


Guilherme Bueno de Oliveira1; Natália Cristina Pires Rossi2; Doramarcia de Oliveira Cury1; Maria Gabriela Gonçalves Coura3; Carlos Roberto Antonio4
Introduction: Tuberous sclerosis is a dominant autosomal genodermatosis, classically characterized by facial angiofibromas, fibrotic plaques, periungual fibromas, leaf-shaped hypochromic maculae and fibrous frontal plaques.
Case report: A patient bore this disease, with Koenen tumors in all nail beds of hands and feet, which were resistant to the conventional treatment — simple excision and electrosurgery. Amputation of the nail beds was performed followed by reconstruction with full thickness skin grafts.
Conclusion: The amputation of the nail apparatus and reconstruction with full thickness skin grafts in aggressive, recurrent or high morbidity cases can be an effective therapeutic option.
Keywords: DERMATOLOGY; DERMATOLOGIC SURGICAL PROCEDURES; TUBEROUS SCLEROSIS; SKIN TRANSPLANTS
Koenen tumors (KT) are a characteristic and one of the major criteria for the diagnosis of tuberous sclerosis complex (TSC). It usually appears after puberty in up to 50% of patients with TSC.1
TSC is an autosomal dominant genodermatosis classically characterized by facial angiofibromas, fibrotic plaques (Shagreen patch), periungual fibromas (KT), hypochromic leaf-shaped macules (ash leaves) and fibrous frontal plaque.1,2 Seizure, mental retardation, hamartomas of the retina, subependymal nodules and hamartomas of the internal organs are common associations.3 Half the families with TSC are linked to the 9q34 chromosome, with inactivating mutations of the tumor suppressor genes of the protein hamartin (TSC1) and the other half to the 16p13 chromosome with inactivating mutations of the tumor suppressor genes of the protein tuberin (TSC2). The hamartin/ tuberin complex is an important inhibitor of tumor growth and its absence triggers the loss of inhibition over cell proliferation and migration.1-3
This study has the objective of demonstrating an unusual presentation and multiple florid KT, that were surgically treated.
We report the case of a 47-year-old female patient with a history of hypochromic, lenticular, confetti-like and leaf-shaped (ash leaves) lesions on her body since the first decade of life, progressing with papular lesions on the face (angiofibromas) and peduncular keratotic confluent lesions in all nail beds of both feet and hands (KTs), that were bigger in size but morphologically similar to periungual viral warts. She also had recurrent seizures.
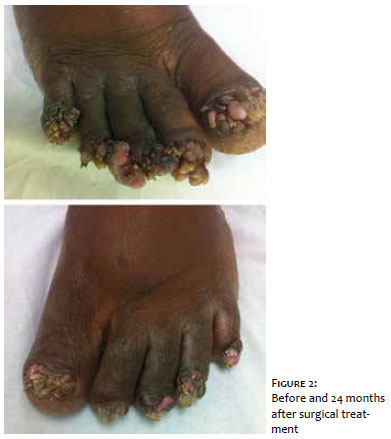
The patient complained of pain in the toes and recurrent local infections, difficulty in walking and putting on shoes due to the lesions on the area. Multiple sessions of electrosurgery and simple excision were performed, but the lesions always recurred in less than 2 months of follow up. Because of the clinical picture’s exuberance and morbidity, we opted to amputate all nail beds and reconstruct them with full thickness skin grafts (Figure 1). After 24 months of follow up, the patient remains with no lesions (Figure 2), with complete control of local pain and infections.
KT are periungual or subungual fibromas manifested as pink or skin-colored papules and nodules, that can be multiple and affect mainly the toes. On histology, they are characterized by stellate fibroblasts and dense collagen, with numerous ectatic blood vessels.1,4
They usually vary between 5 to 10 mm in size, but can be much larger. This can be the only clinically obvious abnormality in 50% of TSC cases. The first tumors appear between 12 and 14 years of age, and progressively enlarge in number and in size with age. They sometimes become keratotic, similar to a fibrokeratoma or, more rarely and with few reports in the literature, to periungual viral warts.1,2,4 In this case, the patient had a florid clinical picture, with elongated, keratotic and confluent fibromas, similar to viral warts. The tumors were so aggressive that they basically replaced the nail plate in most toes, leading to local pain, recurrent skin infections, difficulty in walking and in putting on shoes.
Various treatment techniques such as dermabrasion, chemical ablation, excision and laser ablation have been described in the literature with variable results in regard to duration, and there is still no consensus on a standard treatment. Recurrence is the norm.5 Amputation of the nail apparatus and reconstruction with a full thickness skin graft can have removed the local stimulus for tumor formation, what explains the effectiveness of the therapeutic choice and lack of recurrence in all toes, despite the aggressiveness of the condition.
Amputation of the nail apparatus and reconstruction with full thickness skin graft for aggressive, recurrent or high morbidity cases of KT in patients with TSC can be an effective therapeutic option. More cases are needed with reports in the literature to confirm this hypothesis.
Guilherme Bueno de Oliveira
Dermatologic surgeon responsible for the surgery
Final version and approval of the manuscript Study planning
Critical literature and manuscript review
Natália Cristina Pires Rossi
Primary surgical assistant
Literature review
Writing of the manuscript
Carlos Roberto Antonio
Dermatologic surgeon responsible for the surgery
Final version and approval of the manuscript Study planning
Revisão crítica da literatura e do manuscrito
Maria Gabriela Gonçalves Coura
Secondary surgical assistant Literature review Writing of the manuscript
Doramarcia de Oliveira Cury
Final version and approval of the manuscript Study planning
Critical literature and manuscript review
Post-operative follow up
1. Rodrigues DA, Gomes CM, Costa IMC. Esclerose tuberosa. An Bras Dermatol. 2012; 87(2):185-97.
2. Ortonne JP, Bahadoran P, Fitzpatrick TB, Mosher DB, Hori Y. Hypomelanoses and hypermelanoses. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick's dermatology in general medicine. 6th ed. New York City: McGraw-Hill Professional; 2003. p. 850-3.
3. Devi B, Dash M, Behera B, Puhan MR. Multiple koenen tumors: an uncommon presentation. Indian J Dermatol. 2011;56(6):773-5.
4. Quist SR, Franke I, Sutter C, Bartram CR, Gollnick HP, Leverkus M. Periungual fibroma (Koenen tumors) as isolated sign of tuberous sclerosis complex with tuberous sclerosis complex 1 germline mutation. J Am Acad Dermatol. 2010;62(1):159-61.
5. Liebman JJ, Nigro LC, Matthews MS. Koenen tumors in tuberous sclerosis: a review and clinical considerations for treatment. Ann Plast Surg. 2014;73(6):721-2.
Study conducted at Faculdade de Medicina Estadual de São José do Rio Preto (Famerp) – São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}