


Andressa Lumi Akabane; Isabella Parente Almeida; João Carlos Lopes Simão
Introduction: Melasma is a pigmentation disorder that mainly affects women of childbearing age with high phototypes. Polypodium leucotomos has antioxidant, photoprotective and immuno-modulatory activity, and can be considered as an adjunctive treatment for melasma.
Objective: To evaluate the efficacy, in relation to quality of life and objective improvement, of the use of Polypodium leucotomos in the treatment of melasma.
Methods: Prospective and individualized study. Nine volunteers with melasma were submitted to treatment with Polypodium leucotomos for 45 days. MELASQoL, DLQI and MASI scores were calculated at the beginning (D0) and 45 days after (D45). Analysis of variance ANOVA with Tukey post-test for comparison be-tween D0 and D45 (p <0.05).
Results: All patients were females, mean age of 37.18 ± 6.78 years. Family history of melasma in 55.6%; 88.9% with unprotected photoexposure and use of estrogen. After 45 days of treatment with Polypodium leucotomos there was a significant reduction of ME-LASQoL and DLQI (p <0.05) and improvement of MASI in 55.6% of the patients.
Conclusions: There was improvement of MASI in 55.6% of patients after 45 days of treatment. In spite of the slight improvement in MASI, there was a reflex in the improvement of quality of life scores (DLQI and MELASQoL).
Keywords: MELANOSIS; POLYPODIUM; QUALITY OF LIFE; INDICATORS OF QUALITY OF LIFE
Melasma is a pigmentation disorder that affects mainly women of childbearing age with higher phototypes, due to the induced hyperactivation dermal melanocytes, especially by the ultraviolet radiation. It is a frequent condition in the general population, with a high impact in the quality of life.1-3
Polypodium leucotomos (PL), a Polypodiaceae plant extract has antioxidant, photoprotective and immunomodulatory activity, being adjuvant in photoinduced dermatoses, including melasma.1,3
The objective of the study was to evaluate the efficacy in regards to the quality of life, and the objective improvement with the use of PL for the treatment of melasma.
A comparative, prospective and individualized analysis of melasma patients, submitted to a 45-day treatment with PL, conducted according to the ethical procedures advised by the Declaration of Helsinki. Eleven volunteers took one 250mg tablet of PL every 12 hours and continued using sunscreen with an SPF equal to or higher than 50, three times a day. The volunteers did not use any topical products containing acids or bleaching agents in the previous three months. Medical (MELAS- QoL and DLQi and MASI) and photographic assessments (Visia®, Canfeld Imaging System- Fairfeld, EUA) of the volunteers were performed in D0 and D45. The use of the device Visia® enabled a most accurate photographic record of melasma changes through ultraviolet lamps (UV spots), and the device’s digital analysis system enabled the photographic comparison in the different times of the study. The patients signed an informed consent. Two patients were excluded from the study because they were not present in the final assessment.
The photographs were taken in a frontal view, 45° to the right and 45° to the left on days D0 and D45. MELASQoL and DLQI were filled out by the volunteers. MASI was calculated by three collaborating physicians not involved in the study, previously trained, after seeing the photos of the patients, with no knowledge of the time of picture taking (before and after).
For the comparison of the DLQI, MASI and MELAS- QoL scores, the variance analysis Anova was performed with Tukey post-test with a program, GraphPad Prism 7.0.
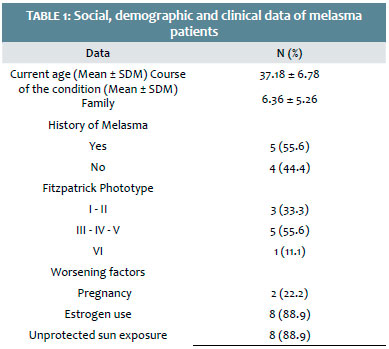
All volunteers were female, with a mean age of 37.18 ± 6.78 years and a mean course of the disease of 6.36 ± 5.26 years. The majority (55.6%) had family history of melasma. In regard to the phototypes, (Fitzpatrick): 33.3% phototypes I-II; 55.6%, III-IV; 11.1%, V-VI (Table 1).
The most prevalent worsening factors for melasma were: unprotected sun exposure (88.9%) and the use of estrogen (88.9%). Worsening of melasma after pregnancy was observed in two of the nine patients (Table 1).
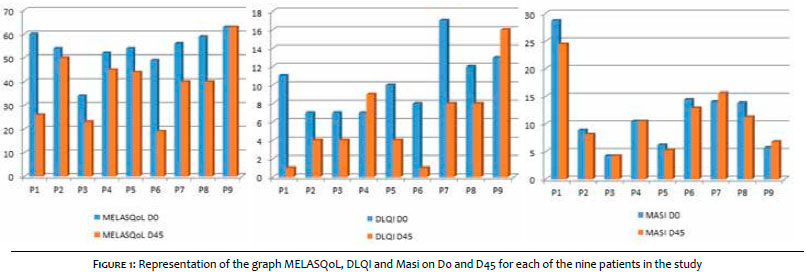
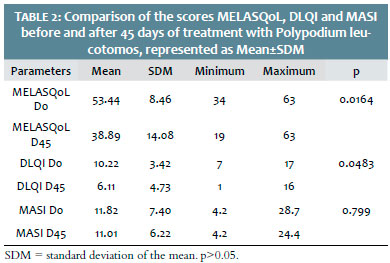
There was a significant reduction in the MELASQoL before and after 45 days using PL (p = 0.0164), as well as a significant decrease in the DLQI score (p = 0.0483). Despite MASI improvement in 55.6% of patients after 45 days of treatment (Figures 1 and 2), overall, there was slight reduction of the mean on D45 (11.01± 6.22) compared to D0 (11.82 ± 7.4). However, there was no statistically significant difference (p = 0.799) (Table 2).
There was a reduction of DLQI and MELASQoL values in seven (77.78%) and eight (88.8%) volunteers, respectively. In regards to MASI values, five (55.55%) patients had a reduction, two (22.2%) had an increase and two (22.2%) kept the same values (Figure 3).
Melasma is more common in females (9:1) and affects 8.8% of Latin women of childbearing age.1 The mean age seen (37.18 years) was similar to other melasma studies.4-6
This condition is particularly prevalent in darker phototypes, especially in Fitzpatrick III to VI.7 In the present study, 66.7% had phototype III-VI and 55.6%, III-IV.
The exact pathogenesis of melasma is not completely clear, being genetics, sun exposure and hormonal therapy possible causal factors.5 The majority (55.6%) had first degree relatives affected; in 88.9% there was unprotected sun exposure and the use of estrogen at some point in life, with worsening of melasma. In 22.2%, pregnancy was a worsening factor.
PL use was associated to improvement of the quality of life, DLQi and MELASQoL scores (p < 0.05). There was improvement in MASI in five (55.6%)of the patients in the study after 45 days of treatment, however, with an overall p > 0.05, with two (22.2%) with higher values and two (22.2%) with the same values upon completion of the study.
Standardized photographic records, such as Visia®, enable better patient follow-up. The comparative analysis of the device’s parameters referring to UV spots and polarized light, was consistent with the evolution of the MASI scores obtained, in the majority of cases. Difficulties such as lack of uniformity of the automatic masking and other concomitant dyschromias can, however, contribute to conflicting scores.
The slight MASI improvement reflected in a significant improvement of the quality of life scores (DLQI and MELAS- QoL). The subjective evaluation of improvement by the patient and by the examiner’s perception reflected independent results, consistent with the low correlation coefficients found between MELASQoL and MASI (0.17 to 0.36) in the literature.4 Similarly, there was a strong correlation of psychometric measures of the perception of the severity of the condition, such as MELASQoL and DLQi.
A slight improvement in MASI improved the quality of life scores significantly (DLQi and MELASQoL) for the patients in the study. The positive results of the adjunctive treatment with PL for melasma favor its use, being a very promising therapeutic alternative. However, new studies with a higher number of patients are needed to best evaluate the efficacy of this drug quantitatively.
Andressa Lumi Akabane:
Clinical evaluation of the patients, preparation of the manuscript, structure of the images and tables
Isabella Parente Almeida:
Clinical evaluation of the patients, preparation of the manuscript, structure of the images and tables
João Carlos Lopes Simão:
Clinical evaluation of the patients, supervision, preparation and proof-reading of the manuscript
1. Miot LDB, Miot HA, da Silva MG, Marques MEA. Pathophisiology of melasma. An Bras Dermatol. 2009; 84(6):623-35.
2. Calzavara- Pinton PG, Rossi MT, Zanca A, Arisi M, Gonzalez S, Venturini M. Oral Polypodium Leucotomos increases anti-inflammatory and melanogenic responses of the skin to different modalities of sun exposures: a pilot study. Photodermatol Photoimmunol Photomed. 2016 Jan; 32(1):22-7.
3. Costa A, Moises TA, Cordero T, Alves CRT, Marmiori J. Associação de emblica, licorice e belides como alternativa à hidroquinona no tratamento clínico do melasma. An Bras Dermatol. 2010;85(5):613-20.
4. Lieu TJ, Pandya AG. Melasma Quality of Life Measures. Dermatol Clin. 2012;30:269-280.
5. Maranzatto CFP, Miot LDB, Miot HA, Meneguin S. Análise psicométrica e estrutura dimensional da versão brasileira da escala de qualidade de vida em melasma (MELASQoL- BP). An Bras Dermatol. 2016;91(4):422-8.
6. Lee HC, Thng TGS, Goh CL. Oral tranexamic acid in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol, 2016.75(2):385-392.
7. Kim JY, Choi M, Nam CH, Kim JS, Kim MH, Park BY, Hong SP. Treatment of Melasma with THE photoacoustic twin pulse mode of low-fluence 1064 nm Q-switched Nd:YAG Laser. Ann Dermatol. 2016;28(3):290-296.
Study conducted at the Division of Dermatology, Department of Internal Medicine, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo - São Paulo(SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}