


Felipe Bochnia Cerci1,2
Introduction: The cutaneous upper lip is often affected by malignant skin neoplasms. Surgical treatment is preferred for most lesions in this site. Whenever available, tumors in the perioral area should be managed with Mohs micrographic surgery.
Case report: The author of the present article describes the implementation of a rotation flap in the cutaneous upper lip of a patient who underwent Mohs micrographic surgery.
Discussion: There are a number of options for repairing surgical defects in the cutaneous upper lip. When primary closure is not possible, rotation flaps are considered because they allow camouflaging of the rotation arc in the nasolabial fold, and the other incisions in the perioral rhytids.
Keywords: LIP NEOPLASMS; MOHS SURGERY; SURGICAL FLAPS
The upper cutaneous lip is frequently affected by malignant neoplasms of the skin. Surgical treatment is preferred for most lesions on this region. Whenever available, Mohs micrographic surgery should be considered for this area, since the technique enables assessment of 100% of the surgical margins, besides saving healthy tissue.1
Surgical wounds in the upper cutaneous lip can be challenging to repair. The complexity of the wounds affecting this anatomical region is due to the proximity to multiple cosmetic subunits, its respective boundaries and to the fact that the lip is a free margin. An ideal reconstruction restores the color, texture and maintains the symmetry of the cupid’s bow, philtrum, apical triangles, nasolabial fold and free margin of the lip, besides camouflaging incisions between anatomical subunits.2
There are many upper cutaneous lip repair options available according to the location, size, depth, elasticity and involvement of adjacent structures.3,4 The case of a patient who underwent a rotation flap for repair of the upper cutaneous lip after Mohs micrographic surgery is described.
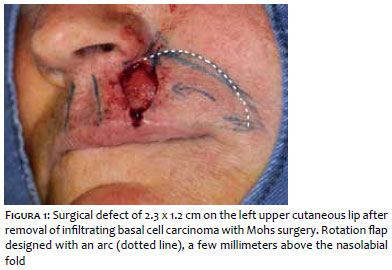
Fifty-year-old female patient came to the Department of Dermatology with a pearly erythematous plaque measuring 1.3 x 0.9 cm in the left upper cutaneous lip. Biopsy revealed an infiltrating basal cell carcinoma. The patient underwent Mohs surgery under local anesthesia (lidocaine and bupivacaine) reaching the free margins after two stages. The resulting defect measured 2.1 x 1.3 cm, affecting the left upper cutaneous lip (Figure 1). The underlying muscles were spared.
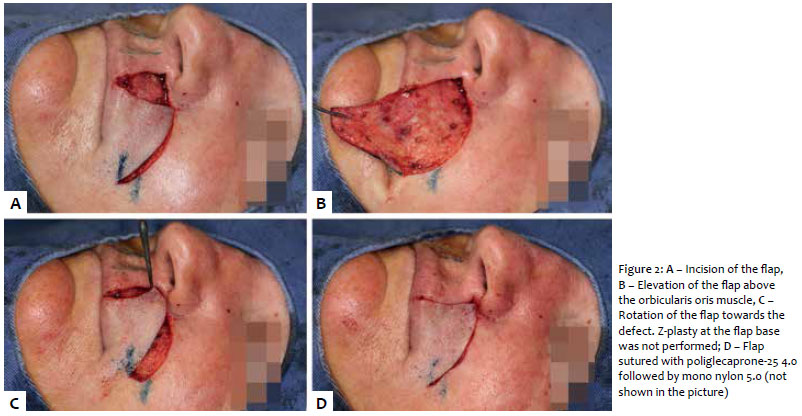
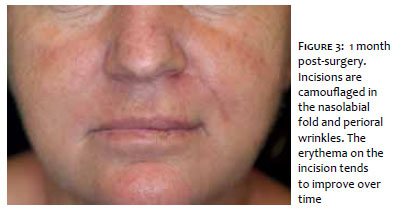
Due to the size and location of the wound, a rotation flap was chosen for the repair (Figure 1). The rotation arc was drawn a few millimeters above the nasolabial fold. The defect edges were initially angulated, and the defect was extended to the inferior edge of the nose to camouflage the incisions. The flap was elevated and undermined above the orbicularis oris muscle in the perioral region and in the subcutaneous tissue close to the nasolabial fold. After hemostasis, the flap was positioned and sutured in two levels, with poliglecapronae-25 4.0 and mono nylon 5.0 (Figure 2). The external sutures were removed after 7 days. After 1 month, the surgical incisions were camouflaged within the inferior edge of the nose, the perioral wrinkles and nasolabial fold (Figure 3).
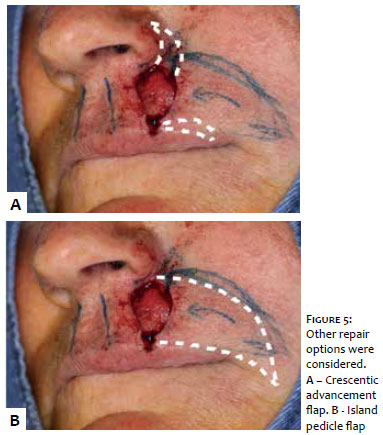
There are many repair options for the upper cutaneous lip. Primary closure is the ideal option when possible, with the longer axis of the ellipse positioned over the perioral relaxed skin tension lines, which tend to be perpendicular and diagonal to the horizontal lip axis.3 Although it is possible to perform an M-plasty to reduce the size of the closure and to avoid going over the vermillion line, its involvement is usually not a problem as long as the vermillion borders are adequately aligned. It is better to advance to the vermillion border than to use a short ellipse and create a bulge or dog ear on the lip. Primary closures must be observed and avoided for they can generate tension that shift the inferior lip upon closure.5 Every time that a considerable distortion is observed during primary closure such as in this case (Figure 4), other repair methods must be considered (Figure 5).
Advancement flaps are useful for the repair of surgical wounds in the lateral region of the upper cutaneous lip because of the great amount of skin adjacent to the medial malar region. These flaps are usually designed along the vermillion border and the excessive tissue is removed in the relaxed skin tension lines of the perioral region. Redundant skin can be removed with Burrow triangles or crescents as to minimize the risk of vermillion distortion.6 When the defect is located on the superior part of the upper cutaneous lip, the flap should be designed extending into the inferior nasal edge and removing a crescent adjacent to the nasal ala, as described by Webster, and the redundant inferior skin removed in the perioral relaxed skin tension lines.7
Another repair option for the defects on the superior part of the upper cutaneous lip are the rotation flaps, as shown in this case. The advantage of this option is the possibility of camouflaging the rotation arc in the nasolabial fold. The arc can be designed a few millimeters above the nasolabial fold since the malar region will shift medially as the flap rotates. The vertical incision of the flap is camouflaged in the perioral relaxed skin tension lines.4
Similarly, the island pedicle flap is useful for the repair of the upper cutaneous lip defects. Many of the incisions can be camouflaged in the nasolabial fold and inferior nasal edge. Care must be taken to avoid tension in the vermillion border by undermining the flap adequately.8
Transposition flaps can be useful for defects in this location when advancement or rotation flaps do not move satisfactory amount of tissue. The incisions can be partially camouflaged in the nasolabial fold. However, a disadvantage is the increased chance of trap door. Besides, transposition flaps in this location tend to obliterate the nasolabial fold more than the advancement or rotation flaps. Skin grafts are rarely used in this area due to the inadequate final color and texture.9
In this case, the rotation flap was performed with satisfactory results. There was no distortion and the incisions were camouflaged in the anatomical units or subunits.
Felipe Bochnia Cerci
Intellectual participation in the propaedeutic and /or therapeutic conduct of studied cases
Data collection, analysis and interpretation
Study design and planning
Approval of the final version of the manuscript
1. Hafiji J, Hussain W, Salmon P. Reconstruction of perioral defects post-Mohs micrographic surgery: a dermatological surgeon's approach. Br J Dermatol. 2015;172(1):145-50.
2. Holmes TE. Crescentic apical triangle island pedicle flap for repair of the medial upper lip. Dermatol Surg. 2013;39(5):784-8.
3. Zitelli JA, Brodland DG. A regional approach to reconstruction of the upper lip. J Dermatol Surg Oncol. 1991;17(2):143-8.
4. Krunic AL, Weitzul S, Taylor RS. Advanced reconstructive techniques for the lip and perioral area. Dermatol Clin. 2005;23(1):43-53.
5. Kaufman AJ, Rohrer TE. Novel flaps for lip reconstruction. Skin Therapy Lett. 2006;11(6):4-9.
6. Lopiccolo MC, Kouba DJ. Bilateral peri-alar advancement flap to close a midline upper lip defect. Dermatol Surg. 2011;37(8):1159-62.
7. Webster JP. Crescentic peri-alar cheek excision for upper lip flap advancement with a short history of upper lip repair. Plast Reconstr Surg. 1955;16(6):434-64.
8. Griffin GR, Weber S, Baker SR. Outcomes following V-Y advancement flap reconstruction of large upper lip defects. Arch Facial Plast Surg. 2012;14(3):193-7.
9. Vasyukevich K, Zimbler MS. O to Z reconstruction of central upper lip defect. Dermatol Surg. 2007;33(1):85-7; discussion 87-9.
Study conducted at the Department of Dermatology at Hospital Santa Casa de Curitiba and at the Department of Dermatology at Hospital de Clínicas of the Universidade Federal do Paraná – Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}