


Lina Andrea Gómez1; Valentina Casas Romero2; William Hernando Merchan Rubiano2
Introduction: Acne is a multifactorial disease where inflammatory lesions usually appear as papules, pustules and comedones. It is more common in people aged between 11 and 30 years, and occurs in various body sites where there are high concentrations of pilosebaceous glands. Acne has different classifications and treatments. More recently, platelet growth factors have been used as an alternative therapy for acne scars.
Objective: The present study is aimed at describing a case of nodule-cystic acne and acne scars Grades 1, 2 and 3b treated with platelet rich plasma and highlighting the effectiveness of the treatment.
Methods: Platelet rich plasma was applied for three months in the left side of the face of a patient bearing acne.
Results: In the clinical and photographic evaluations, there was improvement in the skin appearance and quality, less number of lesions and decrease of pain.
Conclusions: The present study has demonstrated the effectiveness of platelet rich plasma as a treatment for acne and resulting scars.
Keywords: PLATELET-RICH PLASMA; ACNE VULGARIS; CICATRIX
Acne is a multifactorial disease in which the inflammatory lesions arise in the form of papules, pustules and comedones. It is most common in people aged between 11 and 30 years, and can occur in many regions of the body, usually where there are high concentrations of pilosebaceous units.1-3. There are different classification systems that assist in the diagnosis of its severity. One of the most relevant is that created by the Latin American Group for the Study of Acne (Glea - Grupo Latino-Americano para o Estudo da Acne), which uses four classification categories. The first category regards the patient’s age (it can be neonatal acne if arising during the first 30 days of life; infant acne, when it arises between the first month and the second year of life; childhood acne, if it emerges between two and seven years of age; pre-adolescence acne if it occurs between eight and 11 years of age; adolescence acne, if arising between 12 and 24 years of age; and the adult acne if it occurs after the age of 25. The second category is based on the predominant type of lesion (comedonian, which can refer to open, closed or both types of lesions; papulopustular, when the predominant lesions are papules and pustules; and nodule-cystic, characterized by deep inflammatory lesions that can leave severe scars or cases that extend to the cervical region and trunk. The third category classifies the acne according to its degree of severity (mild, moderate or severe); while the fourth and last category includes special forms (such as acne conglobata and fulminans, which share some characteristics of acne vulgaris, nevertheless present the possibility of systemic compromise).4,5 Acne's inflammatory lesions lead to permanent complications, such as scars, which in 95% of the cases are located on the face.1,6 These scars, which worsen with age, may have psychosocial implications that manifest as low self-esteem, sadness, anger and even embarrassment.6,7 Epidemiological data on these acne scars are not very clear, however it is estimated that they occur in 95% of patients with acne.8
The pathophysiology of scars caused by acne has been associated with loss or overproduction of collagen due to the presence of an imbalance in the reorganization phase of the tissue’s architecture, when fibroblasts and keratinocytes produce enzymes such as metalloproteinases, which are responsible for the remodeling of damaged tissue. 7-9
Scars can be classified as atrophic or hypertrophic, when there is loss or overproduction of collagen, respectively. Atrophic scars are more common and can be sub-classified into icepick, rolling and box depending on their width, depth and shape. Another scar classification system is the Goodman and Baron scale, which can attribute one of four grades to the lesions: 1,7,8 Grade 1 corresponds to the macular disease, in which erythematous macules, which may be hyperpigmented and hypopigmented, can be observed; Grade 2 corresponds to a mild degree of the disease, characterized by atrophic and hypertrophic scars that are barely visible and easy to conceal with makeup; Grade 3 refers to a moderate degree of the disease, in which atrophic and hypertrophic scars are more visible and not easily concealed by makeup, however they become imperceptible with the distension of the skin; the fourth grade represents the most serious picture, in which scars can not be easily hidden.10
These scars are known as sequelae from acne and can become permanent and difficult to treat. Its psychosocial implications are a priority in the treatment of patients with acne.1,10 There are a variety of treatments, such as chemical dermabrasion, laser, lipografting and cutaneous filling based treatments. Nonetheless, all these treatments offer limited results, and some lead to negative side effects.11 There are topical treatments, such as retinoids (e.g. adapalene), isotretinoin, antimicrobials (e.g. benzoyl peroxide and azelaic acid), and systemic therapies, such as those performed with retinoids, steroid and non-steroidal hormones, and antibiotics.2
Platelet-rich plasma (PRP) is a fraction of blood with a high platelet concentration (above the baseline concentration of 150,000-350,000/µl).11 Platelets contain growth factors that are secreted by platelet granules and include transforming growth factors (TGFs), platelet-derived growth factors (PDGFs), vascular endothelial growth factor (VEGF), platelet-derived endothelial growth factor (PDEGF), insulin-like growth factor (IGF), epithelial cells growth factor (ECGF), platelet-derived angiogenesis factor (PDAF), platelet factor 4 (PF4) and other molecules with important roles in healing, including cell proliferation, migration and differentiation, collagen synthesis, granulation tissue formation and angiogenesis. 6,10,11
It has been observed that PRP can smooth the scars, resulting in a better appearance regardless of skin tone. The PRP’s mechanism of action in the scars consists of causing mild inflammation, which triggers the healing cascade and the production of growth factors that help to form new vessels (angiogenesis) for tissue repair. Thanks to this process, the new collagen develops and matures, becoming elastic, lending the smoothness appearance to the scars.11 The advantages of PRP lies in the fact that it is an autologous product, excluding the possibilities of treatment rejection and the necessity for a donor, as well as any transmissible infection. However, there are some contraindications, such as presence of cancer, chemotherapy, platelet dysfunction syndrome, critical thrombocytopenia, anticoagulation therapy and others. Side effects include pain, bruising and cutaneous dyschromias, which usually disappear shortly after the application.3
The purpose of the present pilot study is to describe the case of patient with nodule-cystic acne and acne scars Grade 1, 2 and 3b treated with PRP, at the same time highlighting the effectiveness of the treatment.
The application of PRP in the studied patient, who signed a Term of Consent, was approved by the Ethics Committee of the Antonio Nariño University, Bogotá, Colombia. A patient with the following characteristics was chosen for the study: male, 21 years of age, having bore moderate papulopustular acne (GLEA), affected by inflammatory papules, pustules and cysts for three years. According to the Goodman and Baron scale,12 the patient had Grade 1 erythematous cutaneous lesions in the face and neck, Grade 2 atrophic scars in the face, and Grade 3b atrophic scars in the neck and face. The right hand side of the patient’s, which was not treated with PRP, had mild papulopustular acne and Grade 1 and 2 scars on the face and neck region. The patient had not received other treatments prior to the application of PRP.
Preparation of PRP
The PRP was collected in a hospital setting, according to a protocol previously standardized by the researchers: 49.5 ml of venous blood sample were harvested from the cephalic vein and transferred to tubes containing 0.5 ml of sodium citrate (Vacutainer® Ref 369714; BD Biosciences). One of the tubes was reserved for the baseline platelet count. The remaining samples were centrifuged for 10 minutes at 240g, 20ºC (Thermos-cientific Sorvall ST16 centrifuge). Approximately 8 ml of PRP were obtained with this process. Ten percent (10%) calcium gluconate were added in order to activate the platelets.
Procedure
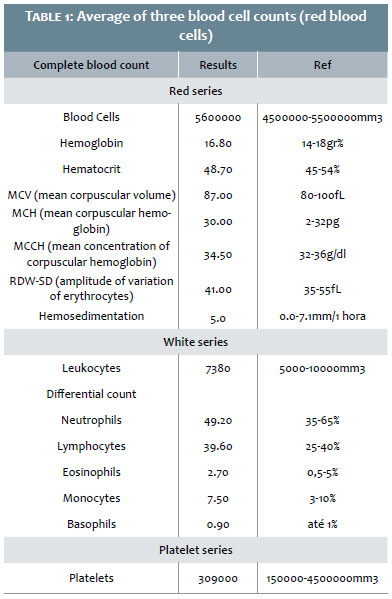
Aimed at partially alleviating pain, approximately 90 minutes before starting the application, the target region was treated with topical anesthetic cream Roxicaina® 2% (lidocaine hydrochloride, Ropsohn, Colombia), followed by gentle cleansing with distilled water. According to the study’s centrifugation protocol, it was possible to increase the concentration of the basal platelets by 2.8 times, resulting in the use of about 865,000pl/ul (baseline platelet count = 309,000pl ul).13 Blood cell counts were performed in each blood sample, on each application (Table 1). The injection sites were determined observing 1cm intervals, with the application of 0.5ml of autologous platelet-rich plasma on the left side of the face and neck. Multiple sub-dermal injections were performed, with minimal erythema and edema being obsereved for up to three hours after treatment. No analgesic drugs or ice were used after the treatment. The patient was instructed to avoid direct exposure to the sunlight during the treatment and use wide spectrum SPF 50 sunscreen daily. The patient underwent 3 treatments with intervals of 1 month between each session.
The papules, pustules and comedones decreased in number and size, with marked improvement in the cervical region. On the treated side, the papules and pustules improved from moderate to mild after treatment, while on the untreated side, the improvement was negligible. The appearance of the skin improved due to improvements in the depth and dimensions of the scars. The skin became smoother and more uniform in appearance and on palpation. Grade 1 erythematous cutaneous lesions in the face and cervical region almost completely disappeared, and Grade 2 lesions in the face and Grade 3b in the face and cervical region decreased significantly (Figure 1). The clinical and photographic evaluations were performed 30 days after the last PRP session. The patient reported intense satisfaction with the results, including decreased skin lesions, improved skin quality and less pain.
Acne is a condition with physical and psychological implications resulting from dermatological disorders manifested in highly visible body areas, such as the face. Some recent studies have assessed the treatment of acne with autologous PRP in combination with other therapies, which entailed difficulty in evaluating the intrinsic performance of PRP as an isolated treatment for acne.
In the present study, the authors used PRP as an isolated therapy, observing a significant decrease in the size and number of papules. In addition, pain reduction and better healing were achieved. Similar studies have used PRP in combination with other therapies (e.g. antibiotic therapy), also improving the patient's condition, reducing the risk of superinfection of primary skin lesions, papules and comedones.6 The use of autologous PRP obtained in sterile conditions, coupled with a standardized methodology, can become a safe and effective alternative to treat conditions like acne. It is important to conduct studies with more patients and similar conditions in order to determine outcomes that will contribute to its implementation.
Platelet rich plasma is a good choice for the treatment of acne and atrophic scars reminiscent of the course of the disease. In addition, for being autologous, it reduces the possibility of side effects, such as skin dryness and rejection. It was demonstrated that PRP accelerates the healing process, regulates inflammation and promotes healing by inhibiting the P. acnes bacteria, additionally restoring collagen.7,10,2 The PRP’s mechanism of action also involves the release of powerful antimicrobial peptides from the platelets' alpha granules. Although there are few studies on the PRP's effectiveness in acne, it emerges as a potential therapeutic option in Dermatology and Aesthetic Medicine.
Lina Andrea Gómez
Study conception; collection, processing and application of PRP in the patient; data collection and analysis; manuscript preparation; translation into English.
Valentina Casas Romero
Preparation of the Discussion Section in Spanish; translation into English, preparation of the Introduction Section (patient description and classification of the patient's scars).
William Hernando Merchan Rubiano
Preparation of Table 1, preparation of the Discussion Section in Spanish, processing of the Figure 1, preparation of the Introduction Section, patient description (classification of the patient’s acne and scars in Spanish).
1. Chawla S. Split face comparative study of microneedling with prp versus microneedling with vitamin c in treating atrophic post acne scars. J Cutan Aesthet Surg. 2014;7(4):209-12.
2. Morales N, Aristizábal AM. Cicatrices de acné , un reto terapéutico. Rev Asoc Colomb Dermatol. 2013;21(4):328-36.
3. Zhu JT, Xuan M, Zhang YN, Liu HW, Cai JH, Wu YH, et al. The efficacy of autologous platelet-rich plasma combined with erbium fractional laser therapy for facial acne scars or acne. Mol Med Rep. 2013;8(1):233-7.
4. Kaminsky A, Florez-White M. Clasificación. In: Kaminsky A, Florez-White M. Acné: un enfoque global. Buenos Aires: Alfaomega Grupo Editor Argentino; Colegio Ibero Latinoamericano de Dermatología; 2012. p. 59-66.
5. Kaminsky A, Florez-White M, Arias MI, Bagatin E. Clasificación del acné: Consenso Ibero-Latinoamericano, 2014. Med Cutan Iber Lat Am. 2015;43(1):18–23.
6. Faghihi G, Keyvan S, Asilian A, Nouraei S, Behfar S, Nilforoushzadeh M. Efficacy of autologous platelet-rich plasma combined with fractional ablative carbon dioxide resurfacing laser in treatment of facial atrophic acne scars: A split-face randomized clinical trial. Indian J Dermatol Venereol Leprol. 2016;82(2):162-8.
7. Flores GG, Morice WM. Tratamiento del acné. Rev Med Costa Rica y Centroam. 2012;69(600):91-7.
8. Fabbrocini G, De Vita V, Cozzolino A, Marasca C, Mazzella C, Monfrecola A. The Management of Atrophic Acne Scars: Overview and New Tools. J Clin Exp Dermatol Res. 2012;S5.
9. Intravia J, Allen DA, Durant TJ, McCarthy MB, Russell R, Beitzel K, et al. In vitro evaluation of the anti-bacterial effect of two preparations of platelet rich plasma compared with cefazolin and whole blood. Muscles Ligaments Tendons J. 2014;4(1):79-84.
10. Goodman GJ, Baron JA. Postacne scarring: a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458-66.
11. Langer C, Mahajan V. Platelet-rich plasma in dermatology. JK Sci. 2014;16(4):147-50.
12. Puri N. Platelet rich plasma in dermatology and aesthetic medicine. Our Dermatol Online. 2015;6(2):207-11.
13. Gómez LA, Escobar M, Peñuela O. Standardization of a protocol for obtaining platelet rich plasma from blood donors; a tool for tissue regeneration procedures. Clin Lab. 2015;61(8):973-80.
This study was carried out at the Universidade Antonio Nariño (UAN) - Bogotá, Colombia.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}