination and facial trauma could trigger an inflammatory process corresponding to the injected area, given the immunogenic nature of the filler, as well as its capacity of retaining water, configuring the local edema.10
In 2013, Alijotas et al selected 235 articles published on PubMed from 2000 to 2012 reporting fillers adverse reactions with the aim to report the various types of related adverse events. The results obtained from this review showed that most of the late effects are inflammatory or immunomediated in nature, and that factors such as systemic infections could act as a trigger for these complications.11
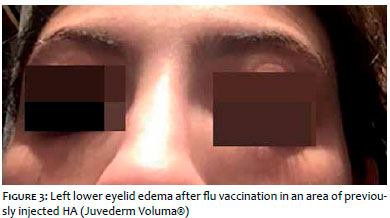
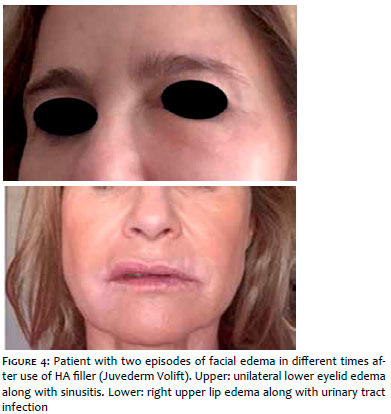
The data obtained suggest that PIDS is a manifestation that can occur after the use of HA facial fillers, clinically characterized as: late onset diffuse, non-pitting edema along the area of HA injection, (it can appear between week and years after HA injection), transient and intermittent and, mainly, persisting while there is HA in the tissue. It is frequently related to some trigger such as local trauma, vaccination (Figure 3) or more commonly after a local or systemic infectious process such as, for example, respiratory infection (Figure 4) or dental procedures, what could explain its intermittent nature.
The authors propose a specific nomenclature: persistent intermittent delayed edema (PIDS) to group late HA adverse reactions, characterized by late local intermittent edema, triggered by specific factors, that persists while there is HA in the tissue.
On US, the common finding is the presence of HA with signs of surrounding panniculitis (increased thickness and echogenicity of the subcutaneous tissue, correlating to the clinical aspect), and the absence of solid nodules or liquids. Since nodules cannot be identified on US, we suggest that PIDS have a specific classification in the group of HA late adverse reactions, commonly described as a group in the literature.
Fernanda Aquino Cavallieri:
Preparation and wording of the manuscript
Laila Klotz de Almeida Balassiano:
Preparation and wording of the manuscript
Julien Totti de Bastos:
Preparation and wording of the manuscript
Gabriela Helena Munhoz de Fontoura:
Preparation and wording of the manuscript
Ada Trindade de Almeida:
Supervision and final review of the manuscript
1. Wortsman X. Common applications of dermatologic sonography. J Ultrasound Med. 2012; 31(1):97-111.
2. Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GB. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venereol. 2012; 26(3):292-301.
3. Quezada-Gaón N, Wortsman X. Ultrasound-guided hyaluronidase injection in cosmetic complications. J Eur Acad Dermatol Venereol. 2016; 30(10):e39-e40.
4. Callan P, Goodman GJ, Carlisle I, Liew S, Muzikants P, Scamp T, et al. Efficacy and safety of a hyaluronic acid filler in subjects treated for correction of midface volume deficiency: a 24 month study. Clin Cosmet Investig Dermatol. 2013; 6:81-9.
5. Goodman GJ. An interesting reaction to a high- and low-molecular weight combination hyaluronic acid. Dermatol Surg. 2015; 41(Suppl 1): S164-6.
6. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015; 41(8):929-39.
7. Artzi O, Loizides C, Verner I, Landau M. Resistant and recurrent late reaction to hyaluronic acid-based gel. Dermatol Surg. 2016;42(1):31-7.
8. Pérez-Pérez L, García-Gavín J, Wortsman X, Santos-Briz Á. Delayed Adverse Subcutaneous Reaction to a New Family of Hyaluronic Acid Dermal Fillers With Clinical, Ultrasound, and Histologic Correlation. Dermatol Surg. 2017;43(4):605-8.
9. Baeva LF, Lyle DB, Rios M, Langone JJ, Lightfoote MM. Different molecular weigh hyaluronic acid effects on human macrophage interleukin 1 ß production. J Biomed Mater Res A. 2014;102(2):305-14.
10. Luebberding S, Alexiades-Armenakas M. Facial volume augmentation in 2014: overview of different filler options. J Drugs Dermatol. 2013; 12(12):1339-44.
11. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, imune- -mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241-58.
Study conducted at Hospital Federal da Lagoa - Rio de Janeiro(RJ), Brasil
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}